Get your patient on Lotemax Sm (Loteprednol Etabonate)
Lotemax SM patient education
Patient toolkit
Dosage & administration

Lotemax SM prescribing information
INDICATIONS AND USAGE
LOTEMAX ® SM (loteprednol etabonate ophthalmic gel) 0.38% is a corticosteroid indicated for the treatment of post-operative inflammation and pain following ocular surgery.
DOSAGE AND ADMINISTRATION
Invert closed bottle and shake once to fill tip before instilling drops. Apply one drop of LOTEMAX ® SM into the conjunctival sac of the affected eye three times daily beginning the day after surgery and continuing throughout the first 2 weeks of the post-operative period.
DOSAGE FORMS AND STRENGTHS
LOTEMAX ® SM (loteprednol etabonate ophthalmic gel) 0.38% is a sterile preserved ophthalmic gel containing 3.8 mg of loteprednol etabonate per gram of gel.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no adequate and well controlled studies with loteprednol etabonate in pregnant women.
Loteprednol etabonate produced teratogenicity at clinically relevant doses in the rabbit and rat when administered orally during pregnancy. Loteprednol etabonate produced malformations when administered orally to pregnant rabbits at doses 4.2 times the recommended human ophthalmic dose (RHOD) and to pregnant rats at doses 106 times the RHOD. In pregnant rats receiving oral doses of loteprednol etabonate during the period equivalent to the last trimester of pregnancy through lactation in humans, survival of offspring was reduced at doses 10.6 times the RHOD. Maternal toxicity was observed in rats at doses 1066 times the RHOD, and a maternal no observed adverse effect level (NOAEL) was established at 106 times the RHOD.
The background risk of major birth defects and miscarriage for the indicated population is unknown. However, the background risk in the U.S. general population of major birth defects is 2 to 4%, and of miscarriage is 15 to 20%, of clinically recognized pregnancies.
Data
Animal Data
Embryofetal studies were conducted in pregnant rabbits administered loteprednol etabonate by oral gavage on gestation days 6 to 18, to target the period of organogenesis. Loteprednol etabonate produced fetal malformations at 0.1 mg/kg (4.2 times the recommended human ophthalmic dose (RHOD) based on body surface area, assuming 100% absorption). Spina bifida (including meningocele) was observed at 0.1 mg/kg, and exencephaly and craniofacial malformations were observed at 0.4 mg/kg (17 times the RHOD). At 3 mg/kg (128 times the RHOD), loteprednol etabonate was associated with increased incidences of abnormal left common carotid artery, limb flexures, umbilical hernia, scoliosis, and delayed ossification. Abortion and embryofetal lethality (resorption) occurred at 6 mg/kg (256 times the RHOD). A NOAEL for developmental toxicity was not established in this study. The NOAEL for maternal toxicity in rabbits was 3 mg/kg/day.
Embryofetal studies were conducted in pregnant rats administered loteprednol etabonate by oral gavage on gestation days 6 to 15, to target the period of organogenesis. Loteprednol etabonate produced fetal malformations, including absent innominate artery at 5 mg/kg (106 times the RHOD); and cleft palate, agnathia, cardiovascular defects, umbilical hernia, decreased fetal body weight and decreased skeletal ossification at 50 mg/kg (1066 times the RHOD). Embryofetal lethality (resorption) was observed at 100 mg/kg (2133 times the RHOD). The NOAEL for developmental toxicity in rats was 0.5 mg/kg (10.6 times the RHOD). Loteprednol etabonate was maternally toxic (reduced body weight gain) at 50 mg/kg/day. The NOAEL for maternal toxicity was 5 mg/kg.
A peri-/postnatal study was conducted in rats administered loteprednol etabonate by oral gavage from gestation day 15 (start of fetal period) to postnatal day 21 (the end of lactation period). At 0.5 mg/kg (10.6 times the clinical dose), reduced survival was observed in live-born offspring. Doses ≥ 5 mg/kg (106 times the RHOD) caused umbilical hernia/incomplete gastrointestinal tract. Doses ≥ 50 mg/kg (1066 times the RHOD) produced maternal toxicity (reduced body weight gain, death), decreased number of live-born offspring, decreased birth weight, and delays in postnatal development. A developmental NOAEL was not established in this study. The NOAEL for maternal toxicity was 5 mg/kg.
Lactation
There are no data on the presence of loteprednol etabonate in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered, along with the mother’s clinical need for LOTEMAX ® SM and any potential adverse effects on the breastfed infant from LOTEMAX ® SM.
Pediatric Use
Safety and effectiveness of LOTEMAX ® SM in pediatric patients have not been established.
Geriatric Use
No overall differences in safety and effectiveness have been observed between elderly and younger patients.
CONTRAINDICATIONS
LOTEMAX ® SM, as with other ophthalmic corticosteroids, is contraindicated in most viral diseases of the cornea and conjunctiva including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, in mycobacterial infection of the eye and fungal diseases of ocular structures.
WARNINGS AND PRECAUTIONS
- Intraocular pressure (IOP) increase - Prolonged use of corticosteroids may result in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. If this product is used for 10 days or longer, IOP should be monitored. ()
- Cataracts - Use of corticosteroids may result in posterior subcapsular cataract formation. (5.2 )
- Delayed healing – The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation. In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids. The initial prescription and renewal of the medication order should be made by a physician only after examination of the patient with the aid of magnification such as slit lamp biomicroscopy and, where appropriate, fluorescein staining. (5.3 )
- Bacterial infections – Prolonged use of corticosteroids may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions, steroids may mask infection or enhance existing infection. (5.4 )
- Viral infections – Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution. Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex). (5.5 )
- Fungal infections – Fungal infections of the cornea are particularly prone to develop coincidentally with long-term local steroid application. Fungus invasion must be considered in any persistent corneal ulceration where a steroid has been used or is in use. (5.6 )
Intraocular Pressure (IOP) Increase
Prolonged use of corticosteroids may result in glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision. Steroids should be used with caution in the presence of glaucoma. If this product is used for 10 days or longer, intraocular pressure should be monitored.
Cataracts
Use of corticosteroids may result in posterior subcapsular cataract formation.
Delayed Healing
The use of steroids after cataract surgery may delay healing and increase the incidence of bleb formation. In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical steroids. The initial prescription and renewal of the medication order should be made by a physician only after examination of the patient with the aid of magnification such as slit lamp biomicroscopy and, where appropriate, fluorescein staining.
Bacterial Infections
Prolonged use of corticosteroids may suppress the host response and thus increase the hazard of secondary ocular infections. In acute purulent conditions of the eye, steroids may mask infection or enhance existing infection.
Viral Infections
Employment of a corticosteroid medication in the treatment of patients with a history of herpes simplex requires great caution. Use of ocular steroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex).
Fungal Infections
Fungal infections of the cornea are particularly prone to develop coincidentally with long-term local steroid application. Fungus invasion must be considered in any persistent corneal ulceration where a steroid has been used or is in use. Fungal cultures should be taken when appropriate.
Contact Lens Wear
Contact lenses should not be worn when the eyes are inflamed.
ADVERSE REACTIONS
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse reactions associated with ophthalmic steroids include elevated intraocular pressure, which may be associated with infrequent optic nerve damage, visual acuity and field defects, posterior subcapsular cataract formation, delayed wound healing and secondary ocular infection from pathogens including herpes simplex, and perforation of the globe where there is thinning of the cornea or sclera.
There were no treatment-emergent adverse drug reactions that occurred in more than 1% of subjects in the three times daily group compared to vehicle.
DESCRIPTION
LOTEMAX ® SM (loteprednol etabonate ophthalmic gel) 0.38% contains a sterile, topical corticosteroid for ophthalmic use. Loteprednol etabonate is a white to off-white powder.
Loteprednol etabonate is represented by the following structural formula:
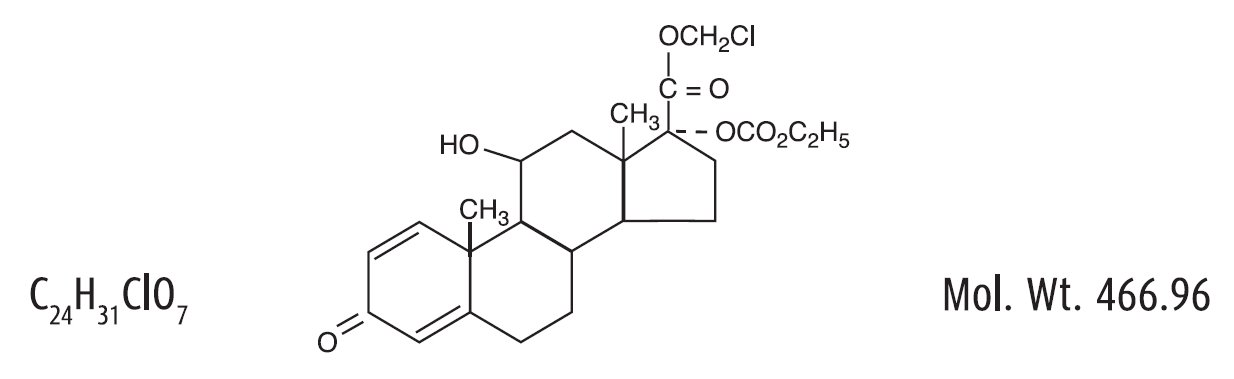
Chemical Name:
chloromethyl 17α-[(ethoxycarbonyl)oxy]-11β-hydroxy-3-oxoandrosta-1,4-diene-17β-carboxylate
Each gram contains:
- Active: loteprednol etabonate 3.8 mg (0.38%);
- Inactives: boric acid, edetate disodium dihydrate, glycerin, hypromellose, poloxamer, polycarbophil, propylene glycol, sodium chloride, water for injection, and sodium hydroxide to adjust to a pH of between 6 and 7.
- Preservative: benzalkonium chloride 0.003%
CLINICAL PHARMACOLOGY
Mechanism of Action
Loteprednol etabonate is a corticosteroid. Corticosteroids have been shown to inhibit the inflammatory response to a variety of inciting agents. They inhibit the edema, fibrin deposition, capillary dilation, leukocyte migration, capillary proliferation, fibroblast proliferation, deposition of collagen, and scar formation associated with inflammation. While glucocorticoids are known to bind to and activate the glucocorticoid receptor, the molecular mechanisms involved in glucocorticoid/glucocorticoid receptor-dependent modulation of inflammation are not clearly established. However, corticosteroids are thought to inhibit prostaglandin production through several independent mechanisms.
Pharmacokinetics
The pharmacokinetic exposure to loteprednol etabonate following topical bilateral ocular administration of one drop three times daily of LOTEMAX ® SM for up to two weeks (Day 15) was evaluated in 18 healthy adult subjects. Plasma concentrations of loteprednol etabonate were analyzed using a validated LC/MS/MS method and the lower limit of quantitation for loteprednol etabonate was 0.05 ng/mL. The mean (± SD) C max values for loteprednol etabonate in plasma were 0.13 (± 0.06) ng/mL on Day 1 after a single dose and 0.16 (± 0.06) ng/mL after the last dose on Day 15 of the study. The mean (± SD) AUC t values for loteprednol etabonate in plasma were 0.15 (± 0.15) hr•ng/mL on Day 1 after a single dose and 0.35 (± 0.32) hr•ng/mL after the last dose on Day 15.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies have not been conducted to evaluate the carcinogenic potential of loteprednol etabonate. Loteprednol etabonate was not genotoxic in vitroin the Ames test, the mouse lymphoma tk assay, or in the chromosomal aberration test in human lymphocytes, or in vivoin the mouse micronucleus assay. Treatment of male and female rats with 25 mg/kg/day of loteprednol etabonate (533 times the RHOD based on body surface area, assuming 100% absorption) prior to and during mating caused preimplantation loss and decreased the number of live fetuses/live births. The NOAEL for fertility in rats was 5 mg/kg/day (106 times the RHOD).
CLINICAL STUDIES
In two randomized, multicenter, double-masked, parallel group, vehicle-controlled trials in patients who underwent cataract extraction with intraocular lens implantation, LOTEMAX ® SM administered three times daily to the affected eye beginning the day after cataract surgery was more effective compared to its vehicle in resolving anterior chamber inflammation and pain following surgery. In these studies, LOTEMAX ® SM had statistically significantly higher rates of subjects with complete clearing of anterior chamber cells and of subjects who were pain free at post-operative Day 8 compared to vehicle. Results are shown in the following table.
Outcome | Study 1 | Study 2 | ||||
LOTEMAX ® SM N=171 n (%) | Vehicle N=172 n (%) | Difference (95 CI) % | LOTEMAX ® SM N=200 n (%) | Vehicle N=199 n (%) | Difference (95% CI) % | |
Cells | 49 (29%) | 16 (9%) | 19 (11, 27) | 61 (31%) | 40 (20%) | 10 (2, 19) |
Pain | 125 (73%) | 82 (48%) | 25 (15, 35) | 151 (76%) | 99 (50%) | 26 (17, 35) |
HOW SUPPLIED/STORAGE AND HANDLING
LOTEMAX ® SM (loteprednol etabonate ophthalmic gel) 0.38% is a sterile ophthalmic submicron gel supplied in a white low-density polyethylene plastic bottle with a white controlled drop tip and a pink polypropylene cap in the following size:
- NDC 24208-507-07 5g in a 10 mL bottle
Use only if imprinted neckband is intact.
Storage: Store upright at 15ºC to 25ºC (59ºF to 77ºF). After opening, LOTEMAX ® SM can be used until the expiration date on the bottle.
Mechanism of Action
Loteprednol etabonate is a corticosteroid. Corticosteroids have been shown to inhibit the inflammatory response to a variety of inciting agents. They inhibit the edema, fibrin deposition, capillary dilation, leukocyte migration, capillary proliferation, fibroblast proliferation, deposition of collagen, and scar formation associated with inflammation. While glucocorticoids are known to bind to and activate the glucocorticoid receptor, the molecular mechanisms involved in glucocorticoid/glucocorticoid receptor-dependent modulation of inflammation are not clearly established. However, corticosteroids are thought to inhibit prostaglandin production through several independent mechanisms.