Get your patient on Clobetasol Propionate - Clobetasol Propionate spray (Clobetasol Propionate)
Clobetasol Propionate - Clobetasol Propionate spray prescribing information
INDICATIONS AND USAGE
Clobetasol propionate spray, 0.05% is a corticosteroid indicated for the topical treatment of moderate to severe plaque psoriasis affecting up to 20% body surface area (BSA) in patients 18 years of age or older. (1.1 )
Limitations of Use:
Indication
Clobetasol propionate spray, 0.05% is a super-high potent topical corticosteroid formulation indicated for the treatment of moderate to severe plaque psoriasis affecting up to 20% body surface area (BSA) in patients 18 years of age or older.
Patients should be instructed to use clobetasol propionate spray, 0.05% for the minimum amount of time necessary to achieve the desired results [ see Dosage and Administration (2 ) ].
Use in patients under 18 years of age is not recommended because safety has not been established and because numerically high rates of HPA axis suppression were seen with other clobetasol propionate topical formulations. [see Use in Specific Populations (8.4 )]
Limitations of Use
Clobetasol propionate spray, 0.05% should not be used on the face, axillae, or groin. Clobetasol propionate spray, 0.05% should not be used if there is atrophy at the treatment site. Clobetasol propionate spray, 0.05% should not be used in the treatment of rosacea or perioral dermatitis.
DOSAGE AND ADMINISTRATION
- Not for oral, ophthalmic, or intravaginal use. (1.2 )
- Spray directly onto the affected skin areas twice daily and rub in gently. (2 )
- The total dosage should not exceed 50 g (59 mL or 2 fluid ounces) per week. Do not use more than 26 sprays per application or 52 sprays per day. (2 )
- Treatment beyond 2 weeks should be limited to localized lesions of moderate to severe plaque psoriasis that have not sufficiently improved after the initial 2 weeks of treatment with clobetasol propionate spray, 0.05%. (2 )
- Do not use for more than 4 weeks (2 )
Clobetasol propionate spray, 0.05% is for topical use only, and not for ophthalmic, oral or intravaginal use.
Clobetasol propionate spray, 0.05% should be sprayed directly onto the affected skin areas twice daily and rubbed in gently and completely.
The total dosage should not exceed 50 g (59 mL or 2 fluid ounces) per week because of the potential for the drug to suppress the hypothalamic-pituitary-adrenal (HPA) axis. Do not use more than 26 sprays per application or 52 sprays per day.
Clobetasol propionate spray, 0.05% contains a topical corticosteroid; therefore treatment should be limited to 4 weeks. Therapy should be discontinued when control has been achieved. Treatment beyond 2 weeks should be limited to localized lesions of moderate to severe plaque psoriasis that have not sufficiently improved after the initial 2 weeks of treatment with clobetasol propionate spray, 0.05%. If no improvement is seen within 2 weeks, reassessment of diagnosis may be necessary. Before prescribing for more than 2 weeks, any additional benefits of extending treatment to 4 weeks should be weighed against the risk of HPA axis suppression.
Unless directed by physician, clobetasol propionate spray, 0.05% should not be used with occlusive dressings.
DOSAGE FORMS AND STRENGTHS
Spray, 0.05% w/w (3 )
Spray, 0.05% w/w. Each gram of clobetasol propionate spray, 0.05% contains 0.5 mg of clobetasol propionate in a clear, colorless liquid.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no available data on clobetasol propionate spray, 0.05% use in pregnant women to identify a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes.
Observational studies suggest an increased risk of low birthweight in infants with the maternal use of potent or very potent topical corticosteroids (see Data). Advise pregnant women that clobetasol propionate spray, 0.05% may increase the risk of having a low birth weight infant and to use clobetasol propionate spray, 0.05% on the smallest area of skin and for the shortest duration possible.
Animal reproduction studies have not been conducted with clobetasol propionate spray, 0.05%. In an animal reproduction study, subcutaneous administration of clobetasol propionate to pregnant rats at doses greater than 12.5 μg/kg/day during the period of organogenesis caused an increase in malformations (increased incidence of umbilical hernia) (see Data). The available data do not allow calculation of relevant comparisons between the systemic exposure of clobetasol propionate in animal studies to the systemic
exposure that would be expected in humans after topical use of clobetasol propionate spray, 0.05%.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Data
Human Data
Available observational studies in pregnant women did not identify a drug-associated risk of major birth defects, preterm delivery, or fetal mortality with the use of topical corticosteroids of any potency. However, when the dispensed amount of potent or very potent topical corticosteroids exceeded 300 g during the entire pregnancy, maternal use was associated with an increased risk of low birth weight in infants.
Animal Data
Clobetasol propionate is absorbed percutaneously, and when administered subcutaneously it caused malformations in both the rabbit and the mouse.
Clobetasol propionate has greater potential for adverse developmental effects than steroids that are less potent.
The effect of clobetasol propionate on pregnancy outcome and development of offspring was studied in the rat. Clobetasol propionate was administered subcutaneously to female rats twice daily (0, 12.5, 25, and 50 μg/kg/day) from day 7 of presumed gestation through day 25 of lactation or day 24 presumed gestation for those rats that did not deliver a litter. The maternal noobserved- adverse-effect-level (NOAEL) for clobetasol propionate was less than 12.5 μg/kg/day due to reduced body weight gain and feed consumption during the gestation period. The reproductive NOAEL in the dams was 25 μg/kg/day based on prolonged delivery at 50 μg/kg/day. The NOAEL for viability and growth in the offspring was 12.5 μg/kg/day based on incidence of stillbirths, reductions in pup body weights on days 1 and 7 of lactation, increased pup mortality, increases in the incidence of umbilical hernia, and increases in the incidence of pups with cysts on the kidney at higher dose levels during the preweaning period. The weights of the epididymides and testes were significantly reduced at higher dosages. Despite these changes, there were no effects on the mating and fertility of the offspring.
Lactation
Risk Summary
There is no information regarding the presence of clobetasol propionate in human milk or its effects on the breastfed infant or on milk production. It is not known whether topical administration of clobetasol propionate could result in sufficient systemic absorption to produce detectable quantities in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for clobetasol propionate spray, 0.05% and any potential adverse effects on the breastfed infant from clobetasol propionate spray, 0.05% or from the underlying maternal condition.
Clinical Considerations
To minimize potential exposure to the breastfed infant via breast milk, use clobetasol propionate spray, 0.05% on the smallest area of skin and for the shortest duration possible while breastfeeding. Advise breastfeeding women not to apply clobetasol propionate spray, 0.05% directly to the nipple and areola to avoid direct infant exposure [see Use in Specific Populations (8.4 )] .
Pediatric Use
Use in patients under 18 years of age is not recommended, because safety has not been established and because numerically high rates of HPA axis suppression were seen with other clobetasol propionate topical formulations. Safety and effectiveness in pediatric patients treated with clobetasol propionate spray, 0.05% have not been established [ see Warnings and Precautions (5.1 ) ].
Because of higher ratio of skin surface area to body mass, pediatric patients are at a greater risk than adults of HPA axis suppression and Cushing's syndrome when they are treated with topical corticosteroids. They are therefore also at greater risk of glucocorticosteroid insufficiency during and/or after withdrawal of treatment. Adverse effects including striae have been reported with inappropriate use of topical corticosteroids in infants and children.
HPA axis suppression, Cushing's syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include low plasma cortisol levels and absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
Geriatric Use
Clinical studies of clobetasol propionate spray, 0.05% did not include sufficient numbers of patients aged 65 and over to adequately determine whether they respond differently than younger patients. In two randomized, vehicle controlled clinical trials, 21 of the 240 patients (9%) were over the age of 65. In general, dose selection for an elderly patient should be made with caution, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal or cardiac function, and of concomitant disease or other drug therapy.
CONTRAINDICATIONS
None.
None.
WARNINGS AND PRECAUTIONS
- Clobetasol propionate is a highly potent topical corticosteroid that has been shown to suppress the HPA axis at the lowest doses tested. (5.1 )
- Cushing's syndrome, hyperglycemia, and unmasking of latent diabetes mellitus can also result from systemic absorption of topical corticosteroids. (5.1 )
- Systemic absorption may require periodic evaluation for HPA axis suppression. Modify use if HPA axis suppression develops. (5.1 )
- Children may be more susceptible to systemic toxicity from use of topical corticosteroids. (5.1 , 8.4 )
- Clobetasol propionate spray, 0.05% may increase the risk of cataract and glaucoma. If visual symptoms occur, consider referral to an ophthalmologist. (5.2 )
- Local adverse reactions with topical corticosteroids may occur more frequently with the use of occlusive dressings and higher potency corticosteroids, including clobetasol propionate. (5.3 )
- Clobetasol propionate spray, 0.05% is flammable, keep away from heat or flame. (5.5 )
Effects on the Endocrine System
Clobetasol propionate is a highly potent topical corticosteroid that has been shown to suppress the HPA axis at the lowest doses tested.
Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for clinical glucocorticosteroid insufficiency. This may occur during treatment or upon withdrawal of the topical corticosteroid.
In studies evaluating the potential for hypothalamic-pituitary-adrenal (HPA) axis suppression, using the Cosyntropin Stimulation Test, clobetasol propionate spray, 0.05% demonstrated rates of suppression that were comparable after 2 and 4 weeks of twice-daily use (19% and 15 to 20%, respectively), in adult patients with moderate to severe plaque psoriasis (≥ 20% BSA). In these studies, HPA axis suppression was defined as serum cortisol level ≤ 18 mcg/dL 30 min post cosyntropin stimulation [ see Clinical Pharmacology (12 ) ].
Because of the potential for systemic absorption, use of topical corticosteroids may require that patients be periodically evaluated for HPA axis suppression. Factors that predispose a patient using a topical corticosteroid to HPA axis suppression include the use of more potent steroids, use over large surface areas, use over prolonged periods, use under occlusion, use on an altered skin barrier, and use in patients with liver failure.
An ACTH stimulation test may be helpful in evaluating patients for HPA axis suppression. If HPA axis suppression is documented, an attempt should be made to gradually withdraw the drug, to reduce the frequency of application, or to substitute a less potent steroid. Manifestations of adrenal insufficiency may require supplemental systemic corticosteroids. Recovery of HPA axis function is generally prompt and complete upon discontinuation of topical corticosteroids.
Cushing's syndrome, hyperglycemia, and unmasking of latent diabetes mellitus can also result from systemic absorption of topical corticosteroids.
Use of more than one corticosteroid-containing product at the same time may increase the total systemic corticosteroid exposure.
Pediatric patients may be more susceptible to systemic toxicity from use of topical corticosteroids. [ see Use in Specific Populations (8.4 ) ]
Ophthalmic Adverse Reactions
Use of topical corticosteroids, including clobetasol propionate spray, 0.05%, may increase the risks of glaucoma and posterior subcapsular cataract. Glaucoma and cataracts have been reported in postmarketing experience with the use of topical corticosteroid products, including topical clobetasol products [see Adverse Reactions (6.2 )] .
Avoid contact of clobetasol propionate spray, 0.05% with eyes. Advise patients to report any visual symptoms and consider referral to an ophthalmologist for evaluation.
Local Adverse Reactions with Topical Corticosteroids
The following additional local adverse reactions have been reported with topical corticosteroids. They may occur more frequently with the use of occlusive dressings and higher potency corticosteroids, including clobetasol propionate. These reactions are listed in an approximate decreasing order of occurrence: folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, striae and miliaria.
Allergic Contact Dermatitis
Allergic contact dermatitis to any component of topical corticosteroids is usually diagnosed by a failure to heal rather than a clinical exacerbation. Clinical diagnosis of allergic contact dermatitis can be confirmed by patch testing.
Concomitant Skin Infections
In the presence of dermatological infections, the use of an appropriate antifungal or antibacterial agent should be instituted. If a favorable response does not occur promptly, use of clobetasol propionate spray, 0.05% should be discontinued until the infection has been adequately controlled.
Flammable Contents
Clobetasol propionate spray, 0.05% is flammable; keep away from heat or flame.
ADVERSE REACTIONS
In controlled, clinical trials with clobetasol propionate spray, 0.05%, the most common adverse reactions (incidence > 2%) were burning, pruritus, nasopharyngitis, upper respiratory tract infection. (6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Zydus Pharmaceuticals USA Inc. at 1-877-993-8779 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In controlled, clinical trials with clobetasol propionate spray, 0.05%, the most common adverse reaction was burning at the site of application [40% of subjects treated with clobetasol propionate spray, 0.05% and 47% of subjects treated with Spray Vehicle]. Other commonly reported adverse reactions for clobetasol propionate spray, 0.05% and Spray Vehicle, respectively, are noted in Table 1.
| Adverse Reaction | Clobetasol Propionate 0.05% Spray (N=120) | Vehicle Spray (N=120) |
| System Organ Class | ||
| General disorders and administration site conditions | 50 (42%) | 56 (47%) |
| Application site burning | 48 (40%) | 56 (47%) |
| Application site dryness | 2 (2%) | 0 (0%) |
| Application site irritation | 1 (1%) | 0 (0%) |
| Application site pain | 1 (1%) | 2 (2%) |
| Application site pigmentation changes | 1 (1%) | 0 (0%) |
| Application site pruritus | 4 (3%) | 3 (3%) |
| Infections and infestations | 17 (14%) | 12 (10%) |
| Nasopharyngitis | 6 (5%) | 3 (3%) |
| Pharyngitis streptococcal | 1 (1%) | 0 (0%) |
| Upper respiratory tract infection | 10 (8%) | 2 (2%) |
| Skin and subcutaneous tissue disorders | 4 (3%) | 2 (2%) |
| Eczema asteatotic | 2 (2%) | 0 (0%) |
Most local adverse reactions were rated as mild to moderate and they are not affected by age, race or gender.
Systemic absorption of topical corticosteroids has produced hypothalamic-pituitary-adrenal (HPA) axis suppression, manifestations of Cushing's syndrome, hyperglycemia, and glycosuria in some patients.
Postmarketing Experience
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The following adverse reactions have been identified during post-approval use of clobetasol propionate spray, 0.05%.
Skin: Burning, pruritus, erythema, pain, irritation, rash, peeling, urticaria, and contact dermatitis.
Ophthalmic adverse reactions of blurred vision, cataracts, glaucoma, increased intraocular pressure, and central serous chorioretinopathy have been reported with the use of topical corticosteroids.
DESCRIPTION
Clobetasol propionate spray, 0.05% contains clobetasol propionate, a synthetic fluorinated corticosteroid, for topical use. The corticosteroids constitute a class of primarily synthetic steroids used topically as anti-inflammatory and antipruritic agents. Clobetasol propionate is 21-chloro-9-fluoro-11β, 17 dihydroxy-16β -methylpregna-1,4-diene-3,20-dione 17-propionate, with the molecular formula C 25 H 32 CIFO 5 , and a molecular weight of 466.97 (CAS Registry Number 25122-41-2).
The following is the chemical structure:
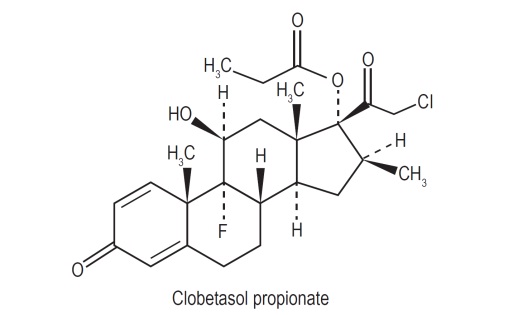
Clobetasol propionate, USP is a white to cream crystalline powder that is soluble in acetone, in dimethyl sulfoxide, in chloroform, in methanol, and in dioxane; sparingly soluble in ethanol; slightly soluble in benzene and in diethyl ether; and practically insoluble in water. Each gram of clobetasol propionate spray, 0.05% contains 0.5 mg of clobetasol propionate, in a clear, colorless liquid composed of alcohol, isopropyl myristate, sodium lauryl sulfate, and undecylenic acid.
CLINICAL PHARMACOLOGY
Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action in corticosteroid responsive dermatoses is unknown.
Pharmacodynamics
Vasoconstrictor Assay
Clobetasol propionate spray, 0.05% is in the super-high range of potency as demonstrated in a vasoconstrictor study in healthy subjects when compared with other topical corticosteroids. However, similar blanching scores do not necessarily imply therapeutic equivalence.
Hypothalamic-Pituitary-Adrenal (HPA) Axis Suppression
The effect of clobetasol propionate spray, 0.05% on hypothalamic-pituitary-adrenal (HPA) axis function was investigated in adults in two studies. In the first study, patients with plaque psoriasis covering at least 20% of their body applied clobetasol propionate spray, 0.05% twice daily for up to 4 weeks. 15% (2 out of 13) of patients displayed adrenal suppression after 4 weeks of use based on the Cosyntropin Stimulation Test. The laboratory suppression was transient; all subjects returned to normal after cessation of drug use. In the second study, patients with plaque psoriasis covering at least 20% of their body applied clobetasol propionate spray, 0.05% twice daily for either 2 or 4 weeks. 19% (4 out of 21) of patients treated for 2 weeks and 20% (3 out of 15) of patients treated for 4 weeks displayed adrenal suppression at the end of treatment based on the Cosyntropin Stimulation Test. The laboratory suppression was transient; all subjects returned to normal after cessation of drug use. In these studies, HPA axis suppression was defined as serum cortisol level ≤ 18 mcg/dL 30 min post cosyntropin (ACTH 1 to 24) stimulation [see Warnings and Precautions (5 ) ] .
Pharmacokinetics
The extent of percutaneous absorption of topical corticosteroids is determined by many factors, including the vehicle, the integrity of the epidermal barrier and occlusion.
Topical corticosteroids can be absorbed from normal intact skin. Inflammation and other disease processes in the skin may increase percutaneous absorption.
There are no human data regarding the distribution of corticosteroids to body organs following topical application. Nevertheless, once absorbed through the skin, topical corticosteroids are handled through metabolic pathways similar to systemically administered corticosteroids. They are metabolized, primarily in the liver, and are then excreted by the kidneys. In addition, some corticosteroids and their metabolites are also excreted in the bile.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Clobetasol propionate was not carcinogenic to rats when topically applied for 2 years at concentrations up to 0.005% which corresponded to doses up to 11 μg/kg/day.
Clobetasol propionate was negative in the in vitro mammalian chromosomal aberration test and in the in vivo mammalian erythrocyte micronucleus test.
The effect of subcutaneously administered clobetasol propionate on fertility and general reproductive toxicity was studied in rats at doses of 0, 12.5, 25, and 50 μg/kg/day. Males were treated beginning 70 days before mating and females beginning 15 days before mating through day 7 of gestation. A dosage level of less than 12.5 μg/kg/day clobetasol propionate was considered to be the NOAEL for paternal and maternal general toxicity based on decreased weight gain and for male reproductive toxicity based on increased weights of fluid-filled seminal vesicles. The female reproductive NOAEL was 12.5 μg/kg/day based on reduction in the numbers of estrous cycles during the pre-cohabitation period and an increase in the number of nonviable embryos at higher doses.
CLINICAL STUDIES
The efficacy of clobetasol propionate spray, 0.05% in psoriasis has been demonstrated in two randomized, vehicle controlled clinical trials, which were identical in design. The studies were conducted in patients aged 18 years and older with moderate to severe plaque psoriasis. Patients were treated twice daily for up to 4 weeks with either clobetasol propionate spray, 0.05% or vehicle spray.
Patients were evaluated on their Overall Disease Severity, a 5-point scale based on scaling, erythema, and plaque elevation that classified subjects as clear, almost clear, mild, moderate, or severe/very severe. Only patients classified as moderate or severe/very severe at baseline were enrolled in the studies. The median percent body surface area (BSA) at baseline was 6% for the two studies. The numbers of patients scored as clear or almost clear at Weeks 2 and 4 are presented in Table 2.
| Study 1 | Study 2 | ||||
| Clobetasol Propionate N = 60 | Vehicle N = 60 | Clobetasol Propionate N = 60 | Vehicle N = 60 | ||
| Week 2 | Clear Almost Clear | 1 (2%) 32 (53%) | 0 (0%) 1 (2%) | 0 (0%) 28 (47%) | 0 (0%) 0 (0%) |
| Week 4 | Clear Almost Clear | 15 (25%) 32 (53%) | 0 (0%) 2 (3%) | 18 (30%) 31 (52%) | 0 (0%) 1 (2%) |
HOW SUPPLIED/STORAGE AND HANDLING
Clobetasol propionate spray, 0.05% is a clear, colorless liquid, filled in white HDPE bottle fitted with white polypropylene cap and are supplied as follows:
2 fl oz/59 mL NDC 68382-998-01
4.25 fl oz/125 mL NDC 68382-998-02
Storage
Keep tightly closed. Store under controlled room temperature conditions 20°C to 25°C (68°F to 77°F) with excursions permitted between 15°C and 30°C (59°F and 86°F). Do not refrigerate or store above 86°F (30°C). Spray is flammable; avoid heat, flame or smoking when using this product.
Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action in corticosteroid responsive dermatoses is unknown.