Get your patient on Aviane - Levonorgestrel And Ethinyl Estradiol (Levonorgestrel And Ethinyl Estradiol)
Aviane - Levonorgestrel And Ethinyl Estradiol prescribing information
WARNING: CIGARETTE SMOKING AND SERIOUS CARDIOVASCULAR EVENTS Cigarette smoking increases the risk of serious cardiovascular events from combined oral-contraceptives (COC) use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked. For this reason, COCs, including Aviane (levonorgestrel and ethinyl estradiol tablets), are contraindicated in women who are over 35 years of age and smoke.
INDICATIONS AND USAGE
Aviane (levonorgestrel and ethinyl estradiol tablets) is indicated for use by females of reproductive potential to prevent pregnancy.
Limitations of use: The efficacy of Aviane (levonorgestrel and ethinyl estradiol tablets) in women with a body mass index (BMI) of > 35 kg/m 2 has not been adequately evaluated.
In a clinical trial with Aviane (levonorgestrel and ethinyl estradiol tablets), 1,477 subjects had 7,720 cycles of use and a total of 5 pregnancies were reported. This represents an overall pregnancy rate of 0.84 per 100 woman-years. This rate includes patients who did not take the drug correctly. One or more pills were missed during 1,479 (18.8%) of the 7,870 cycles; thus all tablets were taken during 6,391 (81.2%) of the 7,870 cycles. Of the total 7,870 cycles, a total of 150 cycles were excluded from the calculation of the Pearl index due to the use of backup contraception and/or missing 3 or more consecutive pills.
The mean BMI of the study population was 24 kg/m 2 . Females with a BMI greater than 30 kg/m 2 accounted for 12.1% (n=179) of the study population. Females with a BMI over 35 kg/m 2 accounted for 4.3% (n=63) of the study population.
DOSAGE AND ADMINISTRATION
To achieve maximum contraceptive effectiveness, Aviane (levonorgestrel and ethinyl estradiol tablets) must be taken exactly as directed and at intervals not exceeding 24 hours. The dosage of Aviane-28 is one orange tablet daily for 21 consecutive days, followed by one light-green inert tablet daily for 7 consecutive days, according to the prescribed schedule. It is recommended that Aviane-28 tablets be taken at the same time each day.
The dispenser should be kept in the wallet supplied to avoid possible fading of the pills. If the pills fade, patients should continue to take them as directed.
During the first cycle of use
The possibility of ovulation and conception prior to initiation of medication should be considered. The patient should be instructed to begin taking Aviane on either the first Sunday after the onset of menstruation (Sunday Start) or on Day 1 of menstruation (Day 1 Start).
Sunday start:
The patient is instructed to begin taking Aviane-28 on the first Sunday after the onset of menstruation. If menstruation begins on a Sunday, the first tablet (orange) is taken that day. One orange tablet should be taken daily for 21 consecutive days, followed by one light-green inert tablet daily for 7 consecutive days. Withdrawal bleeding should usually occur within 3 days following discontinuation of orange tablets and may not have finished before the next pack is started. During the first cycle, contraceptive reliance should not be placed on Aviane-28 until an orange tablet has been taken daily for 7 consecutive days, and a nonhormonal back-up method of birth control should be used during those 7 days.
Day 1 start:
During the first cycle of medication, the patient is instructed to begin taking Aviane-28 during the first 24 hours of her period (day one of her menstrual cycle). One orange tablet should be taken daily for 21 consecutive days, followed by one light-green inert tablet daily for 7 consecutive days. Withdrawal bleeding should usually occur within 3 days following discontinuation of orange tablets and may not have finished before the next pack is started. If medication is begun on day one of the menstrual cycle, no back-up contraception is necessary. If Aviane-28 tablets are started later than day one of the first menstrual cycle or postpartum, contraceptive reliance should not be placed on Aviane-28 tablets until after the first 7 consecutive days of administration, and a nonhormonal back-up method of birth control should be used during those 7 days.
After the first cycle of use
The patient begins her next and all subsequent courses of tablets on the day after taking her last light-green tablet. She should follow the same dosing schedule: 21 days on orange tablets followed by 7 days on light-green tablets. If in any cycle the patient starts tablets later than the proper day, she should protect herself against pregnancy by using a nonhormonal back-up method of birth control until she has taken an orange tablet daily for 7 consecutive days.
Switching from another hormonal method of contraception
When the patient is switching from a 21-day regimen of tablets, she should wait 7 days after her last tablet before she starts Aviane. She will probably experience withdrawal bleeding during that week. She should be sure that no more than 7 days pass after her previous 21-day regimen. When the patient is switching from a 28-day regimen of tablets, she should start her first pack of Aviane on the day after her last tablet. She should not wait any days between packs. The patient may switch any day from a progestin-only pill and should begin Aviane the next day. If switching from an implant or injection, the patient should start Aviane on the day of implant removal or, if using an injection, the day the next injection would be due. In switching from a progestin-only pill, injection, implant, or intrauterine system (IUS), the patient should be advised to use additional nonhormonal contraception (such as condoms) until active tablets have been taken for 7 consecutive days of the first pack.
If spotting or breakthrough bleeding occurs
If spotting or breakthrough bleeding occur, the patient is instructed to continue on the same regimen. This type of bleeding is usually transient and without significance; however, if the bleeding is persistent or prolonged, the patient is advised to consult her physician.
Risk of pregnancy if tablets are missed
While there is little likelihood of ovulation occurring if only one or two orange tablets are missed, the possibility of ovulation increases with each successive day that scheduled orange tablets are missed. Although the occurrence of pregnancy is unlikely if Aviane is taken according to directions, if withdrawal bleeding does not occur, the possibility of pregnancy must be considered. If the patient has not adhered to the prescribed schedule (missed one or more tablets or started taking them on a day later than she should have), the probability of pregnancy should be considered at the time of the first missed period and appropriate diagnostic measures taken. If the patient has adhered to the prescribed regimen and misses two consecutive periods, pregnancy should be ruled out.
The risk of pregnancy increases with each active (orange) tablet missed. For additional patient instructions regarding missed tablets, see the WHAT TO DO IF YOU MISS PILLS section in the DETAILED PATIENT LABELING below.
Use after pregnancy, abortion or miscarriage
Aviane may be initiated no earlier than day 28 postpartum in the nonlactating mother or after a second trimester abortion due to the increased risk for thromboembolism (see C ONTRAINDICATIONS , WARNINGS , and PRECAUTIONS concerning thromboembolic disease). The patient should be advised to use additional nonhormonal contraception (such as condoms) until active tablets have been taken for 7 consecutive days.
Aviane may be initiated immediately after a first trimester abortion or miscarriage. Instruct the patient to use additional nonhormonal contraception (such as condoms) until active tablets have been taken for 7 consecutive days, unless starting Aviane on the day of surgical abortion.
CONTRAINDICATIONS
Combination oral contraceptives should not be used in women with any of the following conditions:
- Thrombophlebitis or thromboembolic disorders
- A history of deep-vein thrombophlebitis or thromboembolic disorders
- Cerebrovascular or coronary artery disease (current or past history)
- Valvular heart disease with thrombogenic complications
- Thrombogenic rhythm disorders
- Hereditary or acquired thrombophilias
- Prolonged immobilization (especially with major surgery)
- Diabetes with vascular involvement
- Headaches with focal neurological symptoms or migraine with aura
- Women with migraine who are 35 years or older
- Uncontrolled hypertension
- Known or suspected carcinoma of the breast or personal history of breast cancer
- Known or suspected estrogen- or progesterone sensitive malignancy
- Undiagnosed abnormal vaginal bleeding
- Cholestatic jaundice of pregnancy or jaundice with prior pill use
- Hepatic adenomas or carcinomas, or active liver disease
Women who are receiving Hepatitis C drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to the potential for alanine aminotransferase (ALT) elevations (see WARNINGS, Risk of Liver Enzyme Elevations with Concomitant Hepatitis C Treatment ) .
ADVERSE REACTIONS
An increased risk of the following serious adverse reactions (see WARNINGS section for additional information) has been associated with the use of oral contraceptives:
Thromboembolic and thrombotic disorders and other vascular problems (including thrombophlebitis and venous thrombosis with or without pulmonary embolism, mesenteric thrombosis, arterial thromboembolism, myocardial infarction, cerebral hemorrhage, cerebral thrombosis), carcinoma of the reproductive organs and breasts, hepatic neoplasia (including hepatic adenomas or benign liver tumors), ocular lesions (including retinal vascular thrombosis), gallbladder disease, carbohydrate and lipid effects, elevated blood pressure, and headache including migraine.
Five studies that compared breast cancer risk between ever-users (current or past use) of COCs and never-users of COCs reported no association between ever use of COCs and breast cancer risk, with effect estimates ranging from 0.90 - 1.12 (Figure 2).
Three studies compared breast cancer risk between current or recent COC users (<6 months since last use) and never users of COCs (Figure 2). One of these studies reported no association between breast cancer risk and COC use. The other two studies found an increased relative risk of 1.19 - 1.33 with current or recent use. Both of these studies found an increased risk of breast cancer with current use of longer duration, with relative risks ranging from 1.03 with less than one year of COC use to approximately 1.4 with more than 8-10 years of COC use.
FIGURE 2: Relevant Studies of Risk of Breast Cancer with Combined Oral Contraceptives
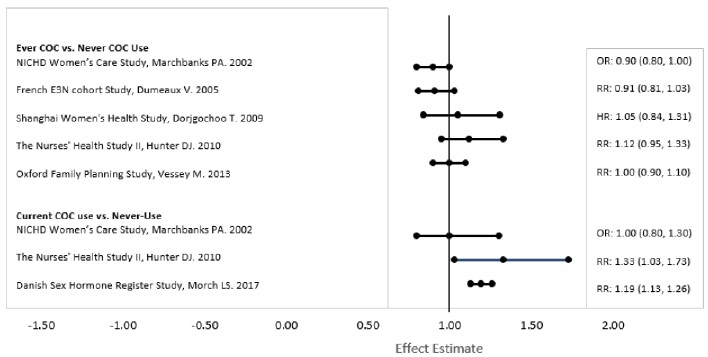
RR = relative risk; OR = odds ratio; HR = hazard ratio. “ever COC” are females with current or past COC use; “never COC use” are females that never used COCs.
The following adverse reactions associated with the use of oral CHCs were identified in clinical studies or postmarketing reports. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Common adverse reactions associated with oral CHCs are headache, abdominal pain, nausea, metrorrhagia, vaginal moniliasis and pain, acne, and vaginitis.
Additional adverse reactions that have been reported include the following:
Eye disorder: intolerance to contact lenses, steepening of corneal curvature
Gastrointestinal disorders: Abdominal bloating, vomiting
General disorders and administration site conditions: Edema, fluid retention
Hepatobiliary disorders: Cholestatic jaundice
Psychiatric disorders: Change in libido, mood changes
Reproductive system and breast disorders: Amenorrhea, breast tenderness, breast pain, breast enlargement, increased cervical mucous, change in menstrual flow, unscheduled bleeding
Skin and subcutaneous tissue disorders: Acne, melasma
Vascular disorders: Budd-Chiari syndrome, aggravation of varicose veins
To report SUSPECTED ADVERSE EVENTS, contact Teva at 1-888-838-2872 or FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch for voluntary reporting of adverse reactions.
DESCRIPTION
21 orange active tablets each containing 0.10 mg of levonorgestrel, USP (-)-13-Ethyl-17-hydroxy-18,19-dinor-17α-pregn-4-en-20-yn-3-one, a totally synthetic progestogen, and 0.02 mg of ethinyl estradiol, USP, (19-Nor-17α-pregna-1,3,5(10)-trien-20-yne-3,17-diol). The inactive ingredients present are: FD&C yellow no. 6 aluminum lake, hypromellose, lactose monohydrate, magnesium stearate, microcrystalline cellulose, polyethylene glycol, pregelatinized corn starch, sodium starch glycolate and titanium dioxide.
7 light-green, inert tablets each containing: D&C yellow no. 10 aluminum lake, FD&C blue no. 1 aluminum lake, FD&C yellow no. 6 aluminum lake, lactose monohydrate, magnesium stearate, microcrystalline cellulose and pregelatinized corn starch.
Levonorgestrel, USP
C 21 H 28 O 2 M.W. 312.45
Ethinyl Estradiol, USP
C 20 H 24 O 2 M.W. 296.40
CLINICAL PHARMACOLOGY
Mode of Action
Combination oral contraceptives prevent pregnancy primarily by suppressing ovulation.
Pharmacokinetics
Absorption
No specific investigation of the absolute bioavailability of Aviane in humans has been conducted. However, literature indicates that levonorgestrel is rapidly and completely absorbed after oral administration (bioavailability about 100%) and is not subject to first-pass metabolism. Ethinyl estradiol is rapidly and almost completely absorbed from the gastrointestinal tract but, due to first-pass metabolism in gut mucosa and liver, the bioavailability of ethinyl estradiol is between 38% and 48%.
After a single dose of Aviane to 22 women under fasting conditions, maximum serum concentrations of levonorgestrel are 2.8 ± 0.9 ng/mL (mean ± SD) at 1.6 ± 0.9 hours. At steady state, attained from day 19 onwards, maximum levonorgestrel concentrations of 6.0 ± 2.7 ng/mL are reached at 1.5 ± 0.5 hours after the daily dose. The minimum serum levels of levonorgestrel at steady state are 1.9 ± 1.0 ng/mL. Observed levonorgestrel concentrations increased from day 1 (single dose) to days 6 and 21 (multiple doses) by 34% and 96%, respectively (Figure 1). Unbound levonorgestrel concentrations increased from day 1 to days 6 and 21 by 25% and 83%, respectively. The kinetics of total levonorgestrel are non-linear due to an increase in binding of levonorgestrel to sex hormone binding globulin (SHBG), which is attributed to increased SHBG levels that are induced by the daily administration of ethinyl estradiol.
Following a single dose, maximum serum concentrations of ethinyl estradiol of 62 ± 21 pg/mL are reached at 1.5 ± 0.5 hours. At steady state, attained from at least day 6 onwards, maximum concentrations of ethinyl estradiol were 77 ± 30 pg/mL and were reached at 1.3 ± 0.7 hours after the daily dose. The minimum serum levels of ethinyl estradiol at steady state are 10.5 ± 5.1 pg/mL. Ethinyl estradiol concentrations did not increase from days 1 to 6, but did increase by 19% from days 1 to 21 (Figure 1).
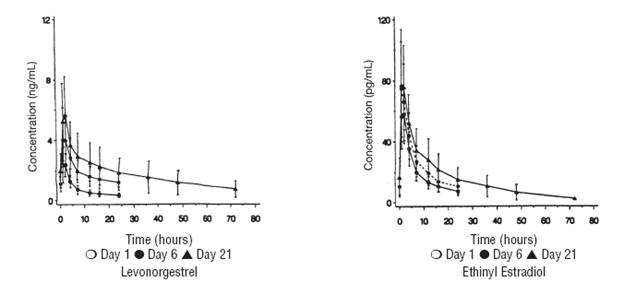
FIGURE 1: Mean (SE) levonorgestrel and ethinyl estradiol serum concentrations in 22 subjects receiving 100 mcg levonorgestrel and 20 mcg ethinyl estradiol
TABLE 1 provides a summary of levonorgestrel and ethinyl estradiol pharmacokinetic parameters.
Levonorgestrel | ||||||
C max | T max | AUC | CL/F | Vλz/F | SHBG | |
Day | ng/mL | h | ng•h/mL | mL/h/kg | L/kg | nmol/L |
1 | 2.75 (0.88) | 1.6 (0.9) | 35.2 (12.8) | 53.7 (20.8) | 2.66 (1.09) | 57 (18) |
6 | 4.52 (1.79) | 1.5 (0.7) | 46.0 (18.8) | 40.8 (14.5) | 2.05 (0.86) | 81 (25) |
21 | 6.00 (2.65) | 1.5 (0.5) | 68.3 (32.5) | 28.4 (10.3) | 1.43 (0.62) | 93 (40) |
Unbound Levonorgestrel | ||||||
pg/mL | h | pg•h/mL | L/h/kg | L/kg | fu% | |
1 | 51.2 (12.9) | 1.6 (0.9) | 654 (201) | 2.79 (0.97) | 135.9 (41.8) | 1.92 (0.30) |
6 | 77.9 (22.0) | 1.5 (0.7) | 794 (240) | 2.24 (0.59) | 112.4 (40.5) | 1.80 (0.24) |
21 | 103.6 (36.9) | 1.5 (0.5) | 1177 (452) | 1.57 (0.49) | 78.6 (29.7) | 1.78 (0.19) |
Ethinyl Estradiol | ||||||
pg/mL | h | pg•h/mL | mL/h/kg | L/kg | ||
1 | 62.0 (20.5) | 1.5 (0.5) | 653 (227) | 567 (204) | 14.3 (3.7) | |
6 | 76.7 (29.9) | 1.3 (0.7) | 604 (231) | 610 (196) | 15.5 (4.0) | |
21 | 82.3 (33.2) | 1.4 (0.6) | 776 (308) | 486 (179) | 12.4 (4.1) | |
Distribution
Levonorgestrel in serum is primarily bound to SHBG. Ethinyl estradiol is about 97% bound to plasma albumin. Ethinyl estradiol does not bind to SHBG, but induces SHBG synthesis.
Metabolism
Levonorgestrel:
The most important metabolic pathway occurs in the reduction of the Δ4-3-oxo group and hydroxylation at positions 2α, 1β, and 16β, followed by conjugation. Most of the metabolites that circulate in the blood are sulfates of 3α,5β-tetrahydro-levonorgestrel, while excretion occurs predominantly in the form of glucuronides. Some of the parent levonorgestrel also circulates as 17β-sulfate. Metabolic clearance rates may differ among individuals by several-fold, and this may account in part for the wide variation observed in levonorgestrel concentrations among users.
Ethinyl estradiol:
Cytochrome P450 enzymes (CYP3A4) in the liver are responsible for the 2-hydroxylation that is the major oxidative reaction. The 2-hydroxy metabolite is further transformed by methylation and glucuronidation prior to urinary and fecal excretion. Levels of Cytochrome P450 (CYP3A) vary widely among individuals and can explain the variation in rates of ethinyl estradiol 2-hydroxylation. Ethinyl estradiol is excreted in the urine and feces as glucuronide and sulfate conjugates, and undergoes enterohepatic circulation.
Excretion
The elimination half-life for levonorgestrel is approximately 36 ± 13 hours at steady state. Levonorgestrel and its metabolites are primarily excreted in the urine (40% to 68%) and about 16% to 48% are excreted in feces. The elimination half-life of ethinyl estradiol is 18 ± 4.7 hours at steady state.
Special Populations
Race
Based on the pharmacokinetic study with Aviane, there are no apparent differences in pharmacokinetic parameters among women of different races.
Hepatic Insufficiency
No formal studies have evaluated the effect of hepatic disease on the disposition of Aviane. However, steroid hormones may be poorly metabolized in patients with impaired liver function.
Renal Insufficiency
No formal studies have evaluated the effect of renal disease on the disposition of Aviane.
Drug-Drug Interactions
See PRECAUTIONS - Drug Interactions
HOW SUPPLIED
Aviane ® (levonorgestrel and ethinyl estradiol tablets USP), 0.10 mg/0.02 mg is available as 28 tablets packaged in cartons (NDC: 0555-9045-58) of six blister card dispensers. Each blister card dispenser contains 21 orange active tablets and 7 light-green inert tablets. Each orange tablet is round, film coated and debossed with dp on one side and 016 on the other side. Each light-green tablet is round and debossed with dp on one side and 519 on the other side.
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
Keep this and all medications out of the reach of children.
Brands listed are the registered trademarks of their respective owners.
Teva Pharmaceuticals USA, Inc.
North Wales, PA 19454
Rev. F 7/2024