Get your patient on Albuterol Sulfate - Albuterol Sulfate solution (Albuterol Sulfate)
Albuterol Sulfate - Albuterol Sulfate solution prescribing information
INDICATIONS AND USAGE
Albuterol inhalation solution is indicated for the relief of bronchospasm in patients 2 to 12 years of age with asthma (reversible obstructive airway disease).
DOSAGE AND ADMINISTRATION
The usual starting dosage for patients 2 to 12 years of age is 1.25 mg (0.042%) or 0.63 mg (0.021%) of albuterol inhalation solution administered 3 or 4 times daily, as needed, by nebulization. More frequent administration is not recommended.
To administer 1.25 mg or 0.63 mg of albuterol, use the entire contents of one unit-dose vial (3 mL of 0.042% [1.25 mg] or 3 mL of 0.021% [0.63 mg] inhalation solution) by nebulization. Adjust nebulizer flow rate to deliver albuterol inhalation solution over 5 to 15 minutes.
The use of albuterol inhalation solution can be continued as medically indicated to control recurring bouts of bronchospasm. During this time most patients gain optimum benefit from regular use of the inhalation solution.
Patients 6 to 12 years of age with more severe asthma (baseline FEV 1 less than 60% predicted), weight > 40 kg, or patients 11 to 12 years of age may achieve a better initial response with the 1.25 mg dose.
Albuterol inhalation solution has not been studied in the setting of acute attacks of bronchospasm. A 2.5 mg dose of albuterol provided by a higher concentration product (2.5 mg albuterol per 3 mL) may be more appropriate for treating acute exacerbations, particularly in children 6 years old and above.
If a previously effective dosage regimen fails to provide the usual relief, medical advice should be sought immediately, as this is often a sign of seriously worsening asthma which would require reassessment of therapy.
The drug compatibility (physical and chemical), clinical efficacy and safety of albuterol inhalation solution, when mixed with other drugs in a nebulizer have not been established.
The safety and efficacy of albuterol inhalation solution have been established in clinical trials when administered using the Pari LC Plus™ nebulizer and Pari PRONEB™ compressor. The safety and efficacy of albuterol inhalation solution when administered with other nebulizer systems have not been established.
Albuterol inhalation solution should be administered via jet nebulizer connected to an air compressor with adequate air flow, equipped with a mouthpiece or suitable face mask.
CONTRAINDICATIONS
Albuterol inhalation solution is contraindicated in patients with a history of hypersensitivity to any of its components.
ADVERSE REACTIONS
Clinical Trial Experience: Adverse events reported in >1% of patients receiving albuterol sulfate and more frequently than in patients receiving placebo in a four-week double-blind study are listed in the following table.
| 1.25 mg (0.042%) Albuterol Inhalation Solution (n = 115) | 0.63 mg (0.021%) Albuterol Inhalation Solution (n = 117) | Placebo (n = 117) | |
| Asthma Exacerbation | 13 | 11.1 | 8.5 |
| Otitis Media | 4.3 | 0.9 | 0 |
| Allergic Reaction | 0.9 | 3.4 | 1.7 |
| Gastroenteritis | 0.9 | 3.4 | 0.9 |
| Cold Symptoms | 0 | 3.4 | 1.7 |
| Flu Syndrome | 2.6 | 2.6 | 1.7 |
| Lymphadenopathy | 2.6 | 0.9 | 1.7 |
| Skin/Appendage Infection | 1.7 | 0 | 0 |
| Urticaria | 1.7 | 0.9 | 0 |
| Migraine | 0.9 | 1.7 | 0 |
| Chest Pain | 0.9 | 1.7 | 0 |
| Bronchitis | 0.9 | 1.7 | 0.9 |
| Nausea | 1.7 | 0.9 | 0.9 |
There was one case of ST segment depression in the 1.25 mg (0.042%) albuterol inhalation solution treatment group.
No clinically relevant laboratory abnormalities related to albuterol inhalation solution administration were seen in this study.
Postmarketing Experience: Metabolic acidosis has been reported after the use of albuterol inhalation solution. Because this reaction is reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate its frequency or establish a causal relationship to drug exposure.
Drug Interactions
Other short-acting sympathomimetic aerosol bronchodilators or epinephrine should not be used concomitantly with albuterol inhalation solution.
Albuterol inhalation solution should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants or within 2 weeks of discontinuation of such agents, since the action of albuterol on the vascular system may be potentiated.
Beta-receptor blocking agents not only block the pulmonary effect of beta-agonists, such as albuterol inhalation solution, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances (e.g., prophylaxis after myocardial infarction), there may be no acceptable alternatives to the use of beta-adrenergic blocking agents in patients with asthma. In this setting, cardioselective beta-blockers should be considered, although they should be administered with caution.
The ECG changes and/or hypokalemia that may result from the administration of non-potassium sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the dose of the beta-agonist is exceeded. Although the clinical significance of these effects is unknown, caution is advised in the co-administration of beta-agonists with non-potassium sparing diuretics.
Mean decreases of 16% to 22% in serum digoxin levels were demonstrated after single dose intravenous and oral administration of albuterol, respectively, to normal volunteers who had received digoxin for 10 days. The clinical significance of these findings for patients with obstructive airway disease who are receiving albuterol and digoxin on a chronic basis is unclear. Nevertheless, it would be prudent to carefully evaluate the serum digoxin levels in patients who are currently receiving digoxin and albuterol.
DESCRIPTION
Albuterol inhalation solution, USP is a sterile, clear, colorless solution of the sulfate salt of racemic albuterol, albuterol sulfate USP. Albuterol sulfate USP is a relatively selective beta 2 -adrenergic bronchodilator (see CLINICAL PHARMACOLOGY ). The chemical name for albuterol sulfate is α 1 -[( tert -Butylamino)methyl]-4-hydroxy- m -xylene-α,α'-diol sulfate (2:1) (salt), and its established chemical structure is as follows:
The molecular weight of albuterol sulfate USP is 576.7 and the empirical formula is (C 13 H 21 NO 3 ) 2 • H 2 SO 4 . Albuterol sulfate USP is a white crystalline powder, soluble in water and slightly soluble in ethanol. The World Health Organization’s recommended name for albuterol is salbutamol.
Albuterol inhalation solution, USP is supplied in two strengths in unit-dose vials. Each unit-dose vial contains either 0.75 mg of albuterol sulfate USP (equivalent to 0.021% or 0.63 mg of albuterol) or 1.5 mg of albuterol sulfate USP (equivalent to 0.042% or 1.25 mg of albuterol) with sodium chloride and sulfuric acid in a 3 mL isotonic, sterile, aqueous solution. Sodium chloride is added to adjust isotonicity of the solution and sulfuric acid is added to adjust pH of the solution to between 3 and 5 (see HOW SUPPLIED ).
Albuterol inhalation solution, USP does not require dilution prior to administration by nebulization. For albuterol inhalation solution, USP like all other nebulized treatments, the amount delivered to the lungs will depend on patient factors, the jet nebulizer utilized, and compressor performance. Using the Pari LC Plus™ nebulizer (with face mask or mouthpiece) connected to a Pari PRONEB™ compressor, under in vitro conditions, the mean delivered dose from the mouth piece (% nominal dose) was approximately 43% of albuterol (0.042% or 1.25 mg strength) and 39% of albuterol (0.021% or 0.63 mg strength) at a mean flow rate of 3.6 L/min. The mean nebulization time was 15 minutes or less.
Albuterol inhalation solution, USP should be administered from a jet nebulizer at an adequate flow rate, via a mouthpiece or face mask (see DOSAGE AND ADMINISTRATION ).
CLINICAL PHARMACOLOGY
The prime action of beta-adrenergic drugs is to stimulate adenyl cyclase, the enzyme which catalyzes the formation of cyclic-3',-5'-adenosine monophosphate (cyclic AMP) from adenosine triphosphate (ATP). The cyclic AMP thus formed mediates the cellular responses. In vitro studies and in vivo pharmacologic studies have demonstrated that albuterol has a preferential effect on beta 2 -adrenergic receptors compared with isoproterenol. While it is recognized that beta 2 -adrenergic receptors are the predominant receptors in bronchial smooth muscle, recent data indicate that 10% to 50% of the beta-receptors in the human heart may be beta 2 -receptors. The precise function of these receptors, however, is not yet established. Controlled clinical studies and other clinical experience have shown that inhaled albuterol, like other beta-adrenergic agonist drugs, can produce a significant cardiovascular effect in some patients, as measured by pulse rate, blood pressure, symptoms, and/or electrocardiographic changes. Albuterol is longer acting than isoproterenol in most patients by any route of administration because it is not a substrate for the cellular uptake processes for catecholamines nor for catechol- O -methyl transferase.
Pharmacokinetics
Studies in asthmatic patients have shown that less than 20% of a single albuterol dose was absorbed following either intermittent positive-pressure breathing (IPPB) or nebulizer administration; the remaining amount was recovered from the nebulizer and apparatus, and expired air. Most of the absorbed dose was recovered in urine collected during the 24 hours after drug administration. Following oral administration of 4 mg albuterol, the elimination half-life was five to six hours. Following a 3 mg dose of nebulized albuterol in adults, the mean maximum albuterol plasma level at 0.5 hours was 2.1 ng/mL (range, 1.4 to 3.2 ng/mL). The pharmacokinetics of albuterol following administration of 0.63 mg (0.021%) or 1.25 mg (0.042%) albuterol inhalation solution by nebulization have not been determined in children 2 to 12 years old.
Clinical Trials: The safety and efficacy of albuterol inhalation solution was evaluated in a 4-week, multi-center, randomized, double-blind, placebo-controlled, parallel group study in 349 children 6 to 12 years of age with mild-to-moderate asthma (mean baseline FEV 1 60% to 70% of predicted). Approximately half of the patients were also receiving inhaled corticosteroids. Patients were randomized to receive albuterol inhalation solution 0.63 mg (0.021%), albuterol inhalation solution 1.25 mg (0.042%), or placebo three times a day administered via a Pari LC Plus™ nebulizer and a Pari PRONEB™ compressor. Racemic albuterol, delivered by a chlorofluorocarbon (CFC) metered dose inhaler (MDI) or nebulized, was used on an as-needed basis as the rescue medication.
Efficacy, as measured by the mean percent change from baseline in the area under the 6-hour curve for FEV 1 , was demonstrated for both active treatment regimens (n=112 [1.25 mg or 0.042% group] and n=110 [0.63 mg or 0.021% group]) compared with placebo (n=110) on day 1 and day 28. Figures 1 and 2 illustrate the mean percentage change from pre-dose FEV 1 on day 1 and day 28, respectively. The mean baseline FEV 1 for all patients was 1.49 L.
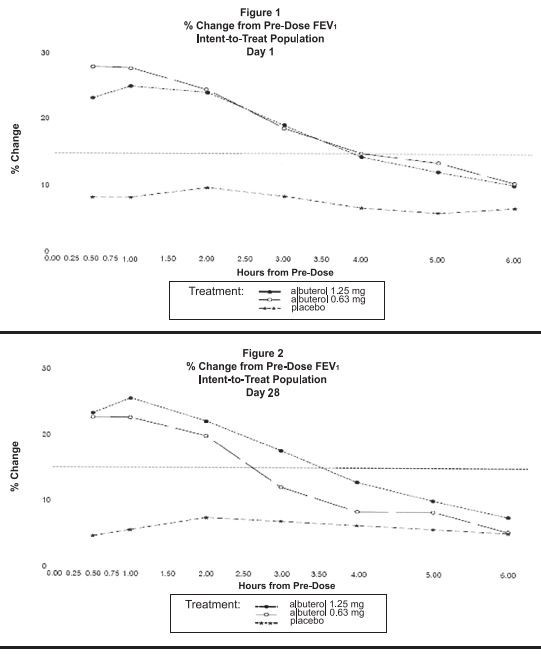
The onset of a 15% increase in FEV 1 over baseline for both doses of albuterol inhalation solution was seen at 30 minutes (the first post-dose assessment). The mean time to peak effect was approximately 30 to 60 minutes for both doses on day 1 and after 4 weeks of treatment. The mean duration of effect, as measured by a >15% increase from baseline in FEV 1 , was approximately 2.5 hours for both doses on day 1 and approximately 2 hours for both doses after 4 weeks of treatment. In some patients, the duration of effect was as long as 6 hours.
HOW SUPPLIED
Albuterol inhalation solution, USP is supplied as a 3 mL, clear, colorless, sterile, preservative-free, aqueous solution in two different strengths, 0.63 mg (0.021%) of albuterol (equivalent to 0.75 mg of albuterol sulfate in 3 mL) and 1.25 mg (0.042%) of albuterol (equivalent to 1.5 mg of albuterol sulfate in 3 mL) in unit-dose low-density polyethylene (LDPE) vials. Each unit-dose LDPE vial is protected in a foil pouch, and each foil pouch contains 1 unit-dose LDPE vial. Each strength of albuterol inhalation solution, USP is available in a shelf carton containing multiple foil pouches.
Albuterol Inhalation Solution, USP 0.021% (0.63 mg / 3 mL) (potency expressed as albuterol equivalent to 0.75 mg albuterol sulfate per 3 mL) in unit-dose vials and is available in the following packaging configurations:
NDC 0487-0301-01 30 foil pouches, each containing 1 vial, total 30 vials per carton
Albuterol Inhalation Solution, USP 0.042% (1.25 mg / 3 mL) (potency expressed as albuterol equivalent to 1.5 mg albuterol sulfate per 3 mL) in unit-dose vials and is available in the following packaging configurations:
NDC 0487-9904-01 30 foil pouches, each containing 1 vial, total 30 vials per carton
Storage and Handling
Store between 20°C to 25°C (68°F to 77°F), excursions permitted to 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature]. Protect from light and excessive heat. Store unit-dose vials in protective foil pouch at all times. Once removed from the foil pouch, use vial within one week. Discard the vial if the solution is not colorless.
Keep out of the reach of children.
Rx Only
Manufactured By: Nephron Pharmaceuticals Corporation West Columbia, SC 29172
INSTRUCTIONS FOR USE
- Remove the vial from the foil pouch.
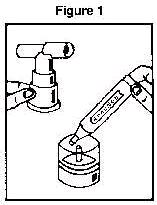
- Twist the cap completely off the vial and squeeze the contents into the nebulizer reservoir (Figure 1).
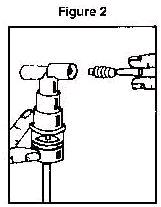
- Connect the nebulizer to the mouthpiece or face mask (Figure 2).
- Connect the nebulizer to the compressor
- Sit in a comfortable, upright position; place the mouthpiece in your mouth (Figure 3) or put on the face mask (Figure 4); and turn on the compressor.
- Breathe as calmly, deeply and evenly as possible through your mouth until no more mist is formed in the nebulizer chamber (about 5 - 15 minutes). At this point, the treatment is finished.
- Clean the nebulizer (see manufacturer's instructions).
Note: Use only as directed by your physician. More frequent administration or higher doses are not recommended.