Get your patient on Impoyz - Clobetasol Propionate cream (Clobetasol Propionate)
Impoyz - Clobetasol Propionate cream prescribing information
INDICATIONS AND USAGE
IMPOYZ Cream 0.025% is indicated for the treatment of moderate to severe plaque psoriasis in patients 18 years of age and older.
DOSAGE AND ADMINISTRATION
Apply a thin layer of IMPOYZ Cream to the affected skin areas twice daily and rub in gently and completely. Use IMPOYZ Cream for up to 2 consecutive weeks of treatment. Treatment beyond 2 consecutive weeks is not recommended, and the total dosage should not exceed 50 g per week because of the potential for the drug to suppress the hypothalamic pituitary adrenal (HPA) axis [see Warnings and Precautions (5.1) ].
Discontinue IMPOYZ Cream when control is achieved.
Do not use if atrophy is present at the treatment site.
Do not bandage, cover, or wrap the treated skin area unless directed by a physician.
Avoid use on the face, scalp, axilla, groin, or other intertriginous areas.
IMPOYZ Cream is for topical use only. It is not for oral, ophthalmic, or intravaginal use.
Wash hands after each application.
DOSAGE FORMS AND STRENGTHS
Cream, 0.025% each gram contains 0.25 mg of clobetasol propionate in a white to off-white cream base.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no available data on IMPOYZ Cream in pregnant women to inform a drug-associated risk for adverse development outcomes. Published data report a significantly increased risk of low birthweight with the use of greater than 300 grams of potent or very potent topical corticosteroids during a pregnancy. Advise pregnant women of the potential risk to a fetus and to use IMPOYZ Cream on the smallest area of skin and for the shortest duration possible (see Data ). In animal reproduction studies, increased malformations, such as cleft palate and skeletal abnormalities, were observed after subcutaneous administration of clobetasol propionate to pregnant mice and rabbits. No comparisons of animal exposure with human exposure are provided due to minimal systemic exposure noted after topical administration of IMPOYZ Cream [see Clinical Pharmacology (12.3) ].
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk or birth defect loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Human Data
Multiple observational studies found no significant associations between maternal use of topical corticosteroids of any potency and congenital malformations, preterm delivery, or fetal mortality. However, when the dispensed amount of potent or very potent topical corticosteroid exceeded 300 g during the entire pregnancy, use was associated with an increase in low birth weight infants [adjusted RR, 7.74 (95% CI, 1.49-40.11)]. In addition, a small cohort study, in which 28 sub-Saharan women using potent topical corticosteroids (27/28 used clobetasol propionate 0.05%) for skin lightening during pregnancy, noted a higher incidence of low birth weight infants in the exposed group. The majority of exposed subjects treated large areas of the body [a mean quantity of 60 g/month (range, 12-170g)] over long periods of time.
Animal Data
In an embryofetal development study in mice, subcutaneous administration of clobetasol propionate resulted in fetotoxicity at the highest dose tested ( 1mg/kg) and malformations at the lowest dose tested (0.03 mg/kg). Malformations seen included cleft palate and skeletal abnormalities. In an embryofetal development study in rabbits, subcutaneous administration of clobetasol propionate resulted in malformations at doses of 0.003 and 0.01 mg/kg. Malformations seen included cleft palate, cranioschisis, and other skeletal abnormalities.
Lactation
Risk Summary
There is no information regarding the presence of clobetasol propionate in breast milk or its effects on the breastfed infant or on milk production. Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of clobetasol propionate could result in sufficient systemic absorption to produce detectable quantities in human milk. The developmental and health benefits of breastfeeding should be considered along with the other’s clinical need for IMPOYZ Cream and any potential adverse effects on the breastfed infant from IMPOYZ Cream or from the underlying maternal condition.
Clinical Considerations
To minimize potential exposure to the breastfed infant via breast milk, use IMPOYZ Cream on the smallest area of skin and for the shortest duration possible while breastfeeding. Advise breastfeeding women not to apply IMPOYZ Cream directly to the nipple and areola to avoid direct infant exposure.
Pediatric Use
The safety and effectiveness of IMPOYZ Cream in patients younger than 18 years of age have not been established; therefore, use in children younger than 18 years is not recommended. Because of a higher ratio of skin surface area to body mass, pediatric patients are at a greater risk than adults of systemic toxicity, including HPA axis suppression when treated with topical drugs [see Warnings and Precautions (5.1) ].
Rare systemic toxicities such as Cushing’s syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in pediatric patients, especially those with prolonged exposure to large doses of high potency topical corticosteroids.
Local adverse reactions including striae and skin atrophy have also been reported with use of topical corticosteroids in pediatric patients.
Avoid use of IMPOYZ Cream in the treatment of diaper dermatitis.
Geriatric Use
Clinical studies of IMPOYZ Cream did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience with topical corticosteroids has not identified differences in responses between the elderly and younger patients.
CONTRAINDICATIONS
None.
WARNINGS AND PRECAUTIONS
- Clobetasol propionate has been shown to suppress the HPA axis at the dose tested. (5.1 )
- Cushing’s syndrome, hyperglycemia, and glucosuria can also result from systemic absorption of topical corticosteroids. (5.1 )
- Systemic absorption may require periodic evaluation for HPA axis suppression. Modify use if HPA axis develops. (5.1 )
- Children may be more susceptible to systemic toxicity from use of topical corticosteroids. (5.1 , 8.4 )
- Local adverse reactions with topical corticosteroids may occur more frequently with the use of occlusive dressings, prolonged use, or use of higher potency corticosteroids, including clobetasol propionate. These reactions include; irritation, dryness, acneiform eruptions, hypertrichosis, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, striae and miliaria. (5.1 , 6.2 )
Effects on the Endocrine System
IMPOYZ Cream can cause reversible hypothalamic-pituitary adrenal (HPA) axis suppression with the potential for glucocorticosteroid insufficiency. This may occur during treatment or after withdrawal of treatment. Because of the potential of systemic absorption, use of topical corticosteroids, including IMPOYZ Cream, may require that patients be evaluated periodically for evidence of HPA axis suppression. Factors that predispose a patient to HPA axis suppression include the use of high-potency steroids, large treatment surface areas, prolonged use, use of occlusive dressings, altered skin barrier, liver failure, and young age.
Evaluation for HPA axis suppression may be done by using the adrenocorticotropic hormone (ACTH) stimulation test. In a trial evaluating the effects of IMPOYZ Cream on the HPA axis, subjects with plaque psoriasis applied IMPOYZ Cream twice daily to at least 20% of involved Body Surface Area (BSA) for 15 days. Abnormal ACTH stimulation tests suggestive of HPA axis suppression were seen in 3 of 24 (12.5%) subjects on IMPOYZ Cream [see Clinical Pharmacology (12.2) ]. In another trial to evaluate the effects of IMPOYZ Cream on the HPA axis, subjects with moderate to severe plaque psoriasis applied IMPOYZ Cream twice daily to at least 25% of involved BSA for 28 consecutive days. Abnormal ACTH stimulation test suggestive of HPA axis suppression was seen in 8 of 26 (30.8%) of subjects on IMPOYZ Cream.
If HPA axis suppression is documented, gradually withdraw the drug, reduce the frequency of application, or substitute with a less potent corticosteroid. If signs and symptoms of steroid withdrawal occur, supplemental systemic corticosteroids may be required. Recovery of HPA axis function is generally prompt and complete upon discontinuation of topical corticosteroids.
Systemic effects of topical corticosteroids may also manifest as Cushing’s syndrome, hyperglycemia, and glucosuria. These complications are rare and generally occur after prolonged exposure to larger than recommended doses, particularly with high-potency topical corticosteroids.
Use of more than one corticosteroid-containing product at the same time may increase the total systemic exposure to topical corticosteroids.
Minimize the unwanted risks from endocrine effects by mitigating risk factors favoring increased systemic bioavailability and by using the product as recommended [see Dosage and Administration (2) ].
Pediatric patients may be more susceptible to systemic toxicity because of their larger skin surface to body mass ratios [see Use in Specific Populations (8.4) ].
Local Adverse Reactions with Topical Corticosteroids
Local adverse reactions from topical corticosteroids may include atrophy, striae, telangiectasias, burning, itching, irritation, dryness, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, and miliaria. These may be more likely to occur with occlusive use, prolonged use, or use of higher potency corticosteroids, including IMPOYZ Cream. Some local adverse reactions by be irreversible.
Concomitant Skin Infections
Use an appropriate antimicrobial agent if a skin infection is present or develops. If a favorable response does not occur promptly, discontinue use of IMPOYZ Cream until the infection has been adequately treated
Allergic Contact Dermatitis
Allergic contact dermatitis with corticosteroids is usually diagnosed by observing failure to heal rather than noting a clinical exacerbation. Such an observation should be corroborated with appropriate diagnostic patch testing. If irritation develops, discontinue the topical corticosteroid and institute appropriate therapy.
ADVERSE REACTIONS
The most common adverse reaction (incidence ≥ 1%) is application site discoloration. (6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Primus Pharmaceuticals Inc. at 480-483-1410 or FDA at 1-800-FDA-1088 or www. FDA.gov/medwatch.
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug, and may not reflect the rates observed in practice.
IMPOYZ Cream was evaluated in two randomized, multicenter, prospective, vehicle-controlled clinical trials in subjects with moderate to severe plaque psoriasis. Subjects applied IMPOYZ Cream or vehicle cream twice daily for 14 days. A total of 354 subjects applied IMPOYZ Cream and 178 subjects applied vehicle.
The adverse reaction that occurred in at least 1% of subjects treated with IMPOYZ Cream and at a higher incidence than in subjects treated with vehicle cream was application site discoloration (2% versus 1%).
Less common local adverse events occurring in < 1% of subjects treated with IMPOYZ Cream were application site atrophy, telangiectasia and rash.
Postmarketing Experience
The following adverse reactions have been identified during post-approval use of clobetasol propionate: striae, irritation, dryness, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, hypertrichosis and miliaria. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
DESCRIPTION
IMPOYZ (clobetasol propionate) Cream, 0.025% for topical use contains clobetasol propionate, a synthetic and fluorinated corticosteroid. Chemically, clobetasol propionate is 21-chloro-9-fluoro-11β-hydroxy-16 β-methyl-3,20-dioxopregna-1,4-dien-17-yl propanoate, and it has the following structural formula.
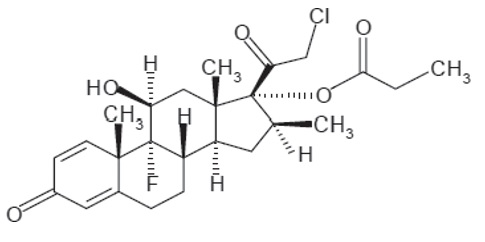
Clobetasol propionate has a molecular formula of C 25 H 32 CIFO 5 and a molecular weight of 467. It is a white to cream-colored crystalline powder practically insoluble in water.
Each gram of IMPOYZ Cream contains 0.25 mg clobetasol propionate. It is an oil-in-water emulsion intended for topical application and contains the following inactive ingredients: butylated hydroxytoluene, cetostearyl alcohol, cyclomethicone, diethylene glycol monoethyl ether, glyceryl stearate and PEG 100 stearate, isopropyl myristate, methyl paraben, propyl paraben. purified water and white wax.
CLINICAL PHARMACOLOGY
Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action in corticosteroid responsive dermatoses is unknown. The contribution to efficacy by individual components of the vehicle has not been established.
Pharmacodynamics
Vasoconstrictor Assay
IMPOYZ Cream, 0.025% is in the high range of potency as demonstrated in vasoconstrictor studies in healthy subjects when compared with other topical corticosteroids. However, similar blanching scores do not necessarily imply therapeutic equivalence.
Hypothalamic-Pituitary-Adrenal (HPA) Axis Suppression:
HPA axis suppression was evaluated in a clinical trial in adult subjects (N=24) with moderate to severe plaque psoriasis involving a mean BSA of 26.5 +8.6%. Treatment consisted of twice daily application of IMPOYZ Cream, 0.025% for 15 days. Adrenal suppression, as indicated by a 30-minute post-stimulation cortisol level ≤18 mcg/dL, was observed in 3 out of 24 subjects (12.5%) after 15 days.
Pharmacokinetics
Topical corticosteroids can be absorbed from intact healthy skin. The extent of percutaneous absorption of topical corticosteroids is determined by many factors, including the product formulation and the integrity of the epidermal barrier. Occlusion, inflammation, and/or other disease processes in the skin may also increase percutaneous absorption. Once absorbed through the skin, topical corticosteroids are metabolized, primarily in the liver, and are then excreted by the kidneys. Some corticosteroids and their metabolites are also excreted in the bile.
In a pharmacokinetic study in 24 adult male and female subjects with moderate to severe psoriasis were treated twice daily for 15 days with a mean dose of approximately 3.7 g of IMPOYZ Cream, 0.025% per application to a mean BSA of 26.5 ± 8.6%. On day 15, the mean + SD pre-treatment and post-treatment systemic concentrations of clobetasol propionate were 50.7 ± 96.0 pg/mL and 56.3 ± 104.7 pg/mL, respectively.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long term animal studies have not been performed to evaluate the carcinogenic potential of clobetasol propionate cream.
In a 13-week repeat dose toxicity study in rats, topical administration of clobetasol propionate cream, 0.001, 0.005 and 0.025% at corresponding doses of 0.004, 0.02 and 0.1 mg/kg/day resulted in corticosteroid class-related systemic effects such as reductions in body weight gain, reductions in total leukocytes and individual white cells, decrease in weight of adrenals, thymus, spleen, liver and lung. Histologically, there were decreased hematopoiesis in the bone marrow, thymic atrophy and mast cell infiltration of the mesenteric lymph nodes. All these effects were indicative of severe immune suppression consistent with long-term exposure to corticosteroids. A no observable adverse effect level (NOAEL) was determined to be clobetasol propionate cream, 0.001% (0.004 mg/kg/day) in male rats while a NOAEL could not be determined in females. The clinical relevance of the findings in animals to humans is not clear, but sustained glucocorticoid-related immune suppression may increase the risk of infection and possibly the risk of carcinogenesis.
Clobetasol propionate was not mutagenic in three different test systems: the Ames test, the Saccharomyces cerevisiae gene conversion assay , and the E. coli B WP2 fluctuation test.
Fertility studies conducted in the rat following subcutaneous administration of clobetasol propionate at dosage levels up to 0.05 mg/kg/day revealed that females exhibited an increase in the number of resorbed embryos and a decrease in the number of living fetuses at the highest dose.
CLINICAL STUDIES
Two double-blind, randomized, vehicle-controlled trials evaluated 532 subjects aged 18 years and older with moderate to severe plaque psoriasis (IGA 3 or 4 and BSA > 3%). Subjects were treated twice daily with IMPOYZ Cream or vehicle cream for 14 days. The primary endpoint was the proportion of subjects who achieved treatment success at Day 15, where treatment success was defined as an IGA score of 0 (clear) or 1 (almost clear) with at least a 2-grade reduction from baseline. The proportion of subjects who achieved treatment success was also assessed at Day 8
Table 1 presents the efficacy results at Day 8 and Day 15
Table 1. Treatment Success • Results
| • Treatment success is defined as an IGA score of 0 (clear) or 1 (almost clear) with at least a 2-grade reduction from baseline. | ||||
| Trial 1 | Trial 2 | |||
| IMPOYZ (N=178) | Vehicle (N=89) | IMPOYZ (N=176) | Vehicle (N=89) | |
| Day 15 (primary endpoint) | 30.2% | 9.0% | 30.1% | 9.7% |
| Day 8 (secondary endpoint) | 15.7% | 5.6% | 14.2% | 1.6% |
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
IMPOYZ Cream, 0.025% is a white off-white cream, supplied as follows:
100 g aluminum tube NDC 68040-713-38
Storage
Store at 20°C-25°C (68°F-77°F), excursions permitted to 15°C-30°C (59°F-86°F) [see USP Controlled Room Temperature]. Do not freeze.
PATIENT INFORMATION IMPOYZ® (Im-poise) (clobetasol propionate) Cream, 0.025%
Important: IMPOYZ Cream is for use on the skin only. Do not get IMPOYZ Cream near or in your eyes, mouth, or vagina.
What is IMPOYZ Cream?
IMPOYZ Cream is a prescription corticosteroid medicine used to treat moderate to severe plaque psoriasis in people 18 year of age and older.
It is not known if IMPOYZ Cream is safe and effective in children under 18 years of age. IMPOYZ Cream is not recommended for use in children under 18 years of age.
Before using IMPOYZ Cream, tell your doctor about all of your medical conditions , including if you:
- have thinning of the skin (atrophy) at the treatment site.
- have a skin infection. You may need medicine to treat the skin infection before using IMPOYZ Cream.
- have diabetes.
- have adrenal gland problems.
- plan to have surgery.
- liver problems
- are pregnant or plan to become pregnant. It is not known if IMPOYZ Cream will harm your unborn baby. If you use IMPOYZ Cream during pregnancy, use IMPOYZ Cream on the smallest area of skin and for the shortest time needed.
- are breastfeeding or plan to breastfeed. It is not known if IMPOYZ Cream passes into breast milk. Breastfeeding women should use IMPOYZ Cream on the smallest area of skin and for the shortest time needed while breastfeeding. Do not apply IMPOYZ Cream directly to the nipple and areola to avoid contact with your baby.
Tell your doctor about all the medicines you take , including prescription and over-the-counter medicines, vitamins, and herbal supplements. Especially tell your doctor if you take other corticosteroid medicines by mount or use other products on your skin that contain corticosteroids.
Do not use other product containing a corticosteroid medicine with IMPOYZ Cream without talking to your doctor first.
How should I use IMPOYZ Cream?
- Use IMPOYZ Cream exactly as your doctor tells you to use it
- Your doctor should tell you how much IMPOYZ Cream to use and where to apply it.
- Apply a thin layer of IMPOYZ Cream to the affected skin areas 2 times each day and rub in gently and completely.
- Use IMPOYZ Cream for the shortest amount of time needed to treat your plaque psoriasis. Tell your doctor if your skin condition is not getting better after 2 weeks for using IMPOYZ. Do not use IMPOYZ Cream for longer than 2 weeks in a row.
- Do not use IMPOYZ Cream on your face, scalp, underarms (armpits), groin, or areas where your skin may touch or rub together.
- Do not use IMPOYZ Cream if thinning of the skin atrophy is present at the treatment site.
- Do not bandage, cover, or wrap the treated skin area unless your doctor tells you to.
- Wash your hand after you apply IMPOYZ Cream.
- See your doctor regularly to check your symptom and side effects while using IMPOYZ Cream.
What are the possible side effects of IMPOYZ Cream?
IMPOYZ Cream may cause serious side effects, including:
- Symptoms of a disorder where the adrenal gland does not make enough of certain hormones (adrenal insufficiency) during treatment or after stopping treatment with IMPOYZ Cream. Your doctor may do blood tests to check for adrenal gland problems during treatment with IMPOYZ Cream.
- Cushing syndrome , a condition that can happen when your body is exposed to too much of the hormone cortisol. Your doctor may do tests to check for this.
- High blood sugar (hyperglycemia) or diabetes mellitus that has not been diagnosed can happened with treatment. Your doctor may do tests to check for this.
- Skin reactions at the treated skin site. Tell your doctor if you get any skin reactions or skin infections.
- Effects on growth and weight in children.
The most common side effect of IMPOYZ Cream includes discoloration of the treated site. This is not the only possible side effect of IMPOYZ Cream.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store IMPOYZ Cream?
- Store IMPOYZ Cream between 68°F to 77°F (20°C to 25°C).
- Do not freeze.
- Throw away (discard) any unused IMPOYZ Cream after 2 weeks.
Keep IMPOYZ Cream and all medicines out of the reach of children.
General information about the safe and effective use of IMPOYZ Cream.
Medicines are sometimes prescribed for purposes other than those listed in the Patient Information leaflet. Do not use IMPOYZ Cream for a condition for which it was not prescribed. Do not give IMPOYZ Cream to other people even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or doctor for information about IMPOYZ Cream that is written for health professionals.
What are the ingredients in IMPOYZ Cream?
Active ingredients: clobetasol propionate
Inactive ingredients: butylated hydroxytoluene, cetostearyl alcohol, cyclomethicone, diethylene glycol monoethyl ether, glyceryl stearate and PEG 100 stearate, isopropyl myristate, methyl paraben, propyl paraben, purified water and white wax.
Manufactured by DPT Laboratories Ltd. San Antonio, TX 78215
For Primus Pharmaceuticals, Inc. Scottsdale AZ 85253 Revised 04/2021
This patient information has been approved by the U.S. Food and Drug Administration Issued 11/2017
Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action in corticosteroid responsive dermatoses is unknown. The contribution to efficacy by individual components of the vehicle has not been established.