Get your patient on Dextroamphetamine Sulfate - Dextroamphetamine Sulfate tablet (Dextroamphetamine Sulfate)
Dextroamphetamine Sulfate - Dextroamphetamine Sulfate tablet prescribing information
WARNING ABUSE, MISUSE, AND ADDICTION
Dextroamphetamine sulfate has a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including dextroamphetamine sulfate, can result in overdose and death (see OVERDOSAGE), and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection. Before prescribing dextroamphetamine sulfate, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout dextroamphetamine sulfate treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction (see WARNINGS and DRUG ABUSE and DEPENDENCE)
DOSAGE AND ADMINISTRATION
Amphetamines should be administered at the lowest effective dosage and dosage should be individually adjusted. Late evening doses should be avoided because of the resulting insomnia.
Narcolepsy
Usual dose is 5 to 60 mg per day in divided doses, depending on the individual patient response.
Narcolepsy seldom occurs in children under 12 years of age; however, when it does, dextroamphetamine sulfate may be used. The suggested initial dose for patients aged 6 to 12 is 5 mg daily; daily dose may be raised in increments of 5 mg at weekly intervals until an optimal response is obtained. In patients 12 years of age and older, start with 10 mg daily; daily dosage may be raised in increments of 10 mg at weekly intervals until optimal response is obtained. If bothersome adverse reactions appear (e.g., insomnia or anorexia), dosage should be reduced. Give first dose on awakening; additional doses (1 or 2) at intervals of 4 to 6 hours.
Attention Deficit Disorder with Hyperactivity
Not recommended for pediatric patients under 3 years of age.
In pediatric patients from 3 to 5 years of age , start with 2.5 mg daily; daily dosage may be raised in increments of 2.5 mg at weekly intervals until optimal response is obtained.
In pediatric patients 6 years of age and older , start with 5 mg once or twice daily; daily dosage may be raised in increments of 5 mg at weekly intervals until optimal response is obtained. Only in rare cases will it be necessary to exceed a total of 40 mg per day.
Give first dose on awakening; additional doses (1 or 2) at intervals of 4 to 6 hours.
Where possible, drug administration should be interrupted occasionally to determine if there is a recurrence of behavioral symptoms sufficient to require continued therapy.
Prior to treating patients with dextroamphetamine sulfate tablets assess:
• for the presence of cardiac disease (i.e., perform a careful history, family history of sudden death or ventricular arrhythmia, and physical exam) (see WARNINGS ).
• the family history and clinically evaluate patients for motor or verbal tics or Tourette’s syndrome (see WARNINGS ).
CONTRAINDICATIONS
Known hypersensitivity to amphetamine products.
During or within 14 days following the administration of monoamine oxidase inhibitors (hypertensive crises may result).
ADVERSE REACTIONS
Cardiovascular
Palpitations, tachycardia, elevation of blood pressure. There have been isolated reports of cardiomyopathy associated with chronic amphetamine use.
Central Nervous System
Psychotic episodes at recommended doses (rare), overstimulation, restlessness, dizziness, insomnia, euphoria, dyskinesia, dysphoria, tremor, headache, exacerbation of motor and verbal tics and Tourette's syndrome.
Gastrointestinal
Dryness of the mouth, unpleasant taste, diarrhea, constipation, intestinal ischemia and other gastrointestinal disturbances. Anorexia and weight loss may occur as undesirable effects.
Allergic
Urticaria.
Endocrine
Impotence, changes in libido, frequent or prolonged erections.
Musculoskeletal
Rhabdomyolysis.
Increased intraocular pressure and glaucoma.
To report SUSPECTED ADVERSE REACTIONS, contact Aurobindo Pharma USA, Inc. at 1-866-850-2876
or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
MAO Inhibitors
MAOI antidepressants, as well as a metabolite of furazolidone, slow amphetamine metabolism. This slowing potentiates amphetamines, increasing their effect on the release of norepinephrine and other monoamines from adrenergic nerve endings; this can cause headaches and other signs of hypertensive crisis. A variety of neurological toxic effects and malignant hyperpyrexia can occur, sometimes with fatal results.
Serotonergic Drugs
The concomitant use of dextroamphetamine sulfate tablets and serotonergic drugs increases the risk of serotonin syndrome. Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome, particularly during dextroamphetamine sulfate tablets initiation or dosage increase. If serotonin syndrome occurs, discontinue dextroamphetamine sulfate tablets and the concomitant serotonergic drug(s) (see WARNINGS and PRECAUTIONS ). Examples of serotonergic drugs include selective serotonin reuptake inhibitors (SSRI), serotonin norepinephrine reuptake inhibitors (SNRI), triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, St. John’s Wort.
CYP2D6 Inhibitors
The concomitant use of dextroamphetamine sulfate tablets and CYP2D6 inhibitors may increase the exposure of dextroamphetamine sulfate tablets compared to the use of the drug alone and increase the risk of serotonin syndrome. Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome particularly during dextroamphetamine sulfate tablets initiation and after a dosage increase. If serotonin syndrome occurs, discontinue dextroamphetamine sulfate tablets and the CYP2D6 inhibitor (see WARNINGS, OVERDOSAGE ).
Acidifying Agents
Gastrointestinal acidifying agents (guanethidine, reserpine, glutamic acid HCl, ascorbic acid, fruit juices, etc.) lower absorption of amphetamines. Urinary acidifying agents (ammonium chloride, sodium acid phosphate, etc.) increase the concentration of the ionized species of the amphetamine molecule, thereby increasing urinary excretion. Both groups of agents lower blood levels and efficacy of amphetamines.
Adrenergic Blockers
Adrenergic blockers are inhibited by amphetamines.
Alkalinizing Agent
Gastrointestinal alkalinizing agents (sodium bicarbonate, etc.) increase absorption of amphetamines. Urinary alkalinizing agents (acetazolamide, some thiazides) increase the concentration of the non-ionized species of the amphetamine molecule, thereby decreasing urinary excretion. Both groups of agents increase blood levels and therefore potentiate the actions of amphetamines.
Antidepressants, Tricyclic
Amphetamines may enhance the activity of tricyclic or sympathomimetic agents; d -amphetamine with desipramine or protriptyline and possibly other tricyclics cause striking and sustained increases in the concentration of d -amphetamine in the brain; cardiovascular effects can be potentiated.
Antihistamines
Amphetamines may counteract the sedative effect of antihistamines.
Antihypertensives
Amphetamines may antagonize the hypotensive effects of antihypertensives.
Chlorpromazine
Chlorpromazine blocks dopamine and norepinephrine reuptake, thus inhibiting the central stimulant effects of amphetamines, and can be used to treat amphetamine poisoning.
Ethosuximide
Amphetamines may delay intestinal absorption of ethosuximide.
Haloperidol
Haloperidol blocks dopamine and norepinephrine reuptake, thus inhibiting the central stimulant effects of amphetamines.
Lithium Carbonate
The stimulatory effects of amphetamines may be inhibited by lithium carbonate.
Meperidine
Amphetamines potentiate the analgesic effect of meperidine.
Methenamine Therapy
Urinary excretion of amphetamines is increased, and efficacy is reduced, by acidifying agents used in methenamine therapy.
Norepinephrine
Amphetamines enhance the adrenergic effect of norepinephrine.
Phenobarbital
Amphetamines may delay intestinal absorption of phenobarbital; co-administration of phenobarbital may produce a synergistic anticonvulsant action.
Phenytoin
Amphetamines may delay intestinal absorption of phenytoin; co-administration of phenytoin may produce a synergistic anticonvulsant action.
Propoxyphene
In cases of propoxyphene overdosage, amphetamine CNS stimulation is potentiated and fatal convulsions can occur.
Veratrum Alkaloids
Amphetamines inhibit the hypotensive effect of veratrum alkaloids.
DESCRIPTION
Dextroamphetamine sulfate, USP is the dextro isomer of the compound d,l -amphetamine sulfate, a sympathomimetic amine of the amphetamine group. Chemically, dextroamphetamine is d -alpha-methylphenethylamine, and is present in all forms of dextroamphetamine sulfate, USP as the neutral sulfate. The structural formula is as follows:
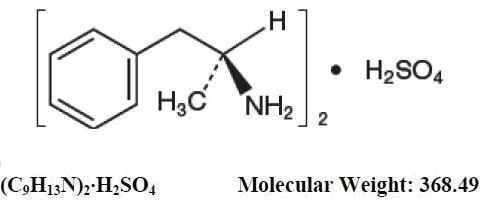
Inactive Ingredients Colloidal silicon dioxide, FD&C red #40 aluminum lake, FD&C yellow #6 aluminum lake, magnesium stearate, microcrystalline cellulose, and pregelatinized starch.
CLINICAL PHARMACOLOGY
Amphetamines are non-catecholamine, sympathomimetic amines with CNS stimulant activity. Peripheral actions include elevations of systolic and diastolic blood pressures and weak bronchodilator and respiratory stimulant action. There is neither specific evidence which clearly establishes the mechanism whereby amphetamines produce mental and behavioral effects in children, nor conclusive evidence regarding how these effects relate to the condition of the central nervous system. Pharmacokinetics The pharmacokinetics of the tablet and sustained-release capsule were compared in 12 healthy subjects. The extent of bioavailability of the sustained-release capsule was similar compared to the immediate-release tablet. Following administration of three 5 mg tablets, average maximal dextroamphetamine plasma concentrations (C max ) of 36.6 ng/mL were achieved at approximately 3 hours. Following administration of one 15 mg sustained-release capsule, maximal dextroamphetamine plasma concentrations were obtained approximately 8 hours after dosing. The average C max was 23.5 ng/mL. The average plasma T 1/2 was similar for both the tablet and sustained-release capsule and was approximately 12 hours. In 12 healthy subjects, the rate and extent of dextroamphetamine absorption were similar following administration of the sustained-release capsule formulation in the fed (58 to 75 gm fat) and fasted state.
HOW SUPPLIED
Dextroamphetamine Sulfate Tablets USP, 5 mg are light orange to orange colored, mottled, round, flat-faced, beveled edge tablets debossed with 'U38' on one side and bisect on other side and are supplied in bottles of 50, 100, and 1000.
Bottles of 50 NDC 13107-035-50 Bottles of 100 NDC 13107-035-01 Bottles of 1000 NDC 13107-035-99
Dextroamphetamine Sulfate Tablets USP, 10 mg are light orange to orange colored, mottled, round, flat-faced, beveled edge tablets debossed with 'U39' on one side and bisect on other side and are supplied in bottles of 50, 100, and 1000.
Bottles of 50 NDC 13107-036-50 Bottles of 100 NDC 13107-036-01 Bottles of 1000 NDC 13107-036-99
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature]. Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required). KEEP THIS AND ALL MEDICATIONS OUT OF THE REACH OF CHILDREN.
DEA Order Form Required Dispense with Medication Guide available at www.aurobindousa.com/medication-guides Distributed by:
Aurobindo Pharma USA, Inc. 279 Princeton-Hightstown Road East Windsor, NJ-08520
Revised: 04/2024