Get your patient on Elucirem - Gadopiclenol injection (Gadopiclenol)
Elucirem - Gadopiclenol injection prescribing information
WARNING: RISK ASSOCIATED WITH INTRATHECAL USE and NEPHROGENIC SYSTEMIC FIBROSIS
Risk Associated with Intrathecal Use Intrathecal administration of gadolinium-based contrast agents (GBCAs) can cause serious adverse reactions including death, coma, encephalopathy, and seizures. ELUCIREM is not approved for intrathecal use [see Warnings and Precautions (5.1 )] .
Nephrogenic Systemic Fibrosis GBCAs increase the risk for nephrogenic systemic fibrosis (NSF) among patients with impaired elimination of the drugs. Avoid use of ELUCIREM in these patients unless the diagnostic information is essential and not available with non-contrasted MRI or other modalities. NSF may result in fatal or debilitating fibrosis affecting the skin, muscle and internal organs. The risk for NSF appears highest among patients with:
- Chronic, severe kidney disease (GFR < 30 mL/min/1.73 m 2 ), or
- Acute kidney injury.
Screen patients for acute kidney injury and other conditions that may reduce renal function. For patients at risk for chronically reduced renal function (e.g. age > 60 years, hypertension, diabetes), estimate the glomerular filtration rate (GFR) through laboratory testing.
For patients at highest risk for NSF, do not exceed the recommended ELUCIREM dose and allow a sufficient period of time for elimination of the drug from the body prior to any re-administration [see Warnings and Precautions (5.2 )] .
RECENT MAJOR CHANGES
INDICATIONS AND USAGE
ELUCIREM is indicated in adult and pediatric patients, including term neonates, for use with magnetic resonance imaging (MRI) to detect and visualize lesions with abnormal vascularity in:
- the central nervous system (brain, spine, and associated tissues),
- the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system).
DOSAGE AND ADMINISTRATION
Recommended Dosage
The recommended dose of ELUCIREM for adult and pediatric patients, including term neonates, is 0.05 mmol/kg actual body weight (equivalent to 0.1 mL/kg) administered intravenously at approximately 2 mL/sec.
Administration and Imaging Instructions
- Administer ELUCIREM as an intravenous bolus injection, manually or by compatible power injector, at approximately 2 mL/sec followed by a flush of 0.9% sodium chloride injection. For pediatric patients, adjust the flow rate and flush volume based on age.
- Use aseptic technique for all handling and administration of ELUCIREM.
- Visually inspect ELUCIREM for particulate matter and discoloration prior to administration. Do not use the solution if any particulate matter is present or the solution is discolored.
- Do not mix with other medications because of the potential for chemical incompatibility.
- Prime intravenous line before use.
- Contrast MRI can begin immediately following the injection of ELUCIREM.
Directions for Use of Single-Dose Vial and Pre-filled Syringe
Vial
- Pierce the rubber stopper only once.
- Aseptically draw up ELUCIREM into a disposable syringe and use immediately.
- If solidification occurs in the vial due to cold exposure, bring the vial of ELUCIREM to room temperature before use and inspect to ensure that the solution is clear and colorless to yellow without any particulate matter or discoloration.
- Discard any unused portion.
Pre-filled syringe
- Remove the tip cap of the syringe, screw the plunger rod and use immediately.
- All luer connections should be gently hand tightened without over tightening, to ensure secure connections and to prevent damage to the device.
- Pre-filled syringes must not be frozen. Frozen pre-filled syringes of ELUCIREM should be discarded.
- Discard any unused portion.
Directions for Use of Pharmacy Bulk Package
- ELUCIREM Pharmacy Bulk Package (PBP) is not for direct infusion.
- Perform the transfer of ELUCIREM from the PBP in an aseptic work area, such as laminar flow hood, using aseptic technique and suitable transfer device for filling empty sterile syringes.
- Penetrate the closure only one time. Once the container closure is punctured, do not remove the PBP from the aseptic work area.
- Use each individual dose of ELUCIREM promptly following withdrawal from the PBP.
- Use the contents of the PBP within 24 hours at room temperature after puncture.
- If solidification occurs in the PBP due to cold exposure, bring the PBP of ELUCIREM to room temperature before use and inspect to ensure that the solution is clear and colorless to yellow without any particulate matter or discoloration.
Directions for Use of Imaging Bulk Package
- ELUCIREM Imaging Bulk Package (IBP) is not for direct infusion.
- The IBP is for use only with an automated contrast injection system, contrast management system, or contrast media transfer set approved or cleared for use with this contrast agent in this IBP. This allows for the administration of multiple single doses of ELUCIREM to multiple patients.
- See drug and device labeling for information on devices indicated for use with this IBP and techniques to help assure safe use.
- The ELUCIREM IBP is to be used only in a room designated for performing radiological procedures that involve administration of a contrast agent.
- Utilize aseptic technique for penetrating the container closure of the IBP and transferring ELUCIREM.
- Penetrate the container closure only one time with a suitable sterile component of the automated contrast injection system, contrast management system, or contrast media transfer set (e.g., transfer spike) approved or cleared for use with this IBP.
- During the entire period of use, ensure that the contents of the ELUCIREM IBP container remain in continuous contact with the automated contrast injector system, contrast management system, or contrast media transfer set. To ensure the protection of the contrast media against any possible contamination, do not remove the dispensing set from the IBP container closure.
- Once the ELUCIREM IBP container is punctured, do not remove it from the work area. Store the ELUCIREM IBP at 25° C (77° F); excursions permitted from 15°C to 30°C (59°F to 86°F) [see USP Controlled Room Temperature].
- Maximum use time from puncture is 24 hours. Discard any unused ELUCIREM 24 hours after puncture of the IBP.
- After the container closure is punctured, if the integrity of IBP and the delivery system cannot be assured through direct continuous supervision, the IBP and all associated disposables for the automated contrast injection system, contrast management system, or contrast media transfer set should be discarded.
- If solidification occurs in the IBP due to cold exposure, bring the IBP of ELUCIREM to room temperature before use and inspect to ensure that the solution is clear and colorless to yellow without any particulate matter or discoloration.
DOSAGE FORMS AND STRENGTHS
Injection: 0.5 mmol/mL of gadopiclenol as a clear, colorless to yellow aqueous solution available as:
Strength | Packaging |
| Single-dose vials (glass) |
| Single-dose prefilled syringes (plastic) |
| Pharmacy bulk package (glass) |
| Imaging Bulk Package (glass) |
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no available data on ELUCIREM use in pregnant women to evaluate for a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. GBCAs cross the placenta and result in fetal exposure. In human placental imaging studies, contrast was visualized in the placenta and fetal tissues after maternal GBCA administration. Based on animal studies, use of GBCAs during pregnancy may result in fetal gadolinium retention.
Published epidemiological studies on the association between GBCAs and adverse fetal outcomes have reported inconsistent findings and have important methodological limitations (see Data) . In animal reproduction studies, there were no adverse developmental effects observed in rats or rabbits with intravenous administration of ELUCIREM during organogenesis (see Data) . Because of the potential risks of gadolinium to the fetus, use ELUCIREM only if imaging is essential during pregnancy and cannot be delayed.
The background risk of major birth defects and miscarriage for the indicated population(s) are unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20% respectively.
Data Human Data
Available data regarding exposure to GBCAs during pregnancy from published epidemiological studies are not sufficient to assess the potential risk of adverse fetal and neonatal effects that may be associated with GBCAs. A retrospective cohort study of over 1.4 million pregnancies in Ontario, Canada, comparing pregnant women who had a GBCA MRI to pregnant women who did not have an MRI, reported a higher occurrence of stillbirths and neonatal deaths in the group receiving GBCA MRI. Limitations of this study include a lack of comparison with non-contrast MRI and lack of information about the maternal indication for MRI. Another retrospective cohort study of over 11 million pregnancies in the Medicaid database found no increased risk of fetal or neonatal death or Neonatal Intensive Care Unit admission when comparing pregnancies exposed to GBCA MRI versus non-contrast MRI. These two retrospective observational studies assessed a limited number of potential pregnancy outcomes and did not evaluate the full spectrum of potential fetal risk.
Animal Data
Gadolinium Retention
GBCAs administered to pregnant non-human primates (0.1 mmol/kg on gestational days 85 and 135) result in measurable gadolinium concentration in the offspring in bone, brain, skin, liver, kidney, and spleen for at least 7 months. GBCAs administered to pregnant mice (2 mmol/kg daily on gestational days 16 through 19) result in measurable gadolinium concentrations in the pups in bone, brain, kidney, liver, blood, muscle, and spleen at one-month postnatal age.
Reproductive Toxicology
Animal reproduction studies conducted with gadopiclenol showed some signs of maternal toxicity in rats at 10 mmol/kg and rabbits at 5 mmol/kg (corresponding to 52 times and 57 times the recommended human dose, respectively). This maternal toxicity was characterized in both species by swelling, decreased activity, and lower gestation weight gain and food consumption.
No effect on embryo-fetal development was observed in rats at 10 mmol/kg (corresponding to 52 times the recommended human dose). In rabbits, a lower mean fetal body weight was observed at 5 mmol/kg (corresponding to 57 times the recommended human dose) and this was attributed as a consequence of the lower gestation weight gain.
Lactation
Risk Summary There are no data on the presence of gadopiclenol in human milk, the effects on the breastfed infant, or the effects on milk production. However, published lactation data on other GBCAs indicate that 0.01% to 0.04% of the maternal gadolinium dose is excreted in breast milk. Additionally, there is limited GBCA gastrointestinal absorption in the breast-fed infant. Gadopiclenol is present in rat milk. When a drug is present in animal milk, it is likely that the drug will be present in human milk (see Data) . The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ELUCIREM and any potential adverse effects on the breastfed infant from ELUCIREM or from the underlying maternal condition.
Data In lactating rats receiving single intravenous injection of [ 153 Gd]-gadopiclenol, 0.3% and 0.2% of the total administered radioactivity was transferred to the pups via maternal milk at 6 hours and 24 hours after administration, respectively. Furthermore, in nursing rat pups, oral absorption of gadopiclenol was 3.6%.
Pediatric Use
The safety and effectiveness of ELUCIREM for use with MRI to detect and visualize lesions with abnormal vascularity in the CNS (brain, spine, and associated tissues), and the body (head and neck, thorax, abdomen, pelvis, and musculoskeletal system) have been established in pediatric patients including term neonates.
Use of ELUCIREM in this age group is supported by evidence from adequate and well-controlled studies in adults, with additional pharmacokinetic and safety data from two open-label, single-arm, multicenter, single-dose studies (i.e., Trials 1 and 2) of ELUCIREM (0.05 mmol/kg) in 116 pediatric patients who underwent CNS and body MRI. Trial 1 (NCT03749252) included 80 pediatric patients aged 2 to 17 years, and Trial 2 (NCT05590884) included 36 pediatric patients aged 25 days to less than 2 years [see Adverse Reactions (6.1 ), Clinical Pharmacology (12.3 ) and Clinical Studies (14.2 , 14.3 )] .
The safety of ELUCIREM has not been established in preterm neonates.
Geriatric Use
Of the total number of ELUCIREM-treated patients in clinical studies, 270 (26%) patients were 65 years of age and over, while 62 (6%) patients were 75 years of age and over. No overall differences in safety or efficacy were observed between these subjects and younger subjects.
This drug is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, it may be useful to monitor renal function.
Renal impairment
In patients with renal impairment, the exposure of gadopiclenol is increased compared to patients with normal renal function. This may increase the risk of adverse reactions such as nephrogenic systemic fibrosis (NSF). Avoid use of GBCAs among these patients unless the diagnostic information is essential and not available with non-contrast MRI or other modalities. No dose adjustment of ELUCIREM is recommended for patients with renal impairment. ELUCIREM can be removed from the body by hemodialysis [see Warnings and Precautions (5.2 , 5.4 , 5.5 ) and Clinical Pharmacology (12.3 )].
CONTRAINDICATIONS
ELUCIREM is contraindicated in patients with history of hypersensitivity reactions to ELUCIREM.
WARNINGS AND PRECAUTIONS
Risk Associated with Intrathecal Use
Intrathecal administration of GBCAs can cause serious adverse reactions including death, coma, encephalopathy, and seizures. The safety and effectiveness of ELUCIREM have not been established with intrathecal use. ELUCIREM is not approved for intrathecal use [see Dosage and Administration (2.1 )] .
Nephrogenic Systemic Fibrosis
GBCAs increase the risk for nephrogenic systemic fibrosis (NSF) among patients with impaired elimination of the drugs. Avoid use of ELUCIREM among these patients unless the diagnostic information is essential and not available with non-contrast MRI or other modalities. The GBCA-associated NSF risk appears highest for patients with chronic, severe kidney disease (GFR <30 mL/min/1.73 m 2 ) as well as patients with acute kidney injury. The risk appears lower for patients with chronic, moderate kidney disease (GFR 30-59 mL/min/1.73 m 2 ) and little, if any, for patients with chronic, mild kidney disease (GFR 60-89 mL/min/1.73 m 2 ). NSF may result in fatal or debilitating fibrosis affecting the skin, muscle, and internal organs. Report any diagnosis of NSF following ELUCIREM administration to Guerbet LLC (1-877-729-6679) or FDA (1-800-FDA-1088 or www.fda.gov/medwatch).
Screen patients for acute kidney injury and other conditions that may reduce renal function. Features of acute kidney injury consist of rapid (over hours to days) and usually reversible decrease in kidney function, commonly in the setting of surgery, severe infection, injury or drug-induced kidney toxicity. Serum creatinine levels and estimated GFR may not reliably assess renal function in the setting of acute kidney injury. For patients at risk for chronically reduced renal function (e.g., age >60 years, diabetes mellitus or chronic hypertension), estimate the GFR through laboratory testing.
Among the factors that may increase the risk for NSF are repeated or higher than recommended doses of a GBCA and the degree of renal impairment at the time of exposure. Record the specific GBCA and the dose administered to a patient. For patients at highest risk for NSF, do not exceed the recommended ELUCIREM dose and allow a sufficient period of time for elimination of the drug prior to re-administration. For patients receiving hemodialysis, physicians may consider the prompt initiation of hemodialysis following the administration of a GBCA in order to enhance the contrast agent’s elimination [see Use in Specific Populations (8.6 ) and Clinical Pharmacology (12.3 )]. The usefulness of hemodialysis in the prevention of NSF is unknown.
Hypersensitivity Reactions
With GBCAs, serious hypersensitivity reactions have occurred. In most cases, initial symptoms occurred within minutes of GBCA administration and resolved with prompt emergency treatment.
- Before ELUCIREM administration, assess all patients for any history of a reaction to contrast media, bronchial asthma and/or allergic disorders. These patients may have an increased risk for a hypersensitivity reaction to ELUCIREM.
- ELUCIREM is contraindicated in patients with history of hypersensitivity reactions to ELUCIREM [see Contraindications (4 )] .
- Administer ELUCIREM only in situations where trained personnel and therapies are promptly available for the treatment of hypersensitivity reactions, including personnel trained in resuscitation.
- During and following ELUCIREM administration, observe patients for signs and symptoms of hypersensitivity reactions.
Gadolinium Retention
Gadolinium is retained for months or years in several organs. The highest concentrations (nanomoles per gram of tissue) have been identified in the bone, followed by other organs (e.g. brain, skin, kidney, liver, and spleen). The duration of retention also varies by tissue and is longest in bone. Linear GBCAs cause more retention than macrocyclic GBCAs. At equivalent doses, gadolinium retention varies among the linear agents with gadodiamide causing greater retention than other linear agents such as gadoxetate disodium and gadobenate dimeglumine. Retention is lowest and similar among the macrocyclic GBCAs such as gadoterate meglumine, gadobutrol, gadoteridol, and gadopiclenol.
Consequences of gadolinium retention in the brain have not been established. Pathologic and clinical consequences of GBCA administration and retention in skin and other organs have been established in patients with impaired renal function [see Warnings and Precautions (5.2 )] . There are rare reports of pathologic skin changes in patients with normal renal function. Adverse events involving multiple organ systems have been reported in patients with normal renal function without an established causal link to gadolinium [see Adverse Reactions (6.2 )] .
While clinical consequences of gadolinium retention have not been established in patients with normal renal function, certain patients might be at higher risk. These include patients requiring multiple lifetime doses, pregnant and pediatric patients, and patients with inflammatory conditions. Consider the retention characteristics of the agent when choosing a GBCA for these patients. Minimize repetitive GBCA imaging studies, particularly closely spaced studies, when possible.
Acute Kidney Injury
In patients with chronically reduced renal function, acute kidney injury requiring dialysis has occurred with the use of GBCAs. The risk of acute kidney injury may increase with increasing dose of the contrast agent. Do not exceed the recommended dose.
Extravasation and Injection Site Reactions
Injection site reactions such as injection site pain have been reported in the clinical studies with ELUCIREM [see Adverse Reactions (6.1 )] . Extravasation during ELUCIREM administration may result in tissue irritation [see Nonclinical Toxicology (13.2 )] . Ensure catheter and venous patency before the injection of ELUCIREM.
Interference with Visualization of Lesions Visible with Non-Contrast MRI
As with any GBCA, ELUCIREM may impair the visualization of lesions seen on non-contrast MRI. Therefore, caution should be exercised when Gadopiclenol MRI scans are interpreted without a companion non-contrast MRI scan.
ADVERSE REACTIONS
The following clinically significant adverse reactions are discussed elsewhere in labeling:
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of ELUCIREM was evaluated in 1,083 patients who received ELUCIREM at doses ranging from 0.025 mmol/kg (one half the recommended dose) to 0.3 mmol/kg (six times the recommended dose). A total of 744 patients (including 116 pediatric patients) received the recommended dose of 0.05 mmol/kg. Among patients who received the recommended dose, the average age was 49 years (range from less than one month to 88 years) and 55% were female. The race distribution was 80% White, 10% Asian, 6% American Indian or Alaska native, 2% Black, and 2% patients of other or unspecified race groups.
Overall, approximately 4.6% of subjects receiving the labeled dose reported one or more adverse reactions.
Table 1 lists adverse reactions that occurred in > 0.2% of patients who received 0.05 mmol/kg ELUCIREM.
Adverse Reaction | ELUCIREM 0.05 mmol/kg (n=744) (%) |
Injection site pain | 0.7 |
Headache | 0.7 |
Nausea | 0.4 |
Injection site warmth | 0.4 |
Injection site coldness | 0.3 |
Dizziness | 0.3 |
Localized swelling | 0.3 |
Erythema | 0.3 |
Adverse reactions that occurred with a frequency ≤ 0.2% in patients who received 0.05 mmol/kg ELUCIREM included: maculopapular rash, vomiting, worsened renal impairment, feeling hot, pyrexia, oral paresthesia, dysgeusia, diarrhea, pruritus, allergic dermatitis, injection site paresthesia, Cystatin C increase, and blood creatinine increase.
Adverse Reactions in Pediatric Patients
The overall safety profile observed in pediatric patients was similar to the safety profile of adult patients [see Use in Specific Populations (8.4 )] .
Postmarketing Experience
The following additional adverse reactions have been identified during postmarketing use of ELUCIREM or other GBCAs. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Gastrointestinal Disorders: Acute pancreatitis with onset within 48 hours after GBCA administration.
General Disorders and Administration Site Conditions: Fatigue, asthenia, pain syndromes, and heterogeneous clusters of symptoms in the neurological, cutaneous, and musculoskeletal systems with variable onset and duration after GBCA administration [see Warnings and Precautions (5.4 )] .
Respiratory, Thoracic and Mediastinal Disorders: Acute respiratory distress syndrome, pulmonary edema.
Skin Disorders: Gadolinium-associated plaques
DESCRIPTION
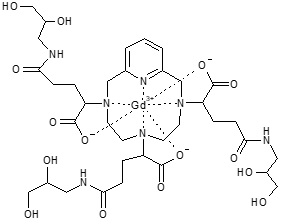
ELUCIREM (gadopiclenol) injection is a paramagnetic macrocyclic non-ionic gadolinium-based contrast agent for intravenous use.
The chemical name for gadopiclenol is rac -[(2R,2'Ξ,2''Ξ)-2,2',2''-(3,6,9-triaza-κ 3 N 3 ,N 6 ,N 9 -1(2,6)-pyridina-κN 1 -cyclodecaphane-3,6,9-triyl)tris(5-{[(2Ξ)-2,3-dihydroxypropyl]amino}-5-oxopentanoato-κ 3 O 1 ,O 1 ',O 1 '')(3−)]gadolinium with a molecular weight of 970.11 g/mol and a molecular formula of 970.11 g/mol and a molecular formula of C 35 H 54 GdN 7 O 15
ELUCIREM is a sterile, nonpyrogenic, clear, colorless to yellow aqueous solution.
Each mL contains 485.1 mg (0.5 mmol) of gadopiclenol (containing 0.5 mmol of gadolinium) and the following inactive ingredients: 0.404 mg tetraxetan, 1.211 mg trometamol, hydrochloric acid and/or sodium hydroxide (for pH adjustment, if needed), and water for injection.
The main physicochemical properties of ELUCIREM are provided in Table 2.
Parameter | Value |
Density at 20°C | 1.211 g/cm 3 |
Mean viscosity at 20°C | 12.6 mPa.s |
Mean viscosity at 37°C | 7.6 mPa.s |
Osmolality at 37°C | 850 mOsm/kg water |
pH | 7.0 – 7.8 |
CLINICAL PHARMACOLOGY
Mechanism of Action
Gadopiclenol is a paramagnetic molecule (macrocyclic non-ionic complex of gadolinium) that develops a magnetic moment when placed in a magnetic field. The magnetic moment alters the relaxation rates of water protons in its vicinity in the body, leading to an increase in signal intensity (brightness) of tissues.
Pharmacodynamics
In MRI, visualization of normal and pathological tissue depends in part on variations in the radiofrequency signal intensity that occur with:
- differences in proton density
- differences of the spin-lattice or longitudinal relaxation times (T 1 )
- differences in the spin-spin or transverse relaxation time (T 2 ).
When placed in a magnetic field (patient in MRI machine), gadopiclenol shortens the T 1 and T 2 relaxation times in targeted tissues. The extent to which a contrast agent can affect the relaxation rate of tissue water (1/T 1 or 1/T 2 ) is termed relaxivity (r 1 or r 2 ). The relaxivity of GBCAs is presented in Table 3.
Gadolinium-Chelate | r 1 (L.mmol -1 .s -1 ) |
Gadobenic acid | 6.3 |
Gadobutrol | 5.2 |
Gadodiamide | 4.3 |
Gadopiclenol | 12.8 |
Gadoteric acid | 3.6 |
Gadoteridol | 4.1 |
Gadoxetic acid | 6.9 |
Cardiac Electrophysiology At 6 times the recommended dosage in adult patients, gadopiclenol does not prolong the QT interval to any clinically relevant extent.
Pharmacokinetics
The C max and AUC inf of gadopiclenol increased proportionally over a dosage range from 0.025 mmol/kg to 0.3 mmol/kg (0.5 times to 6 times the recommended dosage). At the recommended dose, the mean (CV%) C max and AUC inf were 525 (13%) µg/mL and 569 (18%) µg·h/mL, respectively.
Distribution After intravenous administration of ELUCIREM, gadopiclenol is distributed in the extracellular fluids.
The mean (CV%) volume of distribution of gadopiclenol at steady state is 13 (13%) L.
Protein binding of gadopiclenol is ≤ 1.8% at clinically relevant concentrations.
Following GBCA administration, gadolinium is present for months or years in brain, bone, skin, and other organs [see Warnings and Precautions (5.4 )] . It is unknown whether the recommended dose of ELUCIREM results in similar or different levels of gadolinium retention relative to those of other approved macrocyclic GBCAs at their recommended doses.
Elimination
The mean (CV%) elimination half-life (t 1/2 ) of gadopiclenol is 1.5 (14%) hour.
The mean (CV%) total body clearance (CL) and renal clearance (CL r ) of gadopiclenol are 100 (9.5%) mL/min and 81 (35%) mL/min, respectively.
Metabolism Gadopiclenol is not metabolized.
Excretion Gadopiclenol is mainly eliminated through the kidneys by glomerular filtration. Approximately 98% of the dose was recovered in urine within 48 hours after administration.
Specific Populations
No clinically significant differences in the pharmacokinetics of gadopiclenol were observed based on sex.
Pediatric Patients
The pharmacokinetics of gadopiclenol in pediatric patients were within the range of those in adults (>18 years of age) [see Dosage and Administration (2.1 )] .
The pharmacokinetic parameters (median (range)) of gadopiclenol by age group are presented in Table 4.
0 to < 2 years N= 35 a | 2 to 6 years N= 19 a | 7 to 11 years N= 19 a | 12 to <18 years N= 18 a | Adults N= 9 a | |
AUC 0-inf (µg∙h/mL) | 395 [186 ;777] | 465 [282; 764] | 575 [370; 792] | 638 [462; 1040] | 572 [409; 695] |
t 1/2 (h) | 1.51 [0.9 ;2.5] | 1.75 [1.2; 2.5] | 1.61 [1.3; 2.2] | 1.78 [1.4; 5.0] | 1.62 [1.2; 3.0] |
C 10 min (µg/mL) | 223 [142 ;367] | 280 [229; 374] | 328 [281; 439] | 407 [307; 499] | 364 [241; 390] |
C 20 min (µg/mL) | 162 [101 ;269] | 195 [139; 250] | 234 [180; 290] | 256 [210; 302] | 241 [191; 281] |
CL (L/h/kg) | 0.12 [0.06 ;0.25] | 0.10 [0.07; 0.17] | 0.08 [0.06; 0.13] | 0.08 [0.05; 0.11] | 0.08 b [0.06; 0.13] |
a At the recommended dose
b In 54 adults at a dose of 0.025 mmol/kg to 0.3 mmol/kg [0.5 times to 6 times the recommended dose]
Adults with Renal Impairment
The pharmacokinetic parameters (mean (%CV)) of gadopiclenol in patients with renal impairment are presented in Table 5.
Normal (eGFR ≥ 90 mL/min) | Mild (eGFR 60 to < 90 mL/min) | Moderate (eGFR 30 to < 60 mL/min) | Severe (eGFR 15 to < 30 mL/min) | |
AUC inf (µg·h/mL) | 1113 (24%) | 1711 (31%) | 2759 (28%) | 9671 (18%) |
CL r (mL/min) | 96 (10%) | 76 (23%) | 44 (25%) | 14 (26%) |
t 1/2 (h) | 1.9 | 3.3 | 3.8 | 11.7 |
a Following administration of a single gadopiclenol 0.1 mmol/kg dose (2 times the recommended dosage). b eGFR: estimate of GFR based on an estimation equation and expressed in mL/min. To convert mL/min/1.73 m 2 to mL/min, multiply by the individual’s BSA and divide by 1.73.
In patients with mild or moderate renal impairment, more than 90% of the administered ELUCIREM was recovered in urine within 48 hours. In patients with severely impaired renal function about 84% of the administered ELUCIREM was recovered in urine within 5 days.
In patients with eGFR < 15 mL/min, hemodialysis effectively removed gadopiclenol from plasma as the percentage of decrease in blood concentrations was 95 to 98% at the end of the first hemodialysis session and 100% after the third hemodialysis session [see Warnings and Precautions (5.2 ), Use in Specific Populations (8.6 )].
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis No carcinogenicity studies of gadopiclenol were performed.
Mutagenesis Gadopiclenol did not demonstrate mutagenic potential in in vitro bacterial reverse mutation assays (Ames test), in an in vitro chromosome aberration assay in Chinese hamster ovary cells nor in an in vivo rat micronucleus assay.
Impairment of Fertility Gadopiclenol had no effect on fertility and general reproductive performance of male and female rats when given at dose up to 10 mmol/kg (corresponding to 62 times the recommended human dose).
Animal Toxicology
Local intolerance reactions, including slight to moderate erythema and edema, were observed after perivenous injection in rabbits suggesting the possibility of local irritation if the contrast medium leaks around the veins in a clinical setting [see Warnings and Precautions (5.6 )] .
CLINICAL STUDIES
Overview of Clinical Studies
The safety and effectiveness of ELUCIREM for lesion visualization were evaluated in two prospective, double blind, randomized, crossover clinical studies. Study 1 (NCT03996447) was performed in adults with known or highly suspected CNS lesions with focal areas of disruption of the blood-brain barrier. Study 2 (NCT03986138) was performed in adults with suspected enhancing abnormalities in at least one body region among the head and neck, thorax, abdomen, pelvis, and musculoskeletal system.
In each study, patients received both ELUCIREM 0.05 mmol/kg and gadobutrol 0.1 mmol/kg (as an active comparator) in random order separated by 2 days to 14 days. Magnetic resonance imaging was performed before and after administration of each contrast agent.
Pre-contrast and paired (consisting of both pre-contrast and post-contrast images for the same drug) image sets were independently evaluated by three central readers who were blinded to identity of the contrast agent. Readers scored up to three lesions per patient for border delineation, internal morphology, and contrast enhancement, each on a scale from 1 to 4. The total number of lesions was also reported. An additional independent central reader performed lesion tracking to allow matching of lesions between pre-contrast and paired images.
The analysis compared the patient-level average score for matching lesions for each visualization parameter between pre-contrast and paired image sets.
Visualization of CNS Lesions
Study 1 included 256 patients with known or highly suspected CNS lesion(s). Among the enrolled patients, 239 had assessable pre-contrast and paired images with at least one matching lesion for at least one reader. These patients had a mean age of 57 years (range: 18 years to 84 years), 52% were female, and 83% were White.
All three blinded readers’ evaluations of paired pre-contrast plus post-contrast images and pre-contrast images alone for all lesion visualization criteria, the pre-specified co-primary efficacy endpoints, are presented in Table 6.
n | LS Mean (SE) | 95% CI Difference | |||
Paired | Pre-contrast | Difference• | |||
Border delineation | |||||
Reader 1 | 227 | 3.90 (0.02) | 2.08 (0.02) | 1.82 (0.03) | (1.76, 1.88) |
Reader 2 | 229 | 3.64 (0.04) | 1.74 (0.04) | 1.90 (0.05) | (1.81, 2.00) |
Reader 3 | 202 | 3.97 (0.03) | 2.61 (0.03) | 1.36 (0.04) | (1.29, 1.44) |
Internal morphology | |||||
Reader 1 | 227 | 3.92 (0.03) | 1.66 (0.03) | 2.26 (0.03) | (2.20, 2.33) |
Reader 2 | 229 | 3.65 (0.03) | 1.88 (0.03) | 1.77 (0.04) | (1.69, 1.85) |
Reader 3 | 202 | 3.97 (0.04) | 2.01 (0.04) | 1.96 (0.05) | (1.85, 2.06) |
Degree of contrast enhancement | |||||
Reader 1 | 227 | 3.77 (0.03) | 1.00 (0.03) | 2.77 (0.04) | (2.69, 2.85) |
Reader 2 | 229 | 3.58 (0.03) | 1.00 (0.03) | 2.58 (0.05) | (2.49, 2.67) |
Reader 3 | 202 | 3.90 (0.02) | 1.00 (0.02) | 2.90 (0.03) | (2.84, 2.95) |
LS: Least Squares; SE: Standard Error; CI: Confidence Interval. Only matching lesions are considered. The mixed models based on the full analysis set (N=239) include lesion visualization factor as dependent variable, MRI modality (Precontrast and Paired MRI) as fixed factors, and patient as a random factor. •p<0.0001 for all rows
Gadopiclenol lesion visualization scores and number of lesions identified per patient were similar to those for gadobutrol.
Visualization of Body Lesions
Study 2 included 304 patients presenting with known or suspected enhancing abnormality(ies) and/or lesion(s) in at least one region among the head and neck, musculoskeletal system including extremities, and body including thorax, abdomen, and pelvis. Among the enrolled patients, 278 had assessable pre-contrast and paired images with at least one matching lesion for at least one reader. These patients had a mean age of 57 years (range: 21 years to 86 years), 59% were female, and 71% were White.
Three readers assessed images of the head and neck, three other readers assessed images of the musculoskeletal system, and another three readers assessed other areas collectively referred to as the body (thorax, abdomen, and pelvis). Lesion visualization scores by reader in each anatomic region at patient-level as supportive analyses are summarized in Table 7.
Table 7. Patient-Level Body Lesion Visualization Scores by Reader and Anatomic Region, Paired vs. Pre-contrast in Patients Receiving ELUCIREM 0.05 mmol/kg Intravenously
n | LS Mean (SE) | 95% CI difference | |||
Paired | Pre-contrast | Difference | |||
Head & Neck | |||||
Border delineation | |||||
Reader 1 | 15 | 3.71 (0.10) | 2.13 (0.10) | 1.58 (0.14) | (1.30, 1.86) |
Reader 2 | 19 | 3.53 (0.18) | 2.11 (0.18) | 1.42 (0.18) | (1.06, 1.78) |
Reader 3 | 13 | 3.92 (0.13) | 2.85 (0.13) | 1.08 (0.13) | (0.82, 1.33) |
Internal morphology | |||||
Reader 1 | 15 | 3.80 (0.07) | 1.87 (0.07) | 1.93 (0.10) | (1.74, 2.12) |
Reader 2 | 19 | 3.74 (0.14) | 2.05 (0.14) | 1.68 (0.16) | (1.37, 2.00) |
Reader 3 | 13 | 3.92 (0.12) | 2.54 (0.12) | 1.38 (0.14) | (1.10, 1.67) |
Degree of contrast enhancement | |||||
Reader 1 | 15 | 3.60 (0.11) | 1.00 (0.11) | 2.60 (0.16) | (2.29, 2.91) |
Reader 2 | 19 | 3.68 (0.16) | 1.00 (0.16) | 2.68 (0.22) | (2.22, 3.15) |
Reader 3 | 13 | 3.92 (0.11) | 1.00 (0.11) | 2.92 (0.15) | (2.61, 3.24) |
Musculoskeletal system (including extremities) | |||||
Border delineation | |||||
Reader 1 | 17 | 3.00 (0.10) | 2.06 (0.10) | 0.94 (0.13) | (0.68, 1.20) |
Reader 2 | 17 | 2.68 (0.20) | 2.44 (0.20) | 0.24 (0.19) | (-0.15, 0.62) |
Reader 3 | 21 | 2.81 (0.10) | 2.05 (0.10) | 0.76 (0.10) | (0.56, 0.96) |
Internal morphology | |||||
Reader 1 | 17 | 3.00 (0.07) | 2.00 (0.07) | 1.00 (0.09) | (0.82, 1.18) |
Reader 2 | 17 | 3.94 (0.15) | 2.35 (0.15) | 1.59 (0.17) | (1.25, 1.92) |
Reader 3 | 21 | 2.90 (0.09) | 2.05 (0.09) | 0.86 (0.11) | (0.64, 1.08) |
Degree of contrast enhancement | |||||
Reader 1 | 17 | 2.82 (0.10) | 1.00 (0.10) | 1.82 (0.15) | (1.53, 2.12) |
Reader 2 | 17 | 3.33 (0.17) | 1.00 (0.17) | 2.33 (0.24) | (1.847, 2.82) |
Reader 3 | 21 | 3.06 (0.08) | 1.00 (0.08) | 2.06 (0.12) | (1.82, 2.31) |
Body (thorax, abdomen, pelvis) | |||||
Border delineation | |||||
Reader 1 | 219 | 3.86 (0.03) | 2.28 (0.03) | 1.57 (0.04) | (1.50, 1.64) |
Reader 2 | 194 | 3.54 (0.06) | 3.15 (0.06) | 0.40 (0.06) | (0.29, 0.51) |
Reader 3 | 228 | 3.53 (0.03) | 1.69 (0.03) | 1.84 (0.03) | (1.78, 1.90) |
Internal morphology | |||||
Reader 1 | 219 | 3.86 (0.02) | 2.00 (0.02) | 1.87 (0.03) | (1.82, 1.92) |
Reader 2 | 194 | 3.74 (0.05) | 3.41 (0.05) | 0.33 (0.05) | (0.23, 0.43) |
Reader 3 | 228 | 3.78 (0.03) | 1.60 (0.03) | 2.17 (0.03) | (2.11, 2.24) |
Degree of contrast enhancement | |||||
Reader 1 | 219 | 3.71 (0.03) | 1.00 (0.03) | 2.71 (0.04) | (2.63, 2.79) |
Reader 2 | 194 | 2.69 (0.05) | 1.00 (0.05) | 1.69 (0.07) | (1.54, 1.83) |
Reader 3 | 228 | 3.33 (0.03) | 1.00 (0.03) | 2.33 (0.44) | (2.25, 2.40) |
LS: Least Squares; SE: Standard Error; CI: Confidence Interval. Only matching lesions are considered. The mixed models based on the full analysis set (N=278) include lesion visualization factor as a dependent variable, patient as a random factor, and MRI modality (Pre-contrast and Paired MRI), body regions, and MRI body regions as fixed factors.
Gadopiclenol lesion visualization scores and number of lesions identified per patient were similar to those for gadobutrol.
HOW SUPPLIED/STORAGE AND HANDLING
HOW SUPPLIED
ELUCIREM (gadopiclenol) injection is a clear, colorless to yellow aqueous solution supplied in the following presentations:
Strength | Sale Unit | NDC |
Single-Dose Vial (glass) | ||
1.5 mmol/3 mL (0.5 mmol/mL) | Carton of 1 | 67684-4230-1 |
Carton of 10 | 67684-4230-2 | |
3.75 mmol/7.5 mL (0.5 mmol/mL) | Carton of 1 | 67684-4231-1 |
Carton of 10 | 67684-4231-2 | |
5 mmol/10 mL (0.5 mmol/mL) | Carton of 1 | 67684-4232-1 |
Carton of 10 | 67684-4232-2 | |
7.5 mmol/15 mL (0.5 mmol/mL) | Carton of 1 | 67684-4233-1 |
Carton of 10 | 67684-4233-2 | |
Single-Dose Prefilled Syringe (plastic) | ||
3.75 mmol/7.5 mL (0.5 mmol/mL) | Carton of 1 | 67684-4240-1 |
Carton of 10 | 67684-4240-2 | |
5 mmol/10 mL (0.5 mmol/mL) | Carton of 1 | 67684-4241-1 |
Carton of 10 | 67684-4241-2 | |
7.5 mmol/15 mL (0.5 mmol/mL) | Carton of 1 | 67684-4242-1 |
Carton of 10 | 67684-4242-2 | |
Pharmacy Bulk Package (glass) | ||
15 mmol/30 mL (0.5 mmol/mL) | Carton of 1 | 67684-4250-1 |
Carton of 25 | 67684-4250-2 | |
25 mmol/50 mL (0.5 mmol/mL) | Carton of 1 | 67684-4250-3 |
Carton of 25 | 67684-4250-4 | |
50 mmol/100 mL (0.5 mmol/mL) | Carton of 1 | 67684-4250-5 |
Carton of 6 | 67684-4250-6 | |
Carton of 12 | 67684-4250-7 | |
Imaging Bulk Package (glass) | ||
15 mmol/30 mL (0.5 mmol/mL) | Carton of 1 | 67684-4251-1 |
Carton of 25 | 67684-4251-2 | |
25 mmol/50 mL (0.5 mmol/mL) | Carton of 1 | 67684-4251-3 |
Carton of 25 | 67684-4251-4 | |
50 mmol/100 mL (0.5 mmol/mL) | Carton of 1 | 67684-4251-5 |
Carton of 6 | 67684-4251-6 | |
Carton of 12 | 67684-4251-7 | |
Storage and Handling Store at 25°C (77°F); excursions permitted from 15°C to 30°C (59°F to 86°F) [see USP, Controlled Room Temperature].
Do not freeze Pre-filled syringes.
Mechanism of Action
Gadopiclenol is a paramagnetic molecule (macrocyclic non-ionic complex of gadolinium) that develops a magnetic moment when placed in a magnetic field. The magnetic moment alters the relaxation rates of water protons in its vicinity in the body, leading to an increase in signal intensity (brightness) of tissues.