Get your patient on Desonide - Desonide gel (Desonide)
Desonide - Desonide gel prescribing information
1 INDICATIONS AND USAGE
Desonide Gel, 0.05% is indicated for the treatment of mild to moderate atopic dermatitis in patients 3 months of age and older.
Patients should be instructed to use Desonide Gel, 0.05% for the minimum amount of time as necessary to achieve the desired results because of the potential for Desonide Gel, 0.05% to suppress the hypothalamicpituitary-adrenal (HPA) axis [see Warnings and Precautions (5.1 )]. Treatment should not exceed 4 consecutive weeks [see Dosage and Administration (2 )].
2 DOSAGE AND ADMINISTRATION
Apply a thin layer to the affected areas two times daily and rub in gently. Discontinue use when control is achieved. If no improvement is seen within 4 weeks, reassessment of diagnosis may be necessary. Treatment beyond 4 consecutive weeks is not recommended. Do not use with occlusive dressings. Avoid contact with eyes or other mucous membranes.
For topical use only. Not for oral, ophthalmic, or intravaginal use.
3 DOSAGE FORMS AND STRENGTHS
Gel, 0.05%; (0.5mg/g) desonide in a translucent to opaque gel
8 USE IN SPECIFIC POPULATIONS
Safety and effectiveness of Desonide Gel, 0.05% in pediatric patients less than 3 months of age have not been evaluated, and therefore its use in this age group is not recommended. (8.4 )
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 05/2016
8.1 Pregnancy
Teratogenic effects: Pregnancy Category C:
There are no adequate and well-controlled studies in pregnant women. Therefore, Desonide Gel, 0.05%
should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal
application in laboratory animals.
No reproductive studies in animals have been performed with Desonide Gel, 0.05%. Dermal embryofetal
development studies were conducted in rats and rabbits with a desonide cream, 0.05% formulation. Topical doses of 0.2, 0.6, and 2.0 g cream/kg/day of a desonide cream, 0.05% formulation or 2.0 g/kg of the cream base were administered topically to pregnant rats (gestational days 6-15) and pregnant rabbits (gestational days 6-18). Maternal body weight loss was noted at all dose levels of the desonide cream, 0.05% formulation in rats and rabbits. Teratogenic effects characteristic of corticosteroids were noted in both species. The desonide cream, 0.05% formulation was teratogenic in rats at topical doses of 0.6 and 2.0 g cream/kg/day and in rabbits at a topical dose of 2.0 g cream/kg/day. No teratogenic effects were noted for the desonide cream, 0.05% formulation at a topical dose of 0.2 g cream/kg/day in rats and 0.6 g cream/kg/day in rabbits. These doses (0.2 g cream/kg/day and 0.6 g cream/kg/day) are similar to the
maximum recommended human dose based on body surface area comparisons.
Teratogenic effects: Pregnancy Category C:
There are no adequate and well-controlled studies in pregnant women. Therefore, Desonide Gel, 0.05% should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Some corticosteroids have been shown to be teratogenic after dermal application in laboratory animals.
No reproductive studies in animals have been performed with Desonide Gel, 0.05%. Dermal embryofetal development studies were conducted in rats and rabbits with a desonide cream, 0.05% formulation. Topical doses of 0.2, 0.6, and 2.0 g cream/kg/day of a desonide cream, 0.05% formulation or 2.0 g/kg of the cream base were administered topically to pregnant rats (gestational days 6-15) and pregnant rabbits (gestational days 6-18). Maternal body weight loss was noted at all dose levels of the desonide cream, 0.05% formulation in rats and rabbits. Teratogenic effects characteristic of corticosteroids were noted in both species. The desonide cream, 0.05% formulation was teratogenic in rats at topical doses of 0.6 and 2.0 g cream/kg/day and in rabbits at a topical dose of 2.0 g cream/kg/day. No teratogenic effects were noted for the desonide cream, 0.05% formulation at a topical dose of 0.2 g cream/kg/day in rats and 0.6 g cream/kg/day in rabbits. These doses (0.2 g cream/kg/day and 0.6 g cream/kg/day) are similar to the maximum recommended human dose based on body surface area comparisons.
8.3 Nursing Mothers
Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk. Because many drugs are excreted in human milk, caution should be exercised when Desonide Gel, 0.05% is administered to a nursing woman.
8.4 Pediatric Use
Safety and effectiveness of Desonide Gel, 0.05% in pediatric patients less than 3 months of age have not been evaluated, and therefore its use in this age group is not recommended.
The effect of Desonide Gel, 0.05% on HPA axis function was investigated in pediatric subjects, with atopic dermatitis covering at least 35% of their body, who were treated with Desonide Gel, 0.05% twice daily for 4 weeks. One of 37 subjects (3%) displayed adrenal suppression after 4 weeks of use, based on the cosyntropin stimulation test [see Warnings and Precautions (5.1 )] .
In controlled clinical studies in subjects 3 months to 18 years of age, 425 subjects were treated with Desonide Gel, 0.05% and 157 subjects were treated with vehicle [see Adverse Reactions (6 ) and Clinical Studies (14 )] .
Because of a higher ratio of skin surface area to body mass, pediatric patients are at a greater risk than adults of HPA axis suppression when they are treated with topical corticosteroids. They are therefore also at greater risk of glucocorticosteroid insufficiency after withdrawal of treatment and of Cushing’s syndrome while on treatment.
Adverse effects, including striae, have been reported with inappropriate use of topical corticosteroids in infants and children. HPA axis suppression, Cushing’s syndrome, linear growth retardation, delayed weight gain and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include low plasma cortisol levels and absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
8.5 Geriatric Use
Clinical studies of Desonide Gel, 0.05% did not include patients aged 65 and older to determine if they respond differently than younger patients. Treatment of this patient population should reflect the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
4 CONTRAINDICATIONS
Desonide Gel, 0.05% is contraindicated in those patients with a history of hypersensitivity to any of the components of the preparation.
5 WARNINGS AND PRECAUTIONS
• Topical corticosteroids can produce reversible hypothalamic pituitary adrenal (HPA) axis suppression, Cushing’s syndrome and unmask latent diabetes. (5.1 )
• Systemic absorption may require evaluation for HPA axis suppression. (5.1 )
• Modify use should HPA axis suppression develop (5.1 )
• Potent corticosteroids, use on large areas, prolonged use or occlusive use may increase systemic absorption (5.1 )
• Local adverse reactions may include atrophy, striae, irritation, acneiform eruptions, hypopigmentation, and allergic contact dermatitis and may be more likely with occlusive use or more potent corticosteroids. (5.2 , 5.4 , 6 )
• Children may be more susceptible to systemic toxicity when treated with topical corticosteroids. (5.1 , 8.4 )
5.1 Effects on Endocrine System
Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for clinical glucocorticosteroid insufficiency. This may occur during treatment or upon withdrawal of the topical corticosteroid.
The effect of Desonide Gel, 0.05% on HPA axis function was investigated in pediatric subjects, 6 months to 6 years old, with atopic dermatitis covering at least 35% of their body, who were treated with Desonide Gel, 0.05% twice daily for 4 weeks. One of 37 subjects (3%) displayed adrenal suppression after 4 weeks of use, based on the cosyntropin stimulation test. As follow-up evaluation of the subject’s adrenal axis was not performed, it is unknown whether the suppression was reversible [see Use In Specific Populations (8.4 ) and Clinical Pharmacology (12.2 )].
Pediatric patients may be more susceptible than adults to systemic toxicity from equivalent doses of Desonide Gel, 0.05% due to their larger skin surface-to-body mass ratios [see Use In Specific Populations (8.4 )].
Because of the potential for systemic absorption, use of topical corticosteroids may require that patients be periodically evaluated for HPA axis suppression. Factors that predispose a patient using a topical corticosteroid to HPA axis suppression include the use of more potent steroids, use over large surface areas, use over prolonged periods, use under occlusion, use on an altered skin barrier, and use in patients with liver failure.
An ACTH stimulation test may be helpful in evaluating patients for HPA axis suppression. If HPA axis suppression is documented, an attempt should be made to gradually withdraw the drug, to reduce the frequency of application, or to substitute a less potent steroid. Manifestations of adrenal insufficiency may require supplemental systemic corticosteroids. Recovery of HPA axis function is generally prompt and complete upon discontinuation of topical corticosteroids.
Cushing’s syndrome, hyperglycemia, and unmasking of latent diabetes mellitus can also result from systemic absorption of topical corticosteroids.
Use of more than one corticosteroid-containing product at the same time may increase the total systemic corticosteroid exposure.
5.2 Local Adverse Reactions with Topical Corticosteroids
Local adverse reactions may be more likely to occur with occlusive use, prolonged use or use of higher potency corticosteroids. Reactions may include skin atrophy, striae, telangiectasias, burning, itching, irritation, dryness, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, and miliaria. Some local adverse reactions may be irreversible.
5.3 Concomitant Skin Infections
If concomitant skin infections are present or develop during treatment, an appropriate antifungal or antibacterial agent should be used. If a favorable response does not occur promptly, use of Desonide Gel, 0.05% should be discontinued until the infection is adequately controlled.
5.4 Skin Irritation
If irritation develops, Desonide Gel, 0.05% should be discontinued and appropriate therapy instituted. Allergic contact dermatitis with corticosteroids is usually diagnosed by observing failure to heal rather than noting a clinical exacerbation as with most topical products not containing corticosteroids. Such an observation should be corroborated with appropriate diagnostic patch testing.
6 ADVERSE REACTIONS
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In controlled clinical studies of 425 Desonide Gel, 0.05%-treated subjects and 157 Vehicle-treated subjects, adverse events occurred at the application site in 3% of subjects treated with Desonide Gel, 0.05% and the incidence rate was not higher compared with vehicle-treated subjects. The most common local adverse events in Desonide Gel, 0.05% treated subjects were application site burning in 1% (4/425) and rash in 1% (3/425) followed by application site pruritus in <1% (2/425).
Adverse events that resulted in premature discontinuation of study drug in Desonide Gel, 0.05% treated subjects were telangiectasia and worsening of atopic dermatitis in one subject each. Additional adverse events observed during clinical trials for patients treated with Desonide Gel, 0.05% included headache in 2% (8/425) compared with 1% (2/157) in those treated with vehicle.
The following additional local adverse reactions have been reported infrequently with topical corticosteroids. They may occur more frequently with the use of occlusive dressings, especially with higher potency corticosteroids. These reactions are listed in an approximate decreasing order of occurrence: folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, secondary infection, skin atrophy, striae, and miliaria.
11 DESCRIPTION
Desonide Gel, 0.05% contains desonide [(pregna-1, 4-diene-3, 20-dione,11, 21-dihydroxy-16,17-[(1-methylethylidene) bis(oxy)]-,(11β,16α)]- a synthetic nonfluorinated corticosteroid for topical dermatologic use. Chemically, desonide is C 24 H 32 O 6 . It has the following structural formula:
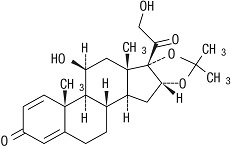
Desonide has the molecular weight of 416.52. It is a white to off-white odorless powder which is soluble in methanol and practically insoluble in water. Each gram of Desonide Gel, 0.05% contains 0.5 mg of desonide in an aqueous gel base of purified water, glycerin, propylene glycol, edetate disodium, methylparaben, propylparaben, sodium hydroxide, and Carbopol ® 974 P.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The mechanism of action of desonide is unknown.
12.2 Pharmacodynamics
In an HPA axis suppression study, one of 37 (3%) pediatric subjects, 6 months to 6 years old, with moderate to severe atopic dermatitis covering at least 35% body surface area who applied Desonide Gel, 0.05% experienced suppression of the adrenal glands following 4 weeks of therapy [see Warnings And Precautions (5.1 ) and Use In Specific Populations (8.4 )] . A follow-up evaluation of the subject’s adrenal axis was not performed; it is unknown whether the suppression was reversible.
Pharmacokinetics
The extent of percutaneous absorption of topical corticosteroids is determined by many factors, including product formulation and the integrity of the epidermal barrier. Occlusion, inflammation and/or other disease processes in the skin may also increase percutaneous absorption. Once absorbed through the skin, topical corticosteroids are handled through pharmacokinetic pathways similar to systemically administered corticosteroids. They are metabolized primarily in the liver and then are excreted by the kidneys. Some corticosteroids and their metabolites are also excreted in the bile.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Systemic long-term animal studies have not been performed to evaluate the carcinogenic potential of desonide or its effect on fertility. In a 26-week dermal carcinogenicity study conducted in transgenic (Tg.AC) mice, once daily application of 0.005% to 0.05% Desonide Gel 0.05 % significantly increased the incidence of papillomas at the treatment site in males and females compared to their respective control animals. The clinical relevance of these findings in animals to humans is not clear.
Desonide revealed no evidence of mutagenic potential based on the results of an in vitro genotoxicity test (Ames assay) and an in vivo genotoxicity test (mouse micronucleus assay). Desonide was positive without S9 activation and was equivocal with S9 activation in an in vitro mammalian cell mutagenesis assay (L5178YITK+ mouse lymphoma assay). A dose response trend was not noted in this assay.
14 CLINICAL STUDIES
In two randomized vehicle-controlled clinical studies, subjects 3 months to 18 years of age with mild to moderate atopic dermatitis were treated twice daily for 4 weeks with either Desonide Gel, 0.05% or vehicle. Treatment success was defined as achieving clear or almost clear on the Investigator’s Global Severity Score (IGSS) with at least a 2-point change (decrease) from the subject’s baseline IGSS when compared to the Week 4 IGSS.
The results of the 2 clinical trials are summarized in Table 1:
| Clinical Trial 1 | |
Desonide Gel, 0.05% N = 289 | Vehicle N = 92 |
| 128 (44%) | 13 (14%) |
| Clinical Trial 2 | |
Desonide Gel, 0.05% N = 136 | Vehicle N = 65 |
| 38 (28%) | 4 (6%) |
16 HOW SUPPLIED/STORAGE AND HANDLING
Desonide Gel, 0.05% is a translucent to opaque gel supplied in 60g tubes in cartons containing 1x 60g tube (NDC 24470-920-60).
Storage:
Store at controlled room temperature: 25°C (77°F); excursions permitted between 15°C and 30°C (59°F and 86°F).
Keep out of reach of children.
12.1 Mechanism of Action
The mechanism of action of desonide is unknown.