Get your patient on Levonorgestrel And Ethinyl Estradiol - Levonorgestrel And Ethinyl Estradiol (Levonorgestrel And Ethinyl Estradiol)
Levonorgestrel And Ethinyl Estradiol - Levonorgestrel And Ethinyl Estradiol prescribing information
WARNING: CIGARETTE SMOKING AND SERIOUS CARDIOVASCULAR EVENTS
Cigarette smoking increases the risk of serious cardiovascular events from combination oral contraceptive (COC) use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked. For this reason, COCs, including levonorgestrel and ethinyl estradiol tablets, are contraindicated in women who are over 35 years of age and smoke [see CONTRAINDICATIONS and WARNINGS (1) ].
INDICATIONS AND USAGE
Levonorgestrel and ethinyl estradiol tablets, 0.15 mg/30 mcg are indicated for use by females of reproductive potential to prevent pregnancy.
DOSAGE AND ADMINISTRATION
How to Start and Take Levonorgestrel and Ethinyl Estradiol Tablets
Levonorgestrel and ethinyl estradiol tablets, 0.15 mg/30 mcg are dispensed in a compact dispenser containing 28 tablets (see HOW SUPPLIED ). Levonorgestrel and ethinyl estradiol tablets may be started using either a Day 1 start or a Sunday start (see Table 3 ). For the first cycle of a Sunday start regimen, an additional method of contraception should be used until after the first 7 consecutive days of administration.
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
Starting Levonorgestrel and Ethinyl Estradiol Tablets after Abortion or Miscarriage
First-trimester
- After a first-trimester abortion or miscarriage, levonorgestrel and ethinyl estradiol tablets may be started immediately. An additional method of contraception is not needed if levonorgestrel and ethinyl estradiol tablets are started immediately.
- If levonorgestrel and ethinyl estradiol tablets are not started within 5 days after termination of the pregnancy, the patient should use additional non-hormonal contraception (such as condoms or spermicide) for the first seven days of her first cycle of levonorgestrel and ethinyl estradiol tablets.
Second-trimester
- Do not start until 4 weeks after a second-trimester abortion or miscarriage, due to the increased risk of thromboembolic disease. Start levonorgestrel and ethinyl estradiol tablets following the instructions in Table 3 for Day 1 or Sunday start. Use additional non-hormonal contraception (such as condoms or spermicide) for the first seven days of the patient’s first cycle of levonorgestrel and ethinyl estradiol tablets (see CONTRAINDICATIONS , WARNINGS (1) , PRECAUTIONS (10) and FDA-APPROVED PATIENT LABELING ).
Starting Levonorgestrel and Ethinyl Estradiol Tablets after Childbirth
- Do not start until 4 weeks after delivery, due to the increased risk of thromboembolic disease. Start contraceptive therapy with levonorgestrel and ethinyl estradiol tablets following the instructions in Table 3 for women not currently using hormonal contraception.
- Levonorgestrel and ethinyl estradiol tablets are not recommended for use in lactating women (see PRECAUTIONS (7) and FDA-APPROVED PATIENT LABELING ).
- If the woman has not yet had a period postpartum, consider the possibility of ovulation and conception occurring prior to use of levonorgestrel and ethinyl estradiol tablets (see CONTRAINDICATIONS , WARNINGS (9) , PRECAUTIONS (6) and FDA- APPROVED PATIENT LABELING ).
Dosing Levonorgestrel and Ethinyl Estradiol Tablets
Instruct patients to take one tablet by mouth at the same time every day. To achieve maximum contraceptive effectiveness, patients must take levonorgestrel and ethinyl estradiol tablets as directed, in the order directed on the blister pack. The failure rate may increase when pills are missed or taken incorrectly.
Missed doses
Instruct patients about the handling of missed doses (e.g., to take single missed pills as soon as possible) and to follow the dosing instructions provided in the FDA-approved patient labeling.
| Take the tablet as soon as possible. Continue taking one tablet a day until the pack is finished. |
| Take the two missed tablets as soon as possible and the next two active tablets the next day. Continue taking one tablet a day until the pack is finished. Additional nonhormonal contraception (such as condoms or spermicide) should be used as back-up if the patient has sex within 7 days after missing tablets. |
| Day 1 start: Throw out the rest of the pack and start a new pack that same day. Sunday start: Continue taking one tablet a day until Sunday, then throw out the rest of the pack and start a new pack that same day. Additional nonhormonal contraception (such as condoms or spermicide) should be used as back-up if the patient has sex within 7 days after missing tablets. |
Advice in Case of Gastrointestinal Disturbances
If vomiting occurs within 3 to 4 hours after taking levonorgestrel and ethinyl estradiol tablets, the patient should proceed as if she missed a tablet. In case of prolonged vomiting or diarrhea, absorption may not be complete and additional contraceptive measures should be taken.
CONTRAINDICATIONS
Levonorgestrel and ethinyl estradiol tablets are contraindicated in females who are known to have the following conditions:
- A high risk of arterial or venous thrombotic diseases. Examples include women who are known to:
- Smoke, if over age 35 [see BOXED WARNING and WARNINGS (1) ].
- Have current or history of deep vein thrombosis or pulmonary embolism [see WARNINGS (1) ].
- Have cerebrovascular disease [see WARNINGS (1) ].
- Have coronary artery disease [see WARNINGS (1) ].
- Have thrombogenic valvular or thrombogenic rhythm diseases of the heart (for example, subacute bacterial endocarditis with valvular disease, or atrial fibrillation) [see WARNINGS (1) ].
- Have inherited or acquired hypercoagulopathies [see WARNINGS (1) ].
- Have uncontrolled hypertension or hypertension with vascular disease [see WARNINGS (3) ].
- Have diabetes mellitus and are over age 35, diabetes mellitus with hypertension or vascular disease or other end-organ damage, or diabetes mellitus of >20 years duration [see WARNINGS (7) ].
- Have headaches with focal neurological symptoms, migraine headaches with aura, or over age 35 with any migraine headaches [see WARNINGS (8) ].
- Current diagnosis of, or history of, breast cancer, which may be hormone-sensitive.
- Liver tumors, acute viral hepatitis, or severe (decompensated) cirrhosis [see WARNINGS (2) ].
- Use of Hepatitis C drug combinations containing ombitasvir/paritaprevir/ritonavir, with or without dasabuvir, due to the potential for ALT elevations [see WARNINGS (5) ].
- Undiagnosed abnormal uterine bleeding [see WARNINGS (9) ].
ADVERSE REACTIONS
The following serious adverse reactions with the use of COCs are discussed elsewhere in the labeling:
- Serious cardiovascular adverse events [see BOXED WARNING and WARNINGS (1) ]
- Vascular events [see WARNINGS (1) ]
- Liver disease [see WARNINGS (2) ]
- Hypertension [see WARNINGS (3) ]
- Gallbladder disease [see WARNINGS (6) ]
- Carbohydrate and lipid effects [see WARNINGS (7) ]
- Headache [see WARNINGS (8) ]
- Carcinoma of the cervix [see WARNINGS (11) ]
Adverse reactions reported by COC users and described elsewhere in the labeling are:
- Bleeding irregularities and amenorrhea [see WARNINGS (9) ]
- Mood changes, including depression [see WARNINGS (10) ]
- Melasma/chloasma which may persist [see WARNINGS (14) ]
- Edema/fluid retention [see PRECAUTIONS (2) ]
- Diminution in lactation when given immediately postpartum [see PRECAUTIONS (7) ]
Post Marketing Experience
Five studies that compared breast cancer risk between ever-users (current or past use) of COCs and never-users of COCs reported no association between ever use of COCs and breast cancer risk, with effect estimates ranging from 0.90 - 1.12 (Figure 2).
Three studies compared breast cancer risk between current or recent COC users (<6 months since last use) and never users of COCs (Figure 2). One of these studies reported no association between breast cancer risk and COC use. The other two studies found an increased relative risk of 1.19 - 1.33 with current or recent use. Both of these studies found an increased risk of breast cancer with current use of longer duration, with relative risks ranging from 1.03 with less than one year of COC use to approximately 1.4 with more than 8-10 years of COC use.
Figure 2: Relevant Studies of Risk of Breast Cancer with Combined Oral Contraceptives
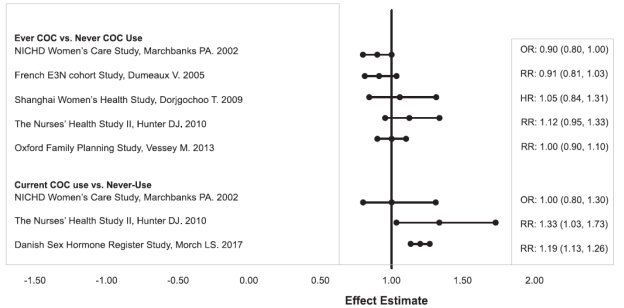
RR = relative risk; OR = odds ratio; HR = hazard ratio. “ever COC” are females with current or past COC use; “never COC use” are females that never used COCs.
The following adverse reactions have been reported in patients receiving oral contraceptives and are believed to be drug-related: Breast tenderness, pain, enlargement, secretion; Nausea, vomiting and gastrointestinal symptoms (such as abdominal pain, cramps and bloating); Change in menstrual flow; Temporary infertility after discontinuation of treatment; Change in weight or appetite (increase or decrease); Change in cervical erosion and secretion; Cholestatic jaundice; Rash (allergic); Vaginitis, including candidiasis; Change in corneal curvature (steepening); Intolerance to contact lenses; Mesenteric thrombosis; Decrease in serum folate levels; Exacerbation of systemic lupus erythematosus; Exacerbation of porphyria; Exacerbation of chorea; Aggravation of varicose veins; Anaphylactic/anaphylactoid reactions, including urticaria, angioedema, and severe reactions with respiratory and circulatory symptoms.
The following adverse reactions have been reported in users of oral contraceptives, and the association has been neither confirmed nor refuted: Congenital anomalies; Premenstrual syndrome; Cataracts; Optic neuritis, which may lead to partial or complete loss of vision; Cystitis-like syndrome; Nervousness; Dizziness; Hirsutism; Loss of scalp hair; Erythema multiforme; Erythema nodosum; Hemorrhagic eruption; Impaired renal function; Hemolytic uremic syndrome; Budd-Chiari syndrome; Acne; Changes in libido; Colitis; Sickle-cell disease; Cerebral-vascular disease with mitral valve prolapse; Lupus-like syndromes; Pancreatitis; Dysmenorrhea.
DESCRIPTION
Levonorgestrel and ethinyl estradiol tablets USP, 0.15 mg/30 mcg are a combination oral contraceptives (COC) consisting of 21 white to off-white active tablets, each containing 0.15 mg of levonorgestrel, a synthetic progestin and 30 mcg of ethinyl estradiol, an estrogen, and 7 green inert tablets (without hormones).
The structural formulas for the active components are:
Levonorgestrel
C 21 H 28 O 2 MW: 312.45
Levonorgestrel is chemically 18,19-Dinorpregn-4-en-20-yn-3-one, 13-ethyl-17-hydroxy-,(17α)-(-)-.
Ethinyl Estradiol
C 20 H 24 O 2 MW: 296.40
Ethinyl Estradiol is 19-Nor-17α-pregna-1,3,5(10)-trien-20-yne-3, 17-diol.
Each white to off-white active tablet contains the following inactive ingredients: lactose monohydrate, magnesium stearate, and polacrilin potassium.
Each green inert tablet contains the following inactive ingredients: FD&C Blue No. 1 aluminum lake, lactose monohydrate, magnesium stearate, polacrilin potassium, and yellow oxide of iron.
CLINICAL PHARMACOLOGY
Combination oral contraceptives prevent pregnancy primarily by suppressing ovulation.