Get your patient on Aminocaproic Acid - Aminocaproic Acid tablet (Aminocaproic Acid)
Aminocaproic Acid - Aminocaproic Acid tablet prescribing information
INDICATIONS AND USAGE
Aminocaproic acid is useful in enhancing hemostasis when fibrinolysis contributes to bleeding. In life- threatening situations, transfusion of appropriate blood products and other emergency measures may be required.
Fibrinolytic bleeding may frequently be associated with surgical complications following heart surgery (with or without cardiac bypass procedures) and portacaval shunt; hematological disorders such as amegakaryocytic thrombocytopenia (accompanying aplastic anemia); acute and life-threatening abruptio placentae; hepatic cirrhosis; and neoplastic disease such as carcinoma of the prostate, lung, stomach, and cervix.
Urinary fibrinolysis, usualIy a normal physiological phenomenon, may contribute to excessive urinary tract fibrinolytic bleeding associated with surgical hematuria (following prostatectomy and nephrectomy) or nonsurgical hematuria (accompanying polycystic or neoplastic diseases of the genitourinary system). (See WARNINGS . )
DOSAGE AND ADMINISTRATION
An identical dosage regimen may be followed by administering aminocaproic acid tablets as follows:
For the treatment of acute bleeding syndromes due to elevated fibrinolytic activity, it is suggested that 5 Aminocaproic acid 1000 mg Tablets or 10 Aminocaproic acid 500 mg Tablets (5 g) be administered during the first hour of treatment, followed by a continuing rate of 1 Aminocaproic acid 1000 mg Tablet or 2 Aminocaproic acid 500 mg Tablets (1 g) per hour. This method of treatment would ordinarily be continued for about 8 hours or until the bleeding situation has been controlled.
CONTRAINDICATIONS
Aminocaproic acid should not be used when there is evidence of an active intravascular clotting process.
When there is uncertainty as to whether the cause of bleeding is primary fibrinolysis or disseminated intravascular coagulation (DIC), this distinction must be made before administering aminocaproic acid.
The following tests can be applied to differentiate the two conditions:
- Platelet count is usually decreased in DIC but normal in primary fibrinolysis.
- Protamine paracoagulation test is positive in DIC; a precipitate forms when protamine sulfate is dropped into citrated plasma. The test is negative in the presence of primary fibrinolysis.
- The euglobulin clot lysis test is abnormal in primary fibrinolysis but normal in DIC.
Aminocaproic acid must not be used in the presence of DIC without concomitant heparin.
ADVERSE REACTIONS
Aminocaproic acid is generally well tolerated. The following adverse experiences have been reported:
General: Edema, headache, malaise.
Hypersensitivity Reactions: Allergic and anaphylactoid reactions, anaphylaxis.
Cardiovascular: Bradycardia, hypotension, peripheral ischemia, thrombosis.
Gastrointestinal: Abdominal pain, diarrhea, nausea, vomiting.
Hematologic: Agranulocytosis, coagulation disorder, leukopenia, thrombocytopenia.
Musculoskeletal: CPK increased, muscle weakness, myalgia, myopathy (see WARNINGS ), myositis, rhabdomyolysis.
Neurologic: Confusion, convulsions, delirium, dizziness, hallucinations, intracranial hypertension, stroke, syncope.
Respiratory: Dyspnea, nasal congestion, pulmonary embolism.
Skin: Pruritis, rash.
Special Senses: Tinnitus, vision decreased, watery eyes.
Urogenital: BUN increased, renal failure. There have been some reports of dry ejaculation during the period of aminocaproic acid treatment. These have been reported to date only in hemophilia patients who received the drug after undergoing dental surgical procedures. However, this symptom resolved in all patients within 24 to 48 hours of completion of therapy.
To report SUSPECTED ADVERSE REACTIONS, contact PuraCap Laboratories, LLC DBA Blu Pharmaceuticals at 1-888-374-2791 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DESCRIPTION
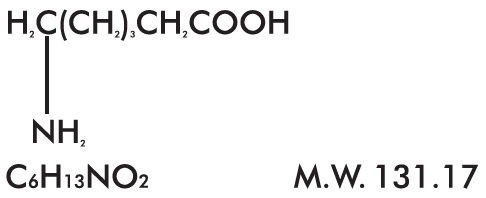
Aminocaproic acid, USP is 6-aminohexanoic acid, which acts as an inhibitor of fibrinolysis. Its chemical structure is:
Aminocaproic acid, USP is soluble in water, acid, and alkaline solutions; it is sparingly soluble in methanol and practically insoluble in chloroform.
Each Aminocaproic Acid Tablet, for oral administration contains 500 mg or 1000 mg of aminocaproic acid and the following inactive ingredients: crospovidone, magnesium stearate, povidone and stearic acid.
CLINICAL PHARMACOLOGY
The fibrinolysis-inhibitory effects of aminocaproic acid appear to be exerted principally via inhibition of plasminogen activators and to a lesser degree through antiplasmin activity.
In adults, oral absorption appears to be a zero-order process with an absorption rate of 5.2 g/hr. The mean lag time in absorption is 10 minutes. After a single oral dose of 5 g, absorption was complete (F=1). Mean ± SD peak plasma concentrations (164 ± 28 mcg/mL) were reached within 1.2 ± 0.45 hours.
After oral administration, the apparent volume of distribution was estimated to be 23.1 ± 6.6 L (mean± SD). Correspondingly, the volume of distribution after intravenous administration has been reported to be 30.0 ± 8.2 L. After prolonged administration, aminocaproic acid has been found to distribute throughout extravascular and intravascular compartments of the body, penetrating human red blood cells as well as other tissue cells.
Renal excretion is the primary route of elimination. Sixty-five percent of the dose is recovered in the urine as unchanged drug and 11% of the dose appears as the metabolite adipic acid. Renal clearance (116 mL/min) approximates endogenous creatinine clearance. The total body clearance is 169 mL/min. The terminal elimination half-life for aminocaproic acid is approximately 2 hours.
HOW SUPPLIED
Aminocaproic acid Tablets USP, 500 mg
Each white, round, standard concave tablet debossed with "LP 231" on one side and scored on other side, contains 500 mg of aminocaproic acid.
Bottle of 30 – NDC 24658-798-30
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]; Dispense in Tight Containers.
Aminocaproic acid Tablets USP, 1000 mg
Each white, caplet shaped tablet debossed with "LP 232" on one side and scored on other side, contains 1000 mg of aminocaproic acid.
Bottle of 30 – NDC 24658-799-30
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]; Dispense in Tight Containers.