Get your patient on Dihydroergotamine Mesylate Nasal - Dihydroergotamine Mesylate Nasal spray, Metered (Dihydroergotamine Mesylate Nasal)
Dihydroergotamine Mesylate Nasal - Dihydroergotamine Mesylate Nasal spray, Metered prescribing information
WARNING: PERIPHERAL ISCHEMIA FOLLOWING COADMINISTRATION WITH POTENT CYP3A4 INHIBITORS
Serious and/or life-threatening peripheral ischemia has been associated with the coadministration of DIHYDROERGOTAMINE with potent CYP 3A4 inhibitors including protease inhibitors and macrolide antibiotics. Because CYP 3A4 inhibition elevates the serum levels of DIHYDROERGOTAMINE, the risk for vasospasm leading to cerebral ischemia and/or ischemia of the extremities is increased. Hence, concomitant use of these medications is contraindicated.
(See also CONTRAINDICATIONS and WARNINGS section)
INDICATIONS AND USAGE
Dihydroergotamine mesylate nasal spray is indicated for the acute treatment of migraine headaches with or without aura.
Dihydroergotamine mesylate nasal spray is not intended for the prophylactic therapy of migraine or for the management of hemiplegic or basilar migraine.
DOSAGE AND ADMINISTRATION
The solution used in dihydroergotamine mesylate nasal spray (4 mg/mL) is intended for intranasal use and must not be injected.
In clinical trials, dihydroergotamine mesylate nasal spray has been effective for the acute treatment of migraine headaches with or without aura. One spray (0.5 mg) of dihydroergotamine mesylate nasal spray should be administered in each nostril. Fifteen minutes later, an additional one spray (0.5 mg) of dihydroergotamine mesylate nasal spray should be administered in each nostril, for a total dosage of four sprays (2 mg) of dihydroergotamine mesylate nasal spray. Studies have shown no additional benefit from acute doses greater than 2 mg for a single migraine administration. The safety of doses greater than 3 mg in a 24 hour period and 4 mg in a 7 day period has not been established.
Dihydroergotamine mesylate nasal spray, should not be used for chronic daily administration.
Prior to administration, the pump must be primed (i.e., squeeze 4 times) before use (see administration instructions). Once the nasal spray applicator has been prepared, it should be discarded (with any remaining drug in opened vial) after 8 hours.
Prior to administration, the pump must be primed (i.e., squeeze 4 times) before use (See administration instructions) .
Once the nasal spray applicator has been prepared, it should be discarded (with any remaining drug in opened vial after 8 hours).
CONTRAINDICATIONS
There have been a few reports of serious adverse events associated with the coadministration of dihydroergotamine and potent CYP 3A4 inhibitors, such as protease inhibitors and macrolide antibiotics, resulting in vasospasm that led to cerebral ischemia and/or ischemia of the extremities. The use of potent CYP 3A4 inhibitors (ritonavir, nelfinavir, indinavir, erythromycin, clarithromycin, troleandomycin, ketoconazole, itraconazole) with dihydroergotamine is, therefore contraindicated (see WARNINGS: CYP 3A4 Inhibitors) .
Dihydroergotamine mesylate nasal spray should not be given to patients with ischemic heart disease (angina pectoris, history of myocardial infarction, or documented silent ischemia) or to patients who have clinical symptoms or findings consistent with coronary artery vasospasm including Prinzmetal's variant angina (see WARNINGS).
Because dihydroergotamine mesylate nasal spray may increase blood pressure, it should not be given to patients with uncontrolled hypertension.
Dihydroergotamine mesylate nasal spray , 5-HT 1 agonists (e.g., sumatriptan), ergotamine-containing or ergot-type medications or methysergide should not be used within 24 hours of each other.
Dihydroergotamine mesylate nasal spray should not be administered to patients with hemiplegic or basilar migraine.
In addition to those conditions mentioned above, dihydroergotamine mesylate nasal spray is also contraindicated in patients with known peripheral arterial disease, sepsis, following vascular surgery, and severely impaired hepatic or renal function.
Dihydroergotamine mesylate nasal spray is contraindicated in patients who have previously shown hypersensitivity to ergot alkaloids.
Dihydroergotamine mesylate should not be used with peripheral and central vasoconstrictors because the combination may result in additive or synergistic elevation of blood pressure.
ADVERSE REACTIONS
During clinical studies and the foreign postmarketing experience with dihydroergotamine mesylate nasal spray there have been no fatalities due to cardiac events.
Serious cardiac events, including some that have been fatal, have occurred following use of the parenteral form of dihydroergotamine mesylate (D.H.E. 45 ® Injection), but are extremely rare. Events reported have included coronary artery vasospasm, transient myocardial ischemia, myocardial infarction, ventricular tachycardia, and ventricular fibrillation (see CONTRAINDICATIONS, WARNINGS, and PRECAUTIONS) .
Fibrotic complications have been reported in association with long term use of injectable dihydroergotamine mesylate (see WARNINGS: Fibrotic Complications) .
Incidence in Controlled Clinical Trials
Of the 1,796 patients and subjects treated with dihydroergotamine mesylate nasal spray doses 2 mg or less in U.S. and foreign clinical studies, 26 (1.4%) discontinued because of adverse events.
The adverse events associated with discontinuation were, in decreasing order of frequency: rhinitis 13, dizziness 2, facial edema 2, and one each due to cold sweats, accidental trauma, depression, elective surgery, somnolence, allergy, vomiting, hypotension, and paraesthesia.
The most commonly reported adverse events associated with the use of dihydroergotamine mesylate nasal spray during placebo-controlled, double-blind studies for the treatment of migraine headache and not reported at an equal incidence by placebo-treated patients were rhinitis, altered sense of taste, application site reactions, dizziness, nausea, and vomiting. The events cited reflect experience gained under closely monitored conditions of clinical trials in a highly selected patient population. In actual clinical practice or in other clinical trials, these frequency estimates may not apply, as the conditions of use, reporting behavior, and the kinds of patients treated may differ.
Dihydroergotamine mesylate nasal spray was generally well tolerated. In most instances these events were transient and self-limited and did not result in patient discontinuation from a study. The following table summarizes the incidence rates of adverse events reported by at least 1% of patients who received dihydroergotamine mesylate nasal spray for the treatment of migraine headaches during placebo-controlled, double-blind clinical studies and were more frequent than in those patients receiving placebo.
| Table 3: Adverse Reaction Reported by at least 1% of the Dihydroergotamine Mesylate Nasal Spray Treated Patients and Occurred More Frequently than in the Placebo-Group in the Migraine Placebo-Controlled Trials | ||
| Dihydroergotamine mesylate nasal spray N=597 | Placebo N=631 | |
| Respiratory System | ||
| Rhinitis Pharyngitis Sinusitis | 26% 3% 1% | 7% 1% 1% |
| Gastrointestinal System | ||
| Nausea Vomiting Diarrhea | 10% 4% 2% | 4% 1% <1% |
| Special Senses, Other | ||
| Altered Sense of Taste | 8% | 1% |
| Application Site | ||
| Application Site Reaction | 6% | 2% |
| Central and Peripheral Nervous System | ||
| Dizziness Somnolence Paraesthesia | 4% 3% 2% | 2% 2% 2% |
| Body as a Whole, General | ||
| Hot Flashes Fatigue Asthenia | 1% 1% 1% | <1% 1% 0% |
| Autonomic Nervous System | ||
| Mouth Dry | 1% | 1% |
| Musculoskeletal System | ||
| Stiffness | 1% | <1% |
Other Adverse Events During Clinical Trials
In the paragraphs that follow, the frequencies of less commonly reported adverse clinical events are presented. Because the reports include events observed in open and uncontrolled studies, the role of dihydroergotamine mesylate nasal spray in their causation cannot be reliably determined. Furthermore, variability associated with adverse event reporting, the terminology used to describe adverse events, etc., limit the value of the quantitative frequency estimates provided. Event frequencies are calculated as the number of patients who used dihydroergotamine mesylate nasal spray in placebo-controlled trials and reported an event divided by the total number of patients (n=1796) exposed to dihydroergotamine mesylate nasal spray. All reported events are included except those already listed in the previous table, those too general to be informative, and those not reasonably associated with the use of the drug. Events are further classified within body system categories and enumerated in order of decreasing frequency using the following definitions: frequent adverse events are defined as those occurring in at least 1/100 patients; infrequent adverse events are those occurring in 1/100 to 1/1,000 patients; and rare adverse events are those occurring in fewer than 1/1,000 patients.
Skin and Appendages:
Infrequent: petechia, pruritus, rash, cold clammy skin;
Rare: papular rash, urticaria, herpes simplex.
Musculoskeletal:
Infrequent: cramps, myalgia, muscular weakness, dystonia;
Rare: arthralgia, involuntary muscle contractions, rigidity.
Central and Peripheral Nervous System:
Infrequent: confusion, tremor, hypoesthesia, vertigo;
Rare : speech disorder, hyperkinesia, stupor, abnormal gait, aggravated migraine.
Autonomic Nervous System: Infrequent: increased sweating.
Special Senses:
Infrequent: sense of smell altered, photophobia, conjunctivitis, abnormal lacrimation, abnormal vision, tinnitus, earache;
Rare: eye pain.
Psychiatric:
Infrequent: nervousness, euphoria, insomnia, concentration impaired;
Rare: anxiety, anorexia, depression.
Gastrointestinal:
Infrequent: abdominal pain, dyspepsia, dysphagia, hiccup;
Rare: increased salivation, esophagospasm.
Cardiovascular:
Infrequent: edema, palpitation, tachycardia;
Rare: hypotension, peripheral ischemia, angina.
Respiratory System:
Infrequent: dyspnea, upper respiratory tract infections;
Rare: bronchospasm, bronchitis, pleural pain, epistaxis.
Urinary System:
Infrequent: increased frequency of micturition, cystitis.
Reproductive, Female:
Rare: pelvic inflammation, vaginitis.
Body as a Whole - General:
Infrequent: feeling cold, malaise, rigors, fever, periorbital edema;
Rare: flu-like symptoms , shock, loss of voice, yawning .
Application Site:
Infrequent: local anesthesia.
Post-introduction Reports
Voluntary reports of adverse events temporally associated with dihydroergotamine products used in the management of migraine that have been received since the introduction of the injectable formulation are included in this section save for those already listed above. Because of their source (open and uncontrolled clinical use), whether or not events reported in association with the use of dihydroergotamine are causally related to it cannot be determined. There have been reports of pleural and retroperitoneal fibrosis in patients following prolonged daily use of injectable dihydroergotamine mesylate. Dihydroergotamine mesylate nasal spray is not recommended for prolonged daily use. (see DOSAGE AND ADMINISTRATION)
To report SUSPECTED ADVERSE REACTIONS, contact Cipla Ltd at 1-866-604-3268 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DESCRIPTION
Dihydroergotamine mesylate is ergotamine hydrogenated in the 9,10 position as the mesylate salt. Dihydroergotamine mesylate is known chemically as ergotaman-3', 6', 18-trione, 9,10-dihydro-12'-hydroxy-2'-methyl-5'- (phenylmethyl)-, (5'α)-, monomethane-sulfonate. Its molecular weight is 679.78 and its empirical formula is C 33 H 37 N 5 O 5 •CH 4 O 3 S.
The chemical structure is:
Dihydroergotamine mesylate nasal spray is provided for intranasal administration as a clear, colorless to faintly yellow solution in an amber glass vial containing:
dihydroergotamine mesylate……………4 mg
caffeine, anhydrous……………………. 10 mg
dextrose, anhydrous…………………… 50 mg
carbon dioxide………………………….qs
purified water ………………………….qs 1 mL
Each milliliter contains
Dihydroergotamine mesylate……4 mg
(equivalent to 3.43 mg dihydroergotamine)
CLINICAL PHARMACOLOGY
Mechanism of Action
Dihydroergotamine binds with high affinity to 5-HT 1Dα and 5-HT 1Dβ receptors. It also binds with high affinity to serotonin 5-HT 1A , 5-HT 2A , and 5-HT 2C receptors, noradrenaline α 2A , α 2B and α 1 receptors, and dopamine D 2L and D 3 receptors.
The therapeutic activity of dihydroergotamine in migraine is generally attributed to the agonist effect at 5-HT 1D receptors. Two current theories have been proposed to explain the efficacy of 5-HT 1D receptor agonists in migraine. One theory suggests that activation of 5-HT 1D receptors located on intracranial blood vessels, including those on arterio-venous anastomoses, leads to vasoconstriction, which correlates with the relief of migraine headache. The alternative hypothesis suggests that activation of 5-HT 1D receptors on sensory nerve endings of the trigeminal system results in the inhibition of pro-inflammatory neuropeptide release. In addition, dihydroergotamine possesses oxytocic properties.
Pharmacokinetics
Absorption
Dihydroergotamine mesylate is poorly bioavailable following oral administration. Following intranasal administration, however, the mean bioavailability of dihydroergotamine mesylate is 32% relative to the injectable administration. Absorption is variable, probably reflecting both intersubject differences of absorption and the technique used for self-administration.
Distribution
Dihydroergotamine mesylate is 93% plasma protein bound. The apparent steady-state volume of distribution is approximately 800 liters.
Metabolism
Four dihydroergotamine mesylate metabolites have been identified in human plasma following oral administration. The major metabolite, 8'-β-hydroxydihydroergotamine, exhibits affinity equivalent to its parent for adrenergic and 5-HT receptors and demonstrates equivalent potency in several venoconstrictor activity models, in vivo and in vitro . The other metabolites, i.e., dihydrolysergic acid, dihydrolysergic amide and a metabolite formed by oxidative opening of the proline ring are of minor importance. Following nasal administration, total metabolites represent only 20%-30% of plasma AUC. The systemic clearance of dihydroergotamine mesylate following I.V. and I.M. administration is 1.5 L/min. Quantitative pharmacokinetic characterization of the four metabolites has not been performed.
Excretion
The major excretory route of dihydroergotamine is via the bile in the feces. After intranasal administration the urinary recovery of parent drug amounts to about 2% of the administered dose compared to 6% after I.M. administration. The total body clearance is 1.5 L/min which reflects mainly hepatic clearance. The renal clearance (0.1 L/min) is unaffected by the route of dihydroergotamine administration. The decline of plasma dihydroergotamine is biphasic with a terminal half-life of about 10 hours.
Subpopulations
No studies have been conducted on the effect of renal or hepatic impairment, gender, race, or ethnicity on dihydroergotamine pharmacokinetics. Dihydroergotamine mesylate nasal spray is contraindicated in patients with severely impaired hepatic or renal function (see CONTRAINDICATIONS).
Interactions
The pharmacokinetics of dihydroergotamine did not appear to be significantly affected by the concomitant use of a local vasoconstrictor (e.g., fenoxazoline).
Multiple oral doses of the β-adrenoceptor antagonist propranolol, used for migraine prophylaxis, had no significant influence on the C max , T max or AUC of dihydroergotamine doses up to 4 mg.
Pharmacokinetic interactions have been reported in patients treated orally with other ergot alkaloids (e.g., increased levels of ergotamine) and macrolide antibiotics, principally troleandomycin, presumably due to inhibition of cytochrome P450 3A metabolism of the alkaloids by troleandomycin. Dihydroergotamine has also been shown to be an inhibitor of cytochrome P450 3A catalyzed reactions and rare reports of ergotism have been obtained from patients treated with dihydroergotamine and macrolide antibiotics (e.g., troleandomycin, clarithromycin, erythromycin), and in patients treated with dihydroergotamine and protease inhibitors (e.g. ritonavir), presumably due to inhibition of cytochrome P450 3A metabolism of ergotamine (see CONTRAINDICATIONS) . No pharmacokinetic interactions involving other cytochrome P450 isoenzymes are known.
Clinical Trials
The efficacy of dihydroergotamine mesylate nasal spray for the acute treatment of migraine headaches was evaluated in four randomized, double-blind, placebo-controlled studies in the U.S. The patient population for the trials was predominantly female (87%) and Caucasian (95%) with a mean age of 39 years (range 18 to 65 years). Patients treated a single moderate to severe migraine headache with a single dose of study medication and assessed pain severity over the 24 hours following treatment. Headache response was determined 0.5, 1, 2, 3 and 4 hours after dosing and was defined as a reduction in headache severity to mild or no pain. In studies 1 and 2, a four-point pain intensity scale was utilized; in studies 3 and 4, a five-point scale was used that included both pain response and restoration of function for "severe" or "incapacitating" pain, a less clear endpoint. Although rescue medication was allowed in all four studies, patients were instructed not to use them during the four-hour observation period. In studies 3 and 4, a total dose of 2 mg was compared to placebo. In studies 1 and 2, doses of 2 and 3 mg were evaluated, and showed no advantage of the higher dose for a single treatment. In all studies, patients received a regimen consisting of 0.5 mg in each nostril, repeated in 15 minutes (and again in another 15 minutes for the 3 mg dose in studies 1 and 2).
The percentage of patients achieving headache response 4 hours after treatment was significantly greater in patients receiving 2 mg doses of dihydroergotamine mesylate nasal spray compared to those receiving placebo in 3 of the 4 studies (see Tables 1 & 2 and Figures 1 & 2).
| Table 1: Studies 1 and 2: Percentage of Patients with Headache Response a 2 and 4 Hours Following a Single Treatment of Study Medication [Dihydroergotamine mesylate nasal spray or Placebo] | ||||
|---|---|---|---|---|
•• p value < 0.001 | ||||
N | 2 hours | 4 hours | ||
Study 1 | Dihydroergotamine mesylate nasal spray | 105 | 61% •• | 70% •• |
Placebo | 98 | 23% | 28% | |
Study 2 | Dihydroergotamine mesylate nasal spray | 103 | 47% | 56% • |
Placebo | 102 | 33% | 35% | |
a Headache response was defined as a reduction in headache severity to mild or no pain. Headache response was based on pain intensity as interpreted by the patient using a four-point pain intensity scale. | ||||
• p value < 0.01 | ||||
| Table 2: Studies 3 and 4: Percentage of Patients with Headache Response a 2 and 4 Hours Following a Single Treatment of Study Medication [Dihydroergotamine mesylate nasal spray or Placebo] | ||||
|---|---|---|---|---|
• p value < 0.01 | ||||
N | 2 hours | 4 hours | ||
Study 3 | Dihydroergotamine mesylate nasal spray | 50 | 32% | 48% • |
Placebo | 50 | 20% | 22% | |
Study 4 | Dihydroergotamine mesylate nasal spray | 47 | 30% | 47% |
Placebo | 50 | 20% | 30% | |
a Headache response was defined as a reduction in headache severity to mild or no pain. Headache response was evaluated on a five-point scale that included both pain response and restoration of function for "severe" or "incapacitating" pain. | ||||
Comparisons of drug performance based upon results obtained in different clinical trials are never reliable. Because studies are conducted at different times, with different samples of patients, by different investigators, employing different criteria and/or different interpretations of the same criteria, under different conditions (dose, dosing regimen, etc.), quantitative estimates of treatment response and the timing of response may be expected to vary considerably from study to study.
The Kaplan-Meier plots below (Figures 1 & 2) provides an estimate of the probability that a patient will have responded to a single 2 mg dose of dihydroergotamine mesylate nasal spray as a function of the time elapsed since initiation of treatment.
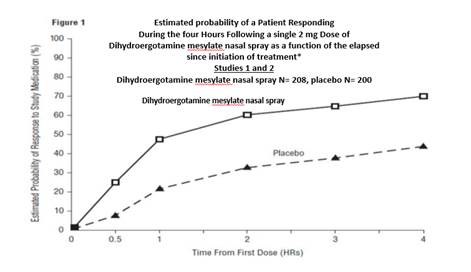
•The figure shows the probability over time of obtaining a response following treatment with dihydroergotamine mesylate nasal spray. Headache response was based on pain intensity as interpreted by the patient using a four-point pain intensity scale. Patients not achieving response within 4 hours were censored to 4 hours.
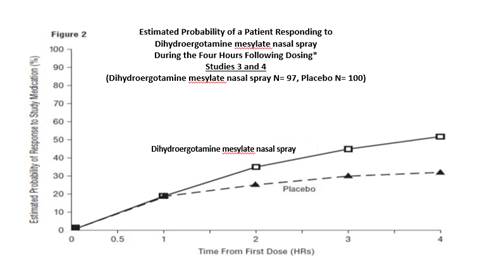
•The figure shows the probability over time of obtaining a response following treatment with dihydroergotamine mesylate nasal spray. Headache response was evaluated on a five-point scale that confounded pain response and restoration of function for "severe" or "incapacitating" pain. Patients not achieving response within 4 hours were censored to 4 hours.
For patients with migraine-associated nausea, photophobia, and phonophobia at baseline, there was a lower incidence of these symptoms at 2 and 4 hours following administration of dihydroergotamine mesylate nasal spray compared to placebo.
Patients were not allowed to use additional treatments for eight hours prior to study medication dosing and during the four-hour observation period following study treatment. Following the 4-hour observation period, patients were allowed to use additional treatments. For all studies, the estimated probability of patients using additional treatments for their migraines over the 24 hours following the single 2 mg dose of study treatment is summarized in Figure 3 below.
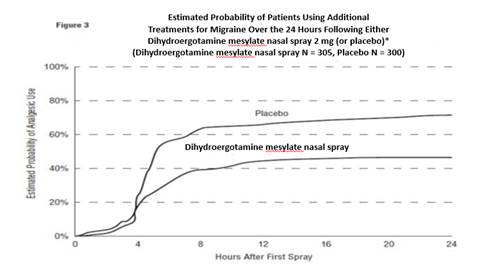
•Kaplan-Meier plot based on data obtained from all studies with patients not using additional treatments censored to 24 hours. All patients received a single treatment of study medication for their migraine attack. The plot also includes patients who had no response to the initial dose.
Neither age nor sex appear to affect the patient's response to dihydroergotamine mesylate nasal spray. While patients with menstrual migraine, migraine with aura, and migraine without aura by medical history were included in the clinical evaluation of dihydroergotamine mesylate nasal spray, patients were not required to report the specific type of migraine treated with study medication. Thus, neither the effect of menses on migraine nor the presence or the absence of aura were assessed. The racial distribution of patients was insufficient to determine the effect of race on the efficacy of dihydroergotamine mesylate nasal spray.
HOW SUPPLIED
Dihydroergotamine mesylate nasal spray is available (as a clear, colorless to faintly yellow solution) in 3.5 mL amber glass vials containing 4 mg of dihydroergotamine mesylate.
Dihydroergotamine mesylate nasal spray is provided as a package of 8 units, administration instruction sheet, and one package insert. Each unit consists of one vial and one sprayer. (NDC 69097-503-31). Each carton contains eight such units. (NDC 69097-503-27).
Store below 25°C (77°F). Do not refrigerate or freeze.
Disclaimer: Other brands listed are the registered trademarks of their respective owners and are not trademarks of Cipla Limited.
Manufactured by:
Mipharm, S.p.A.
Milan, Italy
Manufactured for:
Cipla USA, Inc.
10 Independence Boulevard, Suite 300
Warren, NJ 07059
Revised: 5/2022
Mechanism of Action
Dihydroergotamine binds with high affinity to 5-HT 1Dα and 5-HT 1Dβ receptors. It also binds with high affinity to serotonin 5-HT 1A , 5-HT 2A , and 5-HT 2C receptors, noradrenaline α 2A , α 2B and α 1 receptors, and dopamine D 2L and D 3 receptors.
The therapeutic activity of dihydroergotamine in migraine is generally attributed to the agonist effect at 5-HT 1D receptors. Two current theories have been proposed to explain the efficacy of 5-HT 1D receptor agonists in migraine. One theory suggests that activation of 5-HT 1D receptors located on intracranial blood vessels, including those on arterio-venous anastomoses, leads to vasoconstriction, which correlates with the relief of migraine headache. The alternative hypothesis suggests that activation of 5-HT 1D receptors on sensory nerve endings of the trigeminal system results in the inhibition of pro-inflammatory neuropeptide release. In addition, dihydroergotamine possesses oxytocic properties.