Get your patient on Milrinone Lactate In Dextrose - Milrinone Lactate injection, Solution (Milrinone Lactate)
Milrinone Lactate In Dextrose - Milrinone Lactate injection, Solution prescribing information
INDICATIONS AND USAGE
Milrinone is indicated for the short-term intravenous treatment of patients with acute decompensated heart failure. Patients receiving milrinone should be observed closely with appropriate electrocardiographic equipment. The facility for immediate treatment of potential cardiac events, which may include life-threatening ventricular arrythmias, must be available. The majority of experience with intravenous milrinone has been in patients receiving digoxin and diuretics. There is no experience in controlled trials with infusions of milrinone for periods exceeding 48 hours.
DOSAGE AND ADMINISTRATION
Milrinone should be administered with a loading dose followed by a continuous infusion (maintenance dose) according to the following guidelines:
Loading Dose
50 mcg/kg: Administer slowly over 10 minutes
Note: Milrinone (200 mcg/mL) in INTRAVIA Plastic Container is for intravenous infusion only.
Dosage recommendations using a 1 mg/mL concentration of milrinone are included for informational purposes only.
The table below shows the loading dose in milliliters (mL) of milrinone (1mg/mL) by patient body weight (kg).
Patient Body Weight (kg) | ||||||||||
kg | 30 | 40 | 50 | 60 | 70 | 80 | 90 | 100 | 110 | 120 |
mL | 1.5 | 2.0 | 2.5 | 3.0 | 3.5 | 4.0 | 4.5 | 5.0 | 5.5 | 6.0 |
The loading dose may be given undiluted, but diluting to a rounded total volume of 10 or 20 mL (see appropriate package insert for diluents) may simplify the visualization of the injection rate.
Maintenance Dose
Infusion Rate | Total Daily Dose (24 Hours) | ||
Minimum | 0.375 mcg/kg/min | 0.59 mg/kg | Administer as a continuous intravenous infusion |
Standard | 0.50 mcg/kg/min | 0.77 mg/kg | |
Maximum | 0.75 mcg/kg/min | 1.13 mg/kg |
The infusion rate should be adjusted according to hemodynamic and clinical response. Patients should be closely monitored. In controlled clinical studies, most patients showed an improvement in hemodynamic status as evidenced by increases in cardiac output and reductions in pulmonary capillary wedge pressure.
Note: See " Dosage Adjustment in Renally Impaired Patients ." Dosage may be titrated to the maximum hemodynamic effect and should not exceed 1.13 mg/kg/day. Duration of therapy should depend upon patient responsiveness.
The maintenance dose in mL/hr by patient body weight (kg) may be determined by reference to the following table.
Maintenance Dose (mcg/kg/min) | Patient Body Weight (kg) | |||||||||
30 | 40 | 50 | 60 | 70 | 80 | 90 | 100 | 110 | 120 | |
0.375 | 3.4 | 4.5 | 5.6 | 6.8 | 7.9 | 9.0 | 10.1 | 11.3 | 12.4 | 13.5 |
0.400 | 3.6 | 4.8 | 6.0 | 7.2 | 8.4 | 9.6 | 10.8 | 12.0 | 13.2 | 14.4 |
0.500 | 4.5 | 6.0 | 7.5 | 9.0 | 10.5 | 12.0 | 13.5 | 15.0 | 16.5 | 18.0 |
0.600 | 5.4 | 7.2 | 9.0 | 10.8 | 12.6 | 14.4 | 16.2 | 18.0 | 19.8 | 21.6 |
0.700 | 6.3 | 8.4 | 10.5 | 12.6 | 14.7 | 16.8 | 18.9 | 21.0 | 23.1 | 25.2 |
0.750 | 6.8 | 9.0 | 11.3 | 13.5 | 15.8 | 18.0 | 20.3 | 22.5 | 24.8 | 27.0 |
Dosage Adjustment in Renally Impaired Patients
Data obtained from patients with severe renal impairment (creatinine clearance = 0 to 30 mL/min) but without congestive heart failure have demonstrated that the presence of renal impairment significantly increases the terminal elimination half-life of milrinone. Reductions in infusion rate may be necessary in patients with renal impairment. For patients with clinical evidence of renal impairment, the recommended infusion rate can be obtained from the following table:
Creatinine Clearance (mL/min/1.73 m 2 ) | Infusion Rate (mcg/kg/min) |
5 | 0.20 |
10 | 0.23 |
20 | 0.28 |
30 | 0.33 |
40 | 0.38 |
50 | 0.43 |
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. Milrinone Lactate in 5% Dextrose Injection is a clear, colorless to pale yellow solution.
CONTRAINDICATIONS
Milrinone is contraindicated in patients who are hypersensitive to it.
Solutions containing dextrose may be contraindicated in patients with known allergy to corn or corn products.
ADVERSE REACTIONS
Cardiovascular Effects
In patients receiving milrinone in Phase II and III clinical trials, ventricular arrhythmias were reported in 12.1%: Ventricular ectopic activity, 8.5%; nonsustained ventricular tachycardia, 2.8%; sustained ventricular tachycardia, 1% and ventricular fibrillation, 0.2% (2 patients experienced more than one type of arrhythmia). Holter recordings demonstrated that in some patients injection of milrinone increased ventricular ectopy, including nonsustained ventricular tachycardia. Life-threatening arrhythmias were infrequent and when present have been associated with certain underlying factors such as preexisting arrhythmias, metabolic abnormalities (e.g. hypokalemia), abnormal digoxin levels and catheter insertion. Milrinone was not shown to be arrhythmogenic in an electrophysiology study. Supraventricular arrhythmias were reported in 3.8% of the patients receiving milrinone. The incidence of both supraventricular and ventricular arrhythmias has not been related to the dose or plasma milrinone concentration.
Other cardiovascular adverse reactions include hypotension, 2.9% and angina/chest pain, 1.2%.
In the post-marketing experience, there have been rare cases of “torsades de pointes” reported.
CNS Effects
Headaches, usually mild to moderate in severity, have been reported in 2.9% of patients receiving milrinone.
Other Effects
Other adverse reactions reported, but not definitely related to the administration of milrinone include hypokalemia, 0.6%; tremor, 0.4%; and thrombocytopenia, 0.4%.
Post-Marketing Adverse Event Reports
In addition to adverse events reported from clinical trials, the following events have been reported from worldwide post-marketing experience with Milrinone:
Isolated spontaneous reports of bronchospasm and anaphylactic shock.
Liver function test abnormalities and skin reactions such as rash.
Administration site conditions: Infusion site reaction.
Drug Interactions
No untoward clinical manifestations have been observed in limited experience with patients in whom milrinone was used concurrently with the following drugs: digitalis glycosides; lidocaine, quinidine; hydralazine, prazosin; isosorbide dinitrate, nitroglycerin; chlorthalidone, furosemide, hydrochlorothiazide, spironolactone; captopril; heparin, warfarin, diazepam, insulin; and potassium supplements.
DESCRIPTION
Milrinone lactate is a member of a new class of bipyridine inotropic/vasodilator agents with phosphodiesterase inhibitor activity, distinct from digitalis glycosides or catecholamines. Milrinone lactate is designated chemically as 1,6-dihydro-2-methyl-6-oxo-[3,4’-bipyridine]-5-carbonitrile lactate and has the following structure:
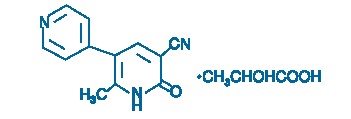
Milrinone is an off-white to tan crystalline compound with a molecular weight of 211.2 and a molecular formula of C 12 H 9 N 3 O. It is slightly soluble in methanol, and very slightly soluble in chloroform and in water. As the lactate salt, it is stable and colorless to pale yellow in solution. Milrinone is available as sterile aqueous solutions of the lactate salt of milrinone for infusion intravenously. The flexible containers provide two ready-to-use dilutions of milrinone in volumes of 100 mL and 200 mL of 5% Dextrose Injection. Each mL contains milrinone lactate equivalent to 200 mcg milrinone. The nominal concentration of lactic acid is 0.282 mg/mL. Each mL also contains 54.3 mg Dextrose Hydrous, USP. The pH is adjusted with lactic acid and/or sodium hydroxide pH 3.5 (3.2 - 4.0). The flexible container is manufactured from a specially designed multilayer plastic (PL 2408). Solutions in contact with the plastic container leach out certain chemical components from the plastic in very small amounts; however, biological testing was supportive of the safety of the plastic container materials. The flexible container has a foil overwrap. Water can permeate the plastic into the overwrap, but the amount is insufficient to significantly affect the premixed solution.
CLINICAL PHARMACOLOGY
Milrinone is a positive inotrope and vasodilator, with little chronotropic activity different in structure and mode of action from either the digitalis glycosides or catecholamines. Milrinone, at relevant inotropic and vasorelaxant concentrations, is a selective inhibitor of peak III cAMP phosphodiesterase isozyme in cardiac and vascular muscle. This inhibitory action is consistent with cAMP mediated increases in intracellular ionized calcium and contractile force in cardiac muscle, as well as with cAMP dependent contractile protein phosphorylation and relaxation in vascular muscle. Additional experimental evidence also indicates that milrinone is not a beta-adrenergic agonist nor does it inhibit sodium-potassium adenosine triphosphatase activity as do the digitalis glycosides.
Clinical studies in patients with congestive heart failure have shown that milrinone produces dose-related and plasma drug concentration-related increases in the maximum rate of increase of left ventricular pressure. Studies in normal subjects have shown that milrinone produces increases in the slope of the left ventricular pressure-dimension relationship, indicating a direct inotropic effect of the drug. Milrinone also produces dose-related and plasma concentration-related increases in forearm blood flow in patients with congestive heart failure, indicating a direct arterial vasodilator activity of the drug.
Both the inotropic and vasodilatory effects have been observed over the therapeutic range of plasma milrinone concentrations of 100 ng/mL to 300 ng/mL.
In addition to increasing myocardial contractility, milrinone improves diastolic function as evidenced by improvements in left ventricular diastolic relaxation.
The acute administration of intravenous milrinone has also been evaluated in clinical trials in excess of 1600 patients, with chronic heart failure, heart failure associated with cardiac surgery, and heart failure associated with myocardial infarction. The total number of deaths, either on therapy or shortly thereafter (24 hours) was 15, less than 0.9%, few of which were thought to be drug-related.
HOW SUPPLIED
Baxter’s Milrinone Lactate in 5% Dextrose Injection is supplied in INTRAVIA Plastic Container as follows:
2J0900 | NDC 0338-6010-48 | 100 mL (200 mcg/mL) |
2J0901 | NDC 0338-6011-37 | 200 mL (200 mcg/mL) |
Exposure of pharmaceutical products to heat should be minimized. Avoid excessive heat. Protect from freezing. It is recommended that the product be stored at room temperature, 25° C (77° F); however, brief exposure up to 40° C (104° F) does not adversely affect the product.