Get your patient on Hydroxocobalamin - Hydroxocobalamin injection, Solution (Hydroxocobalamin)
Hydroxocobalamin - Hydroxocobalamin injection, Solution prescribing information
INDICATIONS AND USAGE
Pernicious anemia, both uncomplicated and accompanied by nervous system involvement.
Dietary deficiency of Vitamin B 12 , occurring in strict vegetarians and in their breast-fed infants. (Isolated vitamin B 12 deficiency is very rare).
Malabsorption of vitamin B 12 , resulting from structural or functional damage to the stomach, where intrinsic factor is secreted or to the ileum, where intrinsic factor facilitates vitamin B 12 absorption. These conditions include tropical sprue, and nontropical sprue (idiopathic steatorrhea, gluten-induced enteropathy). Folate deficiency in these patients is usually more severe than vitamin B 12 deficiency.
Inadequate secretion of intrinsic factor, resulting from lesions that destroy the gastric mucosa (ingestion of corrosives, extensive neoplasia), and a number of conditions associated with a variable degree of gastric atrophy (such as multiple sclerosis, certain endocrine disorders, iron deficiency, and subtotal gastrectomy). Total gastrectomy always produces vitamin B 12 deficiency.
Structural lesions leading to vitamin B 12 deficiency include regional ileitis, ileal resections, malignancies, etc.
Competition for Vitamin B 12 by intestinal parasites or bacteria.
The fish tapeworm (Diphyllobothrium latum) absorbs huge quantities of vitamin B 12 and infested patients often have associated gastric atrophy. The blind-loop syndrome may produce deficiency of Vitamin B 12 or folate.
Inadequate utilization of vitamin B 12 . This may occur if antimetabolites for the vitamin are employed in the treatment of neoplasia.
For the Schilling Test.
DOSAGE AND ADMINISTRATION
Protect from light.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Hydroxocobalamin injection should be given only intramuscularly.
In patients with Addisonian Pernicious Anemia, parenteral therapy with vitamin B 12 is the recommended method of treatment and will be required for the remainder of the patient’s life. Oral therapy is not dependable. In other patients with vitamin B 12 deficiency, the duration of therapy and route of administration will depend upon the cause and whether or not it is reversible.
Confirmatory diagnostic studies should be performed prior to initiating therapy, if possible, and the patient should be followed with appropriate studies to demonstrate hematologic improvement (Hgb, hematocrit, RBC, reticulocyte count). A diagnostic trial utilizing physiologic doses of vitamin B 12 (1 mcg daily) and observing daily reticulocyte counts after establishing a baseline may also be performed. The observation of reticulocytosis which usually occurs between the third and tenth day of therapy confirms the diagnosis of vitamin B 12 deficiency.
In seriously ill patients it may be advisable to administer both vitamin B 12 and folic acid while awaiting the results of distinguishing laboratory studies. It is not necessary to withhold vitamin B 12 therapy until the precise cause of B 12 deficiency is established since absorption studies can be performed at any time.
Serum potassium should be closely observed the first 48 hours and potassium should be administered if necessary.
Treatment of Vitamin B 12 Deficiency
Thirty mcg daily for 5 to 10 days followed by 100 to 200 mcg monthly injected intramuscularly. If the patient is critically ill, or has neurologic disease, an infectious disease or hyperthyroidism, considerably higher doses may be indicated. However, current data indicate that the optimum obtainable neurologic response may be expected with a dosage of vitamin B 12 sufficient to produce good hematologic response. Children may be given a total of 1 to 5 mg over a period of 2 or more weeks in doses of 100 mcg, then 30 to 50 mcg every 4 weeks for maintenance.
Patients who have normal intestinal absorption may be treated with an oral therapeutic multivitamin preparation, containing 15 mcg vitamin B 12 daily.
Schilling Test
The flushing dose is 1000 mcg.
CONTRAINDICATION
Hypersensitivity to any component of this medication.
ADVERSE REACTIONS
Mild transient diarrhea, itching, transitory exanthema, feeling of swelling of entire body, and anaphylaxis.
A few patients may experience pain after injection of hydroxocobalamin.
To report SUSPECTED ADVERSE EVENTS, contact Actavis at 1-800-272-5525 or FDA at 1-800-FDA-1088 or http://www.fda.gov/ for voluntary reporting of adverse reactions.
DESCRIPTION
Hydroxocobalamin injection is a sterile solution of hydroxocobalamin for intramuscular administration.
Each mL contains: Hydroxocobalamin Acetate equivalent to 1000 mcg Hydroxocobalamin, Sodium Acetate Anhydrous 0.2 mg, Glacial Acetic Acid 0.442 mg, Sodium Chloride 8.2 mg, with Methylparaben 1.5 mg and Propylparaben 0.2 mg as preservatives, in Water for Injection q.s. Additional Glacial Acetic Acid and/or Sodium Acetate may have been used to adjust pH. pH range is 3.5 to 5.0.
Hydroxocobalamin appears as dark red orthorhombic needles or as an amorphous or crystalline red powder. It is very hygroscopic in the anhydrous form, and moderately soluble in water. It has a molecular weight of 1346.37. The vitamin B 12 coenzymes are very unstable in light. Hydroxocobalamin shares the cobalamin molecular structure with cyanocobalamin.
The chemical name is α-(5,6-dimethylbenzimidazoly) hydroxocobamide. The empirical formula is C 62 H 89 CoN 13 O 15 P and its structural formula is:
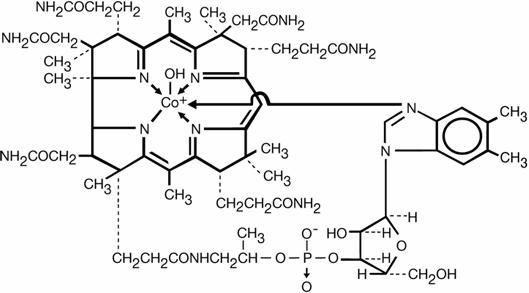
The cobalt content is 4.34%.
CLINICAL PHARMACOLOGY
Vitamin B 12 is essential to growth, cell reproduction, hematopoiesis, nucleoprotein and myelin synthesis.
Fifty percent of the administered dose of hydroxocobalamin disappears from the injection site in 2.5 hours. Hydroxocobalamin is bound to plasma proteins and stored in the liver. It is excreted in the bile and undergoes some enterohepatic recycling. Within 72 hours after injection of 500 to 1000 mcg of hydroxocobalamin, 16 to 66 percent of the injected dose may appear in the urine. The major portion is excreted within the first 24 hours.
HOW SUPPLIED
Hydroxocobalamin Injection USP, 1000 mcg/mL is available in a 30 mL multiple dose vial, individually boxed.
Store at 20°-25°C (68°-77°F). [See USP controlled room temperature.] PROTECT FROM LIGHT.
Literature revised: January 2017
Manufactured by: Hikma Farmaceutica (Portugal) S.A. 2705-906 Terrugem SNT, Portugal Distributed by: Actavis Pharma, Inc. Parsippany, NJ 07054 USA
PIN229-WAT/2