Get your patient on Amiloride Hydrochloride And Hydrochlorothiazide - Amiloride Hydrochloride And Hydrochlorothiazide tablet (Amiloride Hydrochloride And Hydrochlorothiazide)
Amiloride Hydrochloride And Hydrochlorothiazide - Amiloride Hydrochloride And Hydrochlorothiazide tablet prescribing information
Like other potassium-conserving diuretic combinations, amiloride and hydrochlorothiazide may cause hyperkalemia (serum potassium levels greater than 5.5 mEq per liter). In patients without renal impairment or diabetes mellitus, the risk of hyperkalemia with this combination product is about 1 to 2 percent. This risk is higher in patients with renal impairment or diabetes mellitus (even without recognized diabetic nephropathy). Since hyperkalemia, if uncorrected, is potentially fatal, it is essential to monitor serum potassium levels carefully in any patient receiving amiloride hydrochloride and hydrochlorothiazide, particularly when it is first introduced, at the time of dosage adjustments, and during any illness that could affect renal function.
INDICATIONS AND USAGE
Amiloride hydrochloride and hydrochlorothiazide tablets are indicated in those patients with hypertension or with congestive heart failure who develop hypokalemia when thiazides or other kaliuretic diuretics are used alone, or in whom maintenance of normal serum potassium levels is considered to be clinically important, e.g., digitalized patients, or patients with significant cardiac arrhythmias.
The use of potassium-conserving agents is often unnecessary in patients receiving diuretics for uncomplicated essential hypertension when such patients have a normal diet.
Amiloride hydrochloride and hydrochlorothiazide tablets may be used alone or as an adjunct to other antihypertensive drugs, such as methyldopa or beta blockers. Since amiloride hydrochloride and hydrochlorothiazide enhances the action of these agents, dosage adjustments may be necessary to avoid an excessive fall in blood pressure and other unwanted side effects.
The fixed combination drug is not indicated for the initial therapy of edema or hypertension except in individuals in whom the development of hypokalemia cannot be risked.
DOSAGE AND ADMINISTRATION
Amiloride hydrochloride and hydrochlorothiazide tablets should be administered with food.
The usual starting dosage is 1 tablet a day. The dosage may be increased to 2 tablets a day, if necessary. More than 2 tablets of amiloride hydrochloride and hydrochlorothiazide daily usually are not needed and there is no controlled experience with such doses.
Hydrochlorothiazide can be given at doses of 12.5 to 50 mg per day when used alone. Patients usually do not require doses of hydrochlorothiazide in excess of 50 mg daily when combined with other antihypertensive agents. The daily dose is usually given as a single dose but may be given in divided doses. Once an initial diuresis has been achieved, dosage adjustment may be necessary. Maintenance therapy may be on an intermittent basis.
CONTRAINDICATIONS
Hyperkalemia
Amiloride hydrochloride and hydrochlorothiazide tablets should not be used in the presence of elevated serum potassium levels (greater than 5.5 mEq per liter).
Antikaliuretic Therapy or Potassium Supplementation
Amiloride hydrochloride and hydrochlorothiazide should not be given to patients receiving other potassium-conserving agents, such as spironolactone or triamterene. Potassium supplementation in the form of medication, potassium-containing salt substitutes or a potassium-rich diet should not be used with this product except in severe and/or refractory cases of hypokalemia. Such concomitant therapy can be associated with rapid increases in serum potassium levels. If potassium supplementation is used, careful monitoring of the serum potassium level is necessary.
Impaired Renal Function
Anuria, acute or chronic renal insufficiency, and evidence of diabetic nephropathy are contraindications to the use of amiloride hydrochloride and hydrochlorothiazide. Patients with evidence of renal function impairment (blood urea nitrogen [BUN] levels over 30 mg per 100 mL or serum creatinine levels over 1.5 mg per 100 mL) or diabetes mellitus should not receive the drug without careful, frequent and continuing monitoring of serum electrolytes, creatinine, and BUN levels. Potassium retention associated with the use of an antikaliuretic agent is accentuated in the presence of renal impairment and may result in the rapid development of hyperkalemia.
Hypersensitivity
Amiloride hydrochloride and hydrochlorothiazide tablets is contraindicated in patients who are hypersensitive to this product, or to other sulfonamide-derived drugs.
ADVERSE REACTIONS
Amiloride hydrochloride and hydrochlorothiazide is usually well tolerated and significant clinical adverse effects have been reported infrequently. The risk of hyperkalemia (serum potassium levels greater than 5.5 mEq per liter) with amiloride hydrochloride and hydrochlorothiazide is about 1 to 2 percent in patients without renal impairment or diabetes mellitus (see WARNINGS ). Minor adverse reactions to amiloride hydrochloride have been reported relatively frequently (about 20%) but the relationship of many of the reports to amiloride HCl is uncertain and the overall frequency was similar to hydrochlorothiazide treated groups. Nausea/anorexia, abdominal pain, flatulence, and mild skin rash have been reported and probably are related to amiloride. Other adverse experiences that have been reported with amiloride and hydrochlorothiazide are generally those known to be associated with diuresis, thiazide therapy, or with the underlying disease being treated. Clinical trials have not demonstrated that combining amiloride and hydrochlorothiazide increases the risk of adverse reactions over those seen with the individual components.
The adverse reactions for amiloride and hydrochlorothiazide listed in the following table have been arranged into two groups: (1) incidence greater than one percent; and (2) incidence one percent or less. The incidence for group (1) was determined from clinical studies conducted in the United States (607 patients treated with amiloride and hydrochlorothiazide). The adverse effects listed in group (2) include reports from the same clinical studies and voluntary reports since marketing. The probability of a causal relationship exists between amiloride and hydrochlorothiazide and these adverse reactions, some of which have been reported only rarely.
Incidence > 1% | Incidence ≤ 1% |
Body as a Whole | |
Headache 1 Weakness 1 Fatigue/tiredness | Malaise Chest pain Back pain Syncope |
Cardiovascular | |
Arrhythmia | Tachycardia Digitalis toxicity Orthostatic hypotension Angina pectoris |
Digestive | |
Nausea/anorexia 1 Diarrhea Gastrointestinal pain Abdominal pain | Constipation GI bleeding GI disturbance Appetite changes Abdominal fullness Hiccups Thirst Vomiting Anorexia Flatulence |
Metabolic | |
Elevated serum potassium levels (> 5.5 mEq per liter) 2 | Gout Dehydration Symptomatic hyponatremia 3 |
Musculoskeletal | |
Leg ache | Muscle cramps/spasm Joint pain |
Nervous | |
Dizziness 1 | Paresthesia/numbness Stupor Vertigo |
Psychiatric None | Insomnia Nervousness Depression Sleepiness Mental confusion |
Respiratory | |
Dyspnea | None |
Skin | |
Rash 1 Pruritus | Flushing Diaphoresis Erythema multiforme including Stevens- Johnson syndrome Exfoliative dermatitis including toxic epidermal necrolysis Alopecia |
Special Senses | |
None | Bad taste Visual disturbance Nasal congestion |
Urogenital | |
None | Impotence Nocturia Dysuria Incontinence Renal dysfunction including renal failure Gynecomastia |
1.000000000000000e+00 Reactions occurring in 3% to 8% of patients treated with amiloride hydrochloride and hydrochlorothiazide. (Those reactions occurring in less than 3% of the patients are unmarked.)
2.000000000000000e+00 See WARNINGS
3.000000000000000e+00 See PRECAUTIONS
Other adverse reactions that have been reported with the individual components and within each category are listed in order of decreasing severity:
Amiloride
Body as a Whole: Painful extremities, neck/shoulder ache, fatigability.
Cardiovascular: Palpitation.
Digestive: Activation of probable pre-existing peptic ulcer, abnormal liver function, jaundice, dyspepsia, heartburn.
Hematologic: Aplastic anemia, neutropenia.
Integumentary: Alopecia, itching, dry mouth.
Nervous System/Psychiatric: Encephalopathy, tremors, decreased libido.
Respiratory: Shortness of breath, cough.
Special Senses: Increased intraocular pressure, tinnitus.
Urogenital: Bladder spasms, polyuria, urinary frequency.
Hydrochlorothiazide
Digestive: Pancreatitis, jaundice (intrahepatic cholestatic jaundice), sialadenitis, cramping, gastric irritation.
Hematologic: Aplastic anemia, agranulocytosis, leukopenia, hemolytic anemia, thrombocytopenia.
Hypersensitivity: Anaphylactic reactions, necrotizing angiitis (vasculitis, cutaneous vasculitis), respiratory distress including pneumonitis and pulmonary edema, photosensitivity, fever, urticaria, purpura.
Metabolic: Electrolyte imbalance (see PRECAUTIONS ), hyperglycemia, glycosuria, hyperuricemia.
Nervous System/Psychiatric: Restlessness.
Special Senses : Transient blurred vision, xanthopsia.
Urogenital: Interstitial nephritis (see WARNINGS ).
Postmarketing Experience
Non-melanoma Skin Cancer
Hydrochlorothiazide is associated with an increased risk of non-melanoma skin cancer. In a study conducted in the Sentinel System, increased risk was predominantly for squamous cell carcinoma (SCC) and in white patients taking large cumulative doses. The increased risk for SCC in the overall population was approximately 1 additional case per 16,000 patients per year, and for white patients taking a cumulative dose of ≥ 50,000 mg the risk increase was approximately 1 additional SCC case for every 6,700 patients per year.
To report SUSPECTED ADVERSE REACTIONS, contact Teva at 1-888-838-2872 or FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch.
Drug Interactions
In some patients, the administration of a non-steroidal anti-inflammatory agent can reduce the diuretic, natriuretic, and antihypertensive effects of loop, potassium-sparing and thiazide diuretics. Therefore, when amiloride and hydrochlorothiazide plus non-steroidal anti-inflammatory agents are used concomitantly, the patient should be observed closely to determine if the desired effect of the diuretic is obtained. Since indomethacin and potassium-sparing diuretics, including this product, may each be associated with increased serum potassium levels, the potential effects on potassium kinetics and renal function should be considered when these agents are administered concurrently.
Amiloride HCl
When amiloride HCl is administered concomitantly with an angiotensin-converting enzyme inhibitor, cyclosporine or tacrolimus, the risk of hyperkalemia may be increased. Therefore, if concomitant use of these agents is indicated because of demonstrated hypokalemia, they should be used with caution and with frequent monitoring of serum potassium (see WARNINGS ).
Hydrochlorothiazide
When given concurrently the following drugs may interact with thiazide diuretics.
Alcohol, Barbiturates, or Narcotics
Potentiation of orthostatic hypotension may occur.
Antidiabetic Drugs (Oral Agents and Insulin)
Dosage adjustment of the antidiabetic drug may be required.
Other Antihypertensive Drugs
Additive effect or potentiation.
Cholestyramine and Colestipol Resins
Absorption of hydrochlorothiazide is impaired in the presence of anionic exchange resins. Single doses of cholestyramine and colestipol resins bind the hydrochlorothiazide and reduce its absorption from the gastrointestinal tract by up to 85 and 43 percent, respectively.
Corticosteroids, ACTH
Intensified electrolyte depletion, particularly hypokalemia.
Pressor Amines (e.g., norepinephrine)
Possible decreased response to pressor amines but not sufficient to preclude their use.
Skeletal Muscle Relaxants, Nondepolarizing (e.g., tubocurarine)
Possible increased responsiveness to the muscle relaxant.
Lithium
Generally should not be given with diuretics. Diuretic agents reduce the renal clearance of lithium and add a high risk of lithium toxicity. Refer to the package insert for lithium preparations before use of such preparations with this combination product.
DESCRIPTION
Amiloride hydrochloride and hydrochlorothiazide tablets, USP combine the potassium-conserving action of amiloride hydrochloride with the natriuretic action of hydrochlorothiazide.
Amiloride HCl, USP is designated chemically as N -amidino-3,5,-diamino-6-chloropyrazine-carboxamide monohydrochloride dihydrate and its structural formula is:
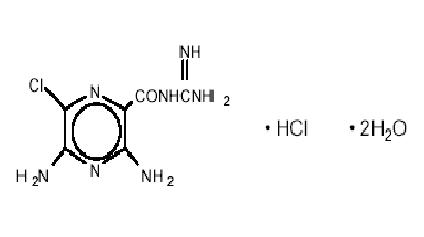
C 6 H 8 CIN 7 O•HCl•2H 2 O M.W. 302.12
Hydrochlorothiazide, USP is designated chemically as 6-chloro-3,4-dihydro-2 H -1, 2, 4-benzo-thiadiazine-7-sulfonamide 1, 1-dioxide. Its structural formula is:
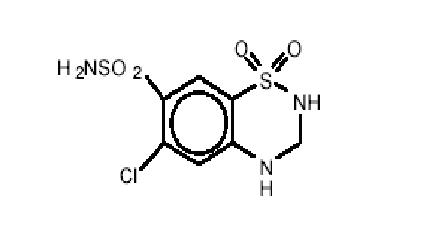
C 7 H 8 CIN 3 O 4 S 2 M.W. 297.74
It is a white, or practically white, crystalline powder which is slightly soluble in water, but freely soluble in sodium hydroxide solution.
Each tablet, for oral administration, contains 5 mg of amiloride hydrochloride, USP (calculated on the anhydrous basis) and 50 mg of hydrochlorothiazide, USP.
Inactive Ingredients: Croscarmellose sodium, D&C yellow no. 10 (aluminum lake), lactose monohydrate, magnesium oxide, magnesium stearate, microcrystalline cellulose.
HOW SUPPLIED
Amiloride hydrochloride and hydrochlorothiazide tablets, USP are available as:
5 mg/50 mg: | Light yellow, round, scored, biconvex tablet. Debossed with 555 over 483 on the scored side and stylized barr on the other side. Each tablet contains 5 mg of anhydrous amiloride HCl, USP and 50 mg of hydrochlorothiazide, USP. |
100 Tablets NDC 0555-0483-02 1000 Tablets NDC 0555-0483-05 |
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
Store at 20º to 25ºC (68º to 77ºF) [See USP Controlled Room Temperature].
Keep this and all medications out of the reach of children.
Manufactured In Canada By:
Teva Canada Limited
Toronto, Canada M1B 2K9
Manufactured For:
Teva Pharmaceuticals
Parsippany, NJ 07054
Rev. D 12/2022