Fingolimod
Fingolimod Prescribing Information
Warnings and Precautions (
Leukoencephalopathy
At the first sign or symptom suggestive of PML, withhold fingolimod and perform an appropriate diagnostic evaluation. Typical symptoms associated with PML are diverse, progress over days to weeks, and include progressive weakness on one side of the body or clumsiness of limbs, disturbance of vision, and changes in thinking, memory, and orientation leading to confusion and personality changes.
Magnetic resonance imaging (MRI) findings may be apparent before clinical signs or symptoms. Cases of PML, diagnosed based on MRI findings and the detection of JCV DNA in the cerebrospinal fluid in the absence of clinical signs or symptoms specific to PML, have been reported in patients treated with MS medications associated with PML, including fingolimod. Many of these patients subsequently became symptomatic with PML. Therefore, monitoring with MRI for signs that may be consistent with PML may be useful, and any suspicious findings should lead to further investigation to allow for an early diagnosis of PML, if present. Lower PML-related mortality and morbidity have been reported following discontinuation of another MS medication associated with PML in patients with PML who were initially asymptomatic compared to patients with PML who had characteristic clinical signs and symptoms at diagnosis. It is not known whether these differences are due to early detection and discontinuation of MS treatment or due to differences in disease in these patients.
Severe increase in disability accompanied by multiple new lesions on MRI has been reported after discontinuation of fingolimod in the postmarketing setting. Patients in most of these reported cases did not return to the functional status they had before stopping fingolimod. The increase in disability generally occurred within 12 weeks after stopping fingolimod, but was reported up to 24 weeks after fingolimod discontinuation.
Monitor patients for development of severe increase in disability following discontinuation of fingolimod and begin appropriate treatment as needed.
Fingolimod capsules are indicated for the treatment of relapsing forms of multiple sclerosis (MS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in patients 10 years of age and older.
Fingolimod capsules are available as:
- 0.5 mg hard gelatin capsule with a yellow cap and white opaque body, imprinted with “TV” (over) “7820” in black ink on both the cap and body. The capsule is filled with white to off-white powder, with small agglomerates.
Fingolimod is contraindicated in patients who have:
- in the last 6 months experienced myocardial infarction, unstable angina, stroke, transient ischemic attack (TIA), decompensated heart failure requiring hospitalization or Class III/IV heart failure
- a history or presence of Mobitz Type II second-degree or third-degree AV block or sick sinus syndrome, unless patient has a functioning pacemaker [see Warnings and Precautions ()]
5.1 Bradyarrhythmia and
Atrioventricular BlocksBecause of a risk for bradyarrhythmia and AV blocks, patients should be monitored during fingolimod treatment initiation
[see Dosage and Administration ].Reduction in Heart RateAfter the first dose of fingolimod, the heart rate decrease starts within an hour. On Day 1, the maximum decline in heart rate generally occurs within 6 hours and recovers, although not to baseline levels, by 8 to 10 hours postdose. Because of physiological diurnal variation, there is a second period of heart rate decrease within 24 hours after the first dose. In some patients, heart rate decrease during the second period is more pronounced than the decrease observed in the first 6 hours. Heart rates below 40 bpm in adults, and below 50 bpm in pediatric patients occurred rarely. In controlled clinical trials in adult patients, adverse reactions of symptomatic bradycardia following the first dose were reported in 0.6% of patients receiving fingolimod 0.5 mg and in 0.1% of patients on placebo. Patients who experienced bradycardia were generally asymptomatic, but some patients experienced hypotension, dizziness, fatigue, palpitations, and/or chest pain that usually resolved within the first 24 hours on treatment.Patients with some preexisting conditions (e.g., ischemic heart disease, history of myocardial infarction, congestive heart failure, history of cardiac arrest, cerebrovascular disease, uncontrolled hypertension, history of symptomatic bradycardia, history of recurrent syncope, severe untreated sleep apnea, AV block, sinoatrial heart block) may poorly tolerate the fingolimod-induced bradycardia, or experience serious rhythm disturbances after the first dose of fingolimod. Prior to treatment with fingolimod, these patients should have a cardiac evaluation by a physician appropriately trained to conduct such evaluation, and if treated with fingolimod, should be monitored overnight with continuous ECG in a medical facility after the first dose.
Since initiation of fingolimod treatment, results in decreased heart rate and may prolong the QT interval, patients with a prolonged QTc interval (>450 msec adult and pediatric males, >470 msec adult females, or >460 msec pediatric females) before dosing or during 6-hour observation, or at additional risk for QT prolongation (e.g., hypokalemia, hypomagnesemia, congenital long-QT syndrome), or on concurrent therapy with QT prolonging drugs with a known risk of torsades de pointes (e.g., citalopram, chlorpromazine, haloperidol, methadone, erythromycin) should be monitored overnight with continuous ECG in a medical facility.
Following the second dose, a further decrease in heart rate may occur when compared to the heart rate prior to the second dose, but this change is of a smaller magnitude than that observed following the first dose. With continued dosing, the heart rate returns to baseline within 1 month of chronic treatment. Clinical data indicate effects of fingolimod on heart rate are maximal after the first dose although milder effects on heart rate may persist for, on average, 2 to 4 weeks after initiation of therapy at which time heart rate generally returns to baseline. Physicians should continue to be alert to patient reports of cardiac symptoms.
Atrioventricular BlocksInitiation of fingolimod treatment has resulted in transient AV conduction delays. In controlled clinical trials in adult patients, first-degree AV block after the first dose occurred in 4.7% of patients receiving fingolimod and 1.6% of patients on placebo. In a study of 697 patients with available 24-hour Holter monitoring data after their first dose (N=351 receiving fingolimod and N=346 on placebo), second-degree AV blocks (Mobitz Types I [Wenckebach] or 2:1 AV blocks) occurred in 4% (N=14) of patients receiving fingolimod and 2% (N=7) of patients on placebo. Of the 14 patients receiving fingolimod, 7 patients had 2:1 AV block (5 patients within the first 6 hours postdose and 2 patients after 6 hours postdose). All second-degree AV blocks on placebo were Mobitz Type I and occurred after the first 12 hours postdose. The conduction abnormalities were usually transient and asymptomatic, and resolved within the first 24 hours on treatment, but they occasionally required treatment with atropine or isoproterenol.
Postmarketing ExperienceIn the postmarketing setting, third-degree AV block and AV block with junctional escape have been observed during the first-dose 6-hour observation period with fingolimod. Isolated delayed onset events, including transient asystole and unexplained death, have occurred within 24 hours of the first dose. These events were confounded by concomitant medications and/or preexisting disease, and the relationship to fingolimod is uncertain. Cases of syncope were also reported after the first dose of fingolimod.
- a baseline QTc interval ≥500 msec
- cardiac arrhythmias requiring anti-arrhythmic treatment with Class Ia or Class III anti-arrhythmic drugs
- had a hypersensitivity reaction to fingolimod or any of the excipients in fingolimod. Observed reactions include rash, urticaria and angioedema upon treatment initiation [see Warnings and Precautions (.)]
5.14 Hypersensitivity
ReactionsHypersensitivity reactions, including rash, urticaria, and angioedema have been reported with fingolimod in the postmarketing setting. Fingolimod is contraindicated in patients with history of hypersensitivity to fingolimod or any of its excipients
[see Contraindications ].
The following serious adverse reactions are described elsewhere in labeling:
- Bradyarrhythmia and Atrioventricular Blocks [see Warnings and Precautions ()]
5.1 Bradyarrhythmia and
Atrioventricular BlocksBecause of a risk for bradyarrhythmia and AV blocks, patients should be monitored during fingolimod treatment initiation
[see Dosage and Administration ].Reduction in Heart RateAfter the first dose of fingolimod, the heart rate decrease starts within an hour. On Day 1, the maximum decline in heart rate generally occurs within 6 hours and recovers, although not to baseline levels, by 8 to 10 hours postdose. Because of physiological diurnal variation, there is a second period of heart rate decrease within 24 hours after the first dose. In some patients, heart rate decrease during the second period is more pronounced than the decrease observed in the first 6 hours. Heart rates below 40 bpm in adults, and below 50 bpm in pediatric patients occurred rarely. In controlled clinical trials in adult patients, adverse reactions of symptomatic bradycardia following the first dose were reported in 0.6% of patients receiving fingolimod 0.5 mg and in 0.1% of patients on placebo. Patients who experienced bradycardia were generally asymptomatic, but some patients experienced hypotension, dizziness, fatigue, palpitations, and/or chest pain that usually resolved within the first 24 hours on treatment.Patients with some preexisting conditions (e.g., ischemic heart disease, history of myocardial infarction, congestive heart failure, history of cardiac arrest, cerebrovascular disease, uncontrolled hypertension, history of symptomatic bradycardia, history of recurrent syncope, severe untreated sleep apnea, AV block, sinoatrial heart block) may poorly tolerate the fingolimod-induced bradycardia, or experience serious rhythm disturbances after the first dose of fingolimod. Prior to treatment with fingolimod, these patients should have a cardiac evaluation by a physician appropriately trained to conduct such evaluation, and if treated with fingolimod, should be monitored overnight with continuous ECG in a medical facility after the first dose.
Since initiation of fingolimod treatment, results in decreased heart rate and may prolong the QT interval, patients with a prolonged QTc interval (>450 msec adult and pediatric males, >470 msec adult females, or >460 msec pediatric females) before dosing or during 6-hour observation, or at additional risk for QT prolongation (e.g., hypokalemia, hypomagnesemia, congenital long-QT syndrome), or on concurrent therapy with QT prolonging drugs with a known risk of torsades de pointes (e.g., citalopram, chlorpromazine, haloperidol, methadone, erythromycin) should be monitored overnight with continuous ECG in a medical facility.
Following the second dose, a further decrease in heart rate may occur when compared to the heart rate prior to the second dose, but this change is of a smaller magnitude than that observed following the first dose. With continued dosing, the heart rate returns to baseline within 1 month of chronic treatment. Clinical data indicate effects of fingolimod on heart rate are maximal after the first dose although milder effects on heart rate may persist for, on average, 2 to 4 weeks after initiation of therapy at which time heart rate generally returns to baseline. Physicians should continue to be alert to patient reports of cardiac symptoms.
Atrioventricular BlocksInitiation of fingolimod treatment has resulted in transient AV conduction delays. In controlled clinical trials in adult patients, first-degree AV block after the first dose occurred in 4.7% of patients receiving fingolimod and 1.6% of patients on placebo. In a study of 697 patients with available 24-hour Holter monitoring data after their first dose (N=351 receiving fingolimod and N=346 on placebo), second-degree AV blocks (Mobitz Types I [Wenckebach] or 2:1 AV blocks) occurred in 4% (N=14) of patients receiving fingolimod and 2% (N=7) of patients on placebo. Of the 14 patients receiving fingolimod, 7 patients had 2:1 AV block (5 patients within the first 6 hours postdose and 2 patients after 6 hours postdose). All second-degree AV blocks on placebo were Mobitz Type I and occurred after the first 12 hours postdose. The conduction abnormalities were usually transient and asymptomatic, and resolved within the first 24 hours on treatment, but they occasionally required treatment with atropine or isoproterenol.
Postmarketing ExperienceIn the postmarketing setting, third-degree AV block and AV block with junctional escape have been observed during the first-dose 6-hour observation period with fingolimod. Isolated delayed onset events, including transient asystole and unexplained death, have occurred within 24 hours of the first dose. These events were confounded by concomitant medications and/or preexisting disease, and the relationship to fingolimod is uncertain. Cases of syncope were also reported after the first dose of fingolimod.
- Infections [see Warnings and Precautions ()]
5.2 InfectionsRisk of InfectionsFingolimod causes a dose-dependent reduction in peripheral lymphocyte count to 20% to 30% of baseline values because of reversible sequestration of lymphocytes in lymphoid tissues. Fingolimod may therefore increase the risk of infections, some serious in nature
[see Clinical Pharmacology ]. Life-threatening and fatal infections have occurred in association with fingolimod.Before initiating treatment with fingolimod, a recent CBC (i.e., within 6 months or after discontinuation of prior therapy) should be available. Consider suspending treatment with fingolimod if a patient develops a serious infection, and reassess the benefits and risks prior to reinitiation of therapy. Because the elimination of fingolimod after discontinuation may take up to 2 months, continue monitoring for infections throughout this period. Instruct patients receiving fingolimod to report symptoms of infections to a physician. Patients with active acute or chronic infections should not start treatment until the infection(s) is resolved.
In MS placebo-controlled trials in adult patients, the overall rate of infections (72%) with fingolimod was similar to placebo. However, bronchitis, herpes zoster, influenza, sinusitis, and pneumonia were more common in fingolimod-treated patients. Serious infections occurred at a rate of 2.3% in the fingolimod group versus 1.6% in the placebo group.
In the postmarketing setting, serious infections with opportunistic pathogens, including viruses (e.g., John Cunningham virus [JCV], herpes simplex viruses 1 and 2, varicella zoster virus), fungi (e.g., cryptococci), and bacteria (e.g., atypical mycobacteria) have been reported with fingolimod. Patients with symptoms and signs consistent with any of these infections should undergo prompt diagnostic evaluation and appropriate treatment.
Herpes Viral InfectionsIn placebo-controlled trials in adult patients, the rate of herpetic infections was 9% in patients receiving fingolimod 0.5 mg and 7% on placebo.
Two patients died of herpetic infections during controlled trials. One death was due to disseminated primary herpes zoster and the other was to herpes simplex encephalitis. In both cases, the patients were taking a 1.25 mg dose of fingolimod (higher than the recommended 0.5 mg dose) and had received high-dose corticosteroid therapy to treat suspected MS relapses.
Serious, life-threatening events of disseminated varicella zoster and herpes simplex infections, including cases of encephalitis and multiorgan failure, have occurred with fingolimod in the postmarketing setting. Include disseminated herpetic infections in the differential diagnosis of patients who are receiving fingolimod and present with an atypical MS relapse or multiorgan failure.
Cases of Kaposi’s sarcoma have been reported in the postmarketing setting. Kaposi’s sarcoma is an angioproliferative disorder that is associated with infection with human herpes virus 8 (HHV-8). Patients with symptoms or signs consistent with Kaposi’s sarcoma should be referred for prompt diagnostic evaluation and management.
Cryptococcal InfectionsCryptococcal infections, including cases of fatal cryptococcal meningitis and disseminated cryptococcal infections, have been reported with fingolimod in the postmarketing setting. Cryptococcal infections have generally occurred after approximately 2 years of fingolimod treatment, but may occur earlier. The relationship between the risk of cryptococcal infection and the duration of treatment is unknown. Patients with symptoms and signs consistent with a cryptococcal infection should undergo prompt diagnostic evaluation and treatment.
Prior and Concomitant Treatment with Antineoplastic, Immunosuppressive, or Immune-Modulating TherapiesIn clinical studies, patients who received fingolimod did not receive concomitant treatment with antineoplastic, non-corticosteroid immunosuppressive, or immune-modulating therapies used for treatment of MS. Concomitant use of fingolimod with any of these therapies, and also with corticosteroids, would be expected to increase the risk of immunosuppression
[see Drug Interactions ].When switching to fingolimod from immune-modulating or immunosuppressive medications, consider the duration of their effects and their mode of action to avoid unintended additive immunosuppressive effects.
Varicella Zoster Virus Antibody Testing/VaccinationPatients without a healthcare professional confirmed history of chickenpox or without documentation of a full course of vaccination against VZV should be tested for antibodies to VZV before initiating fingolimod. VZV vaccination of antibody-negative patients is recommended prior to commencing treatment with fingolimod, following which initiation of treatment with fingolimod should be postponed for 1 month to allow the full effect of vaccination to occur
[see Drug Interactions , Use in Specific Populations ].Human Papilloma Virus InfectionHuman papilloma virus (HPV) infections, including papilloma, dysplasia, warts, and HPV-related cancer, have been reported in patients treated with fingolimod in the postmarketing setting. Vaccination against HPV should be considered prior to treatment initiation with fingolimod, taking into account vaccination recommendations. Cancer screening, including Papanicolaou (Pap) test, is recommended as per standard of care for patients using an immunosuppressive therapy.
- Progressive Multifocal Leukoencephalopathy [see Warnings and Precautions ()]
5.3 Progressive Multifocal
LeukoencephalopathyCases of progressive multifocal leukoencephalopathy (PML) have occurred in patients with MS who received fingolimod in the postmarketing setting. PML is an opportunistic viral infection of the brain caused by the JC virus (JCV) that typically only occurs in patients who are immunocompromised, and that usually leads to death or severe disability. PML has occurred in patients who had not been treated previously with natalizumab, which has a known association with PML, were not taking any other immunosuppressive or immunomodulatory medications concomitantly, and did not have any ongoing systemic medical conditions resulting in compromised immune system function. Longer treatment duration increases the risk of PML in fingolimod-treated patients; the majority of cases have occurred in patients treated with fingolimod for at least 18 months.At the first sign or symptom suggestive of PML, withhold fingolimod and perform an appropriate diagnostic evaluation. Typical symptoms associated with PML are diverse, progress over days to weeks, and include progressive weakness on one side of the body or clumsiness of limbs, disturbance of vision, and changes in thinking, memory, and orientation leading to confusion and personality changes.
Magnetic resonance imaging (MRI) findings may be apparent before clinical signs or symptoms. Cases of PML, diagnosed based on MRI findings and the detection of JCV DNA in the cerebrospinal fluid in the absence of clinical signs or symptoms specific to PML, have been reported in patients treated with MS medications associated with PML, including fingolimod. Many of these patients subsequently became symptomatic with PML. Therefore, monitoring with MRI for signs that may be consistent with PML may be useful, and any suspicious findings should lead to further investigation to allow for an early diagnosis of PML, if present. Lower PML-related mortality and morbidity have been reported following discontinuation of another MS medication associated with PML in patients with PML who were initially asymptomatic compared to patients with PML who had characteristic clinical signs and symptoms at diagnosis. It is not known whether these differences are due to early detection and discontinuation of MS treatment or due to differences in disease in these patients.
If PML is confirmed, treatment with fingolimod should be discontinued.Immune reconstitution inflammatory syndrome (IRIS) has been reported in patients treated with S1P receptor modulators, including fingolimod, who developed PML and subsequently discontinued treatment. IRIS presents as a clinical decline in the patient’s condition that may be rapid, can lead to serious neurological complications or death, and is often associated with characteristic changes on MRI. The time to onset of IRIS in patients with PML was generally within a few months after S1P receptor modulator discontinuation. Monitoring for development of IRIS and appropriate treatment of the associated inflammation should be undertaken. - Macular Edema [see Warnings and Precautions ()]
5.4 Macular EdemaS1P receptor modulators, including fingolimod, have been associated with an increased risk of macular edema. Obtain a baseline evaluation of the fundus, including the macula, near the start of treatment with fingolimod. Perform an examination of the fundus, including the macula, 3 to 4 months after starting treatment, periodically while on therapy, and any time there is a change in vision.A dose-dependent increase in the risk of macular edema occurred in the fingolimod clinical development program.
In 2-year double-blind, placebo-controlled studies in adult patients with multiple sclerosis, macular edema with or without visual symptoms occurred in 1.5% of patients (11/799) treated with fingolimod 1.25 mg, 0.5% of patients (4/783) treated with fingolimod 0.5 mg, and 0.4% of patients (3/773) treated with placebo. Macular edema occurred predominantly during the first 3 to 4 months of therapy. These clinical trials excluded patients with diabetes mellitus, a known risk factor for macular edema (see below
Macular Edema in Patients with History of Uveitis or Diabetes Mellitus). Symptoms of macular edema included blurred vision and decreased visual acuity. Routine ophthalmological examination detected macular edema in some patients with no visual symptoms. Macular edema generally partially or completely resolved with or without treatment after drug discontinuation. Some patients had residual visual acuity loss even after resolution of macular edema. Macular edema has also been reported in patients taking fingolimod in the postmarketing setting, usually within the first 6 months of treatment.Continuation of fingolimod in patients who develop macular edema has not been evaluated. Macular edema over an extended period of time (i.e., 6 months) can lead to permanent visual loss. Consider discontinuing fingolimod if macular edema develops; this decision should include an assessment of the potential benefits and risks for the individual patient. The risk of recurrence after rechallenge has not been evaluated.Macular Edema in Patients with History of Uveitis or Diabetes MellitusPatients with a history of uveitis and patients with diabetes mellitus are at increased risk of macular edema during fingolimod therapy. In the combined clinical trial experience in adult patients with all doses of fingolimod, the rate of macular edema was higher in MS patients with a history of uveitis compared to those without a history of uveitis (approximately 20% versus 0.6%, respectively). Fingolimod has not been tested in MS patients with diabetes mellitus. - Liver Injury [see Warnings and Precautions ()]
5.5 Liver InjuryClinically significant liver injury has occurred in patients treated with fingolimod in the postmarketing setting. Signs of liver injury, including markedly elevated serum hepatic enzymes and elevated total bilirubin, have occurred as early as ten days after the first dose and have also been reported after prolonged use. Cases of acute liver failure requiring liver transplant have been reported.
In 2-year placebo-controlled clinical trials in adult patients, elevation of liver enzymes (ALT, AST, and GGT) to 3-fold the upper limit of normal (ULN) or greater occurred in 14% of patients treated with fingolimod 0.5 mg and 3% of patients on placebo. Elevations 5-fold the ULN or greater occurred in 4.5% of patients on fingolimod and 1% of patients on placebo. The majority of elevations occurred within 6 to 9 months. In clinical trials, fingolimod was discontinued if the elevation exceeded 5 times the ULN. Serum transaminase levels returned to normal within approximately 2 months after discontinuation of fingolimod. Recurrence of liver transaminase elevations occurred with rechallenge in some patients.
Prior to starting treatment with fingolimod (within 6 months), obtain serum transaminases (ALT and AST) and total bilirubin levels. Obtain transaminase levels and total bilirubin levels periodically until two months after fingolimod discontinuation.
Patients should be monitored for signs and symptoms of any hepatic injury. Measure liver transaminase and bilirubin levels promptly in patients who report symptoms that may indicate liver injury, including new or worsening fatigue, anorexia, right upper abdominal discomfort, dark urine, or jaundice. In this clinical context, if the patient is found to have an alanine aminotransferase (ALT) greater than three times the reference range with serum total bilirubin greater than two times the reference range, treatment with fingolimod should be interrupted. Treatment should not be resumed if a plausible alternative etiology for the signs and symptoms cannot be established, because these patients are at risk for severe drug-induced liver injury.
Because fingolimod exposure is doubled in patients with severe hepatic impairment, these patients should be closely monitored, as the risk of adverse reactions is greater
[see Use in Specific Populations , Clinical Pharmacology ]. - Posterior Reversible Encephalopathy Syndrome [see Warnings and Precautions ()]
5.6 Posterior Reversible Encephalopathy SyndromeThere have been rare cases of posterior reversible encephalopathy syndrome (PRES) reported in adult patients receiving fingolimod. Symptoms reported included sudden onset of severe headache, altered mental status, visual disturbances, and seizure. Symptoms of PRES are usually reversible but may evolve into ischemic stroke or cerebral hemorrhage. Delay in diagnosis and treatment may lead to permanent neurological sequelae. If PRES is suspected, fingolimod should be discontinued.
- Respiratory Effects [see Warnings and Precautions ()]
5.7 Respiratory EffectsDose-dependent reductions in forced expiratory volume over 1 second (FEV1) and diffusion lung capacity for carbon monoxide (DLCO) were observed in patients treated with fingolimod as early as 1 month after treatment initiation. In 2-year placebo-controlled trials in adult patients, the reduction from baseline in the percent of predicted values for FEV1 at the time of last assessment on drug was 2.8% for fingolimod 0.5 mg and 1.0% for placebo. For DLCO, the reduction from baseline in percent of predicted values at the time of last assessment on drug was 3.3% for fingolimod 0.5 mg and 0.5% for placebo. The changes in FEV1 appear to be reversible after treatment discontinuation. There is insufficient information to determine the reversibility of the decrease of DLCO after drug discontinuation. In MS placebo-controlled trials in adult patients, dyspnea was reported in 9% of patients receiving fingolimod 0.5 mg and 7% of patients receiving placebo. Several patients discontinued fingolimod because of unexplained dyspnea during the extension (uncontrolled) studies. Fingolimod has not been tested in MS patients with compromised respiratory function.
Spirometric evaluation of respiratory function and evaluation of DLCO should be performed during therapy with fingolimod if clinically indicated.
- Fetal Risk [see Warnings and Precautions ()]
5.8 Fetal RiskBased on findings from animal studies, fingolimod may cause fetal harm when administered to a pregnant woman. In animal reproduction studies conducted in rats and rabbits, developmental toxicity was observed with administration of fingolimod at doses less than the recommended human dose. Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Because it takes approximately 2 months to eliminate fingolimod from the body, advise females of reproductive potential to use effective contraception to avoid pregnancy during and for 2 months after stopping fingolimod treatment
[see Use in Specific Populations ]. - Severe Increase in Disability After Stopping Fingolimod [see Warnings and Precautions ()]
5.9 Severe Increase in Disability After Stopping FingolimodSevere increase in disability accompanied by multiple new lesions on MRI has been reported after discontinuation of fingolimod in the postmarketing setting. Patients in most of these reported cases did not return to the functional status they had before stopping fingolimod. The increase in disability generally occurred within 12 weeks after stopping fingolimod, but was reported up to 24 weeks after fingolimod discontinuation.
Monitor patients for development of severe increase in disability following discontinuation of fingolimod and begin appropriate treatment as needed.
After stopping fingolimod in the setting of PML, monitor for development of immune reconstitution inflammatory syndrome (PML-IRIS)[see Warnings and Precautions ]. - Tumefactive Multiple Sclerosis [see Warnings and Precautions ()]
5.10 Tumefactive Multiple SclerosisMS relapses with tumefactive demyelinating lesions on imaging have been observed during fingolimod therapy and after fingolimod discontinuation in the postmarketing setting. Most reported cases of tumefactive MS in patients receiving fingolimod have occurred within the first 9 months after fingolimod initiation, but tumefactive MS may occur at any point during treatment. Cases of tumefactive MS have also been reported within the first 4 months after fingolimod discontinuation. Tumefactive MS should be considered when a severe MS relapse occurs during fingolimod treatment, especially during initiation, or after discontinuation of fingolimod, prompting imaging evaluation and initiation of appropriate treatment.
- Increased Blood Pressure [see Warnings and Precautions ()]
5.11 Increased Blood PressureIn adult MS controlled clinical trials, patients treated with fingolimod 0.5 mg had an average increase over placebo of approximately 3 mmHg in systolic pressure, and approximately 2 mmHg in diastolic pressure, first detected after approximately 1 month of treatment initiation, and persisting with continued treatment. Hypertension was reported as an adverse reaction in 8% of patients on fingolimod 0.5 mg and in 4% of patients on placebo. Blood pressure (BP) should be monitored during treatment with fingolimod.
- Malignancies[see Warnings and Precautions ()]
5.12 MalignanciesCutaneous MalignanciesThe risk of cutaneous malignancies (including basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and melanoma) is increased in patients treated with S1P receptor modulators. Use of fingolimod has been associated with an increased risk of BCC and melanoma.In two-year placebo-controlled trials in adult patients, the incidence of BCC was 2% in patients on fingolimod 0.5 mg and 1% in patients on placebo[see Adverse Reactions ]. Melanoma, basal cell carcinoma, squamous cell carcinoma, Kaposi’s sarcoma[see Warnings and Precautions ],and Merkel cell carcinoma have been reported with fingolimod in the postmarketing setting.Skin examinations are recommended prior to or shortly after the start of treatment and periodically thereafter for all patients, particularly those with risk factors for skin cancer. Providers and patients are advised to monitor for suspicious skin lesions. If a suspicious skin lesion is observed, it should be promptly evaluated. As usual for patients with increased risk for skin cancer, exposure to sunlight and ultraviolet light should be limited by wearing protective clothing and using a sunscreen with a high protection factor. Concomitant phototherapy with UV-B radiation or PUVA photochemotherapy is not recommended in patients taking fingolimod.LymphomaCases of lymphoma, including both T-cell and B-cell types and CNS lymphoma, have occurred in patients receiving fingolimod. The reporting rate of non-Hodgkin lymphoma with fingolimod is greater than that expected in the general population adjusted by age, gender, and region. Cutaneous T-cell lymphoma (including mycosis fungoides) has also been reported with fingolimod in the postmarketing setting.
- Immune System Effects Following Fingolimod Discontinuation [see Warnings and Precautions ()]
5.13 Immune System Effects
Following Fingolimod DiscontinuationFingolimod remains in the blood and has pharmacodynamic effects, including decreased lymphocyte counts, for up to 2 months following the last dose of fingolimod. Lymphocyte counts generally return to the normal range within 1 to 2 months of stopping therapy
[see Clinical Pharmacology ]. Because of the continuing pharmacodynamic effects of fingolimod, initiating other drugs during this period warrants the same considerations needed for concomitant administration (e.g., risk of additive immunosuppressant effects)[see Drug Interactions ]. - Hypersensitivity Reactions [see Warnings and Precautions ()]
5.14 Hypersensitivity
ReactionsHypersensitivity reactions, including rash, urticaria, and angioedema have been reported with fingolimod in the postmarketing setting. Fingolimod is contraindicated in patients with history of hypersensitivity to fingolimod or any of its excipients
[see Contraindications ].
Fingolimod is a sphingosine 1-phosphate receptor modulator.
Chemically, fingolimod is 2-amino-2-[2-(4-octylphenyl)ethyl]propan-1,3-diol hydrochloride. Its structure is shown below:
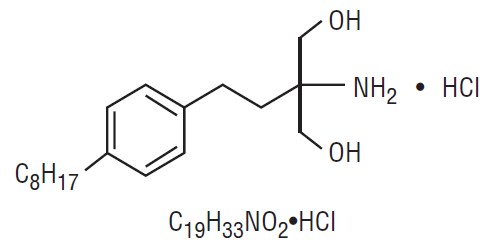
Fingolimod hydrochloride, USP is a white to off-white solid that is freely soluble in water and alcohol and soluble in propylene glycol. It has a molecular weight of 343.93 g/mol.
Fingolimod is provided as 0.5 mg hard gelatin capsules for oral use.
Each 0.5 mg capsule contains 0.56 mg of fingolimod hydrochloride USP, equivalent to 0.5 mg of fingolimod.
Each capsule contains the following inactive ingredients: pregelatinized starch (corn) and sodium lauryl sulfate. The capsule shell contains gelatin, iron oxide yellow, and titanium dioxide. In addition, the imprinting ink contains the following: black iron oxide, potassium hydroxide, propylene glycol, shellac, and strong ammonia solution.