Get your patient on Nimodipine - Nimodipine capsule, Liquid Filled (Nimodipine)
Nimodipine - Nimodipine capsule, Liquid Filled prescribing information
DO NOT ADMINISTER NIMODIPINE INTRAVENOUSLY OR BY OTHER PARENTERAL ROUTES. DEATHS AND SERIOUS, LIFE THREATENING ADVERSE EVENTS HAVE OCCURRED WHEN THE CONTENTS OF NIMODIPINE CAPSULES HAVE BEEN INJECTED PARENTERALLY (See WARNINGS and DOSAGE AND ADMINISTRATION ).
INDICATIONS AND USAGE
Nimodipine is indicated for the improvement of neurological outcome by reducing the incidence and severity of ischemic deficits in patients with subarachnoid hemorrhage from ruptured intracranial berry aneurysms regardless of their post-ictus neurological condition (i.e., Hunt and Hess Grades I to V).
DOSAGE AND ADMINISTRATION
DO NOT ADMINISTER NIMODIPINE CAPSULES INTRAVENOUSLY OR BY OTHER PARENTERAL ROUTES (see WARNINGS ). If nimodipine is inadvertently administered intravenously, clinically significant hypotension may require cardiovascular support with pressor agents. Specific treatments for calcium channel blocker overdose should also be given promptly.
Nimodipine is given orally in the form of soft gelatin 30 mg capsules for subarachnoid hemorrhage.
The recommended oral dose is 60 mg (two 30 mg capsules) every 4 hours for 21 consecutive days. In general, the capsules should be swallowed whole with a little liquid, preferably not less than one hour before or two hours after meals. Grapefruit juice is to be avoided (see PRECAUTIONS, Drug Interactions ). Oral nimodipine therapy should commence as soon as possible within 96 hours of the onset of subarachnoid hemorrhage.
If the capsule cannot be swallowed, e.g., at the time of surgery, or if the patient is unconscious, a hole should be made in both ends of the capsule with an 18 gauge needle, and the contents of the capsule extracted into a syringe. A parenteral syringe can be used to extract the liquid inside the capsule, but the liquid should always be transferred to a syringe that cannot accept a needle and that is designed for administration orally or via a naso-gastric tube or PEG. To help minimize administration errors, it is recommended that the syringe used for administration be labeled "Not for IV Use". The contents should then be emptied into the patient's in situ naso-gastric tube and washed down the tube with 30 mL of normal saline (0.9%).
Severely disturbed liver function, particularly liver cirrhosis, may result in an increased bioavailability of nimodipine due to a decreased first pass capacity and a reduced metabolic clearance. The reduction in blood pressure and other adverse effects may be more pronounced in these patients. Dosage should be reduced to one 30 mg capsule every 4 hours with close monitoring of blood pressure and heart rate; if necessary, discontinuation of the treatment should be considered.
Strong inhibitors of CYP3A4 should not be administered concomitantly with nimodipine (see CONTRAINDICATIONS ). Strong inducers of CYP3A4 should generally not be administered with nimodipine (see WARNINGS ). Patients on moderate and weak inducers of CYP3A4 should be closely monitored for lack of effectiveness, and a nimodipine dose increase may be required. Patients on moderate and weak CYP3A4 inhibitors may require a nimodipine dose reduction in case of hypotension (see PRECAUTIONS, Drug Interactions ).
CONTRAINDICATIONS
The concomitant use of nimodipine with strong inhibitors of CYP3A4 such as some macrolide antibiotics (e.g., clarithromycin, telithromycin), some anti-HIV protease inhibitors (e.g., delaviridine, indinavir, nelfinavir, ritonavir, saquinavir), some azole antimycotics (e.g., ketoconazole, itraconazole, voriconazole) and some antidepressants (e.g., nefazadone) is contraindicated because of a risk of significant hypotension (see PRECAUTIONS, Drug Interactions ).
ADVERSE REACTIONS
Adverse experiences were reported by 92 of 823 patients with subarachnoid hemorrhage (11.2%) who were given nimodipine. The most frequently reported adverse experience was decreased blood pressure in 4.4% of these patients. Twenty-nine of 479 (6.1%) placebo treated patients also reported adverse experiences. The events reported with a frequency greater than 1% are displayed below by dose.
| Sign/Symptom | 0.35 mg/kg (n=82) | 30 mg (n=71) | 60 mg (n=494) | 90 mg (n=172) | 120 mg (n=4) | Placebo (n=479) |
| Decreased | ||||||
| Blood Pressure | 1 (1.2) | 0 | 19 (3.8) | 14 (8.1) | 2 (50.0) | 6 (1.2) |
| Abnormal Liver | ||||||
| Function Test | 1 (1.2) | 0 | 2 (0.4) | 1 (0.6) | 0 | 7 (1.5) |
| Edema | 0 | 0 | 2 (0.4) | 2 (1.2) | 0 | 3 (0.6) |
| Diarrhea | 0 | 3 (4.2) | 0 | 3 (1.7) | 0 | 3 (0.6) |
| Rash | 2 (2.4) | 0 | 3 (0.6) | 2 (1.2) | 0 | 3 (0.6) |
| Headache | 0 | 1 (1.4) | 6 (1.2) | 0 | 0 | 1 (0.2) |
| Gastrointestinal | ||||||
| Symptoms | 2 (2.4) | 0 | 0 | 2 (1.2) | 0 | 0 |
| Nausea | 1 (1.2) | 1 (1.4) | 6 (1.2) | 1 (0.6) | 0 | 0 |
| Dyspnea | 1 (1.2) | 0 | 0 | 0 | 0 | 0 |
| EKG Abnormalities | 0 | 1 (1.4) | 0 | 1 (0.6) | 0 | 0 |
| Tachycardia | 0 | 1 (1.4) | 0 | 0 | 0 | 0 |
| Bradycardia | 0 | 0 | 5 (1.0) | 1 (0.6) | 0 | 0 |
| Muscle Pain/Cramp | 0 | 1 (1.4) | 1 (0.2) | 1 (0.6) | 0 | 0 |
| Acne | 0 | 1 (1.4) | 0 | 0 | 0 | 0 |
| Depression | 0 | 1 (1.4) | 0 | 0 | 0 | 0 |
There were no other adverse experiences reported by the patients who were given 0.35 mg/kg q4h, 30 mg q4h or 120 mg q4h. Adverse experiences with an incidence rate of less than 1% in the 60 mg q4h dose group were: hepatitis; itching; gastrointestinal hemorrhage; thrombocytopenia; anemia; palpitations; vomiting; flushing; diaphoresis; wheezing; phenytoin toxicity; lightheadedness; dizziness; rebound vasospasm; jaundice; hypertension; hematoma.
Adverse experiences with an incidence rate less than 1% in the 90 mg q4h dose group were: itching, gastrointestinal hemorrhage; thrombocytopenia; neurological deterioration; vomiting; diaphoresis; congestive heart failure; hyponatremia; decreasing platelet count; disseminated intravascular coagulation; deep vein thrombosis.
As can be seen from the table, side effects that appear related to nimodipine use based on increased incidence with higher dose or a higher rate compared to placebo control, included decreased blood pressure, edema and headaches which are known pharmacologic actions of calcium channel blockers. It must be noted, however, that SAH is frequently accompanied by alterations in consciousness which lead to an under reporting of adverse experiences. Patients who received nimodipine in clinical trials for other indications reported flushing (2.1%), headache (4.1%) and fluid retention (0.3%), typical responses to calcium channel blockers. As a calcium channel blocker, nimodipine may have the potential to exacerbate heart failure in susceptible patients or to interfere with A-V conduction, but these events were not observed.
No clinically significant effects on hematologic factors, renal or hepatic function or carbohydrate metabolism have been causally associated with oral nimodipine. Isolated cases of non-fasting elevated serum glucose levels (0.8%), elevated LDH levels (0.4%), decreased platelet counts (0.3%), elevated alkaline phosphatase levels (0.2%) and elevated SGPT levels (0.2%) have been reported rarely.
To report SUSPECTED ADVERSE REACTIONS, contact Avet Pharmaceuticals Inc. at 1-866-901-DRUG (3784) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DESCRIPTION
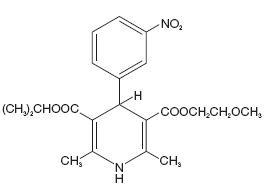
Nimodipine belongs to the class of pharmacological agents known as calcium channel blockers. Nimodipine is isopropyl 2-methoxyethyl 1,4-dihydro-2,6-dimethyl-4-( m -nitrophenyl)-3,5-pyridinedicarboxylate. It has a molecular weight of 418.5 and a molecular formula of C 21 H 26 N 2 O 7 . The structural formula is:
Nimodipine is a yellow crystalline substance, practically insoluble in water.
Nimodipine capsules are formulated as soft gelatin capsules for oral administration. Each liquid filled capsule contains 30 mg of nimodipine in a vehicle of glycerin, peppermint oil and polyethylene glycol. The gelatin shell contains FD&C Yellow No. 6 Aluminum Lake, gelatin, glycerin, iron oxide black, lecithin, medium-chain triglycerides, shellac, sorbitol and titanium dioxide.
CLINICAL PHARMACOLOGY
Mechanism of Action
Nimodipine is a calcium channel blocker. The contractile processes of smooth muscle cells are dependent upon calcium ions, which enter these cells during depolarization as slow ionic transmembrane currents. Nimodipine inhibits calcium ion transfer into these cells and thus inhibits contractions of vascular smooth muscle. In animal experiments, nimodipine had a greater effect on cerebral arteries than on arteries elsewhere in the body perhaps because it is highly lipophilic, allowing it to cross the blood-brain barrier; concentrations of nimodipine as high as 12.5 ng/mL have been detected in the cerebrospinal fluid of nimodipine-treated subarachnoid hemorrhage (SAH) patients.
The precise mechanism of action of nimodipine in humans is unknown. Although the clinical studies described below demonstrate a favorable effect of nimodipine on the severity of neurological deficits caused by cerebral vasospasm following SAH, there is no arteriographic evidence that the drug either prevents or relieves the spasm of these arteries. However, whether or not the arteriographic methodology utilized was adequate to detect a clinically meaningful effect, if any, on vasospasm is unknown.
Pharmacokinetics and Metabolism
In man, nimodipine is rapidly absorbed after oral administration, and peak concentrations are generally attained within one hour. The terminal elimination half-life is approximately 8 to 9 hours but earlier elimination rates are much more rapid, equivalent to a half-life of 1 to 2 hours; a consequence is the need for frequent (every 4 hours) dosing. There were no signs of accumulation when nimodipine was given three times a day for seven days. Nimodipine is over 95% bound to plasma proteins. The binding was concentration independent over the range of 10 ng/mL to 10 mcg/mL. Nimodipine is eliminated almost exclusively in the form of metabolites and less than 1% is recovered in the urine as unchanged drug. Numerous metabolites, all of which are either inactive or considerably less active than the parent compound, have been identified. The metabolism of nimodipine is mediated by CYP3A4. Because of a high first-pass metabolism, the bioavailability of nimodipine averages 13% after oral administration. The bioavailability is significantly increased in patients with hepatic cirrhosis, with C max approximately double that in normals which necessitates lowering the dose in this group of patients (see DOSAGE AND ADMINISTRATION ). In a study of 24 healthy male volunteers, administration of nimodipine capsules following a standard breakfast resulted in a 68% lower peak plasma concentration and 38% lower bioavailability relative to dosing under fasted conditions.
In a single parallel-group study involving 24 elderly subjects (aged 59 to 79) and 24 younger subjects (aged 22 to 40), the observed AUC and C max of nimodipine was approximately 2-fold higher in the elderly population compared to the younger study subjects following oral administration (given as a single dose of 30 mg and dosed to steady-state with 30 mg t.i.d. for 6 days). The clinical response to these age-related pharmacokinetic differences, however, was not considered significant. (See PRECAUTIONS: Geriatric Use. )
Clinical Trials
Nimodipine has been shown, in 4 randomized, double-blind, placebo-controlled trials, to reduce the severity of neurological deficits resulting from vasospasm in patients who have had a recent subarachnoid hemorrhage (SAH). The trials used doses ranging from 20–30 mg to 90 mg every 4 hours, with drug given for 21 days in 3 studies, and for at least 18 days in the other. Three of the four trials followed patients for 3 to 6 months. Three of the trials studied relatively well patients, with all or most patients in Hunt and Hess Grades I to III (essentially free of focal deficits after the initial bleed) the fourth studied much sicker patients, Hunt and Hess Grades III to V. Two studies, one U.S., one French, were similar in design, with relatively unimpaired SAH patients randomized to nimodipine or placebo. In each, a judgment was made as to whether any late-developing deficit was due to spasm or other causes, and the deficits were graded. Both studies showed significantly fewer severe deficits due to spasm in the nimodipine group; the second (French) study showed fewer spasm-related deficits of all severities. No effect was seen on deficits not related to spasm.
• Hunt and Hess Grade | ||||||
•• p=0.03 | ||||||
| Patients | ||||||
| Study | Dose | Grade• | Number Analyzed | Any Deficit Due to Spasm | Numbers with Severe Deficit | |
| U.S. | 20 to 30 mg | I to III | Nimodipine Placebo | 56 60 | 13 16 | 1 8•• |
| French | 60 mg | I to III | Nimodipine Placebo | 31 39 | 4 11 | 2 10•• |
A third, large, study was performed in the United Kingdom in SAH patients with all grades of severity (but 89% were in Grades I to III). Nimodipine was dosed 60 mg every 4 hours. Outcomes were not defined as spasm related or not but there was a significant reduction in the overall rate of infarction and severely disabling neurological outcome at 3 months:
• p=0.0444 - good and moderate vs severe and dead | ||
•• p=0.001 - severe disability | ||
••• p=0.056 - death | ||
| Nimodipine | Placebo | |
| Total patients | 278 | 276 |
| Good recovery | 199• | 169 |
| Moderate disability | 24 | 16 |
| Severe disability | 12•• | 31 |
| Death | 43••• | 60 |
A Canadian study entered much sicker patients, (Hunt and Hess Grades III to V), who had a high rate of death and disability, and used a dose of 90 mg every 4 hours, but was otherwise similar to the first two studies. Analysis of delayed ischemic deficits, many of which result from spasm, showed a significant reduction in spasm-related deficits. Among analyzed patients (72 nimodipine, 82 placebo), there were the following outcomes.
• p = 0.001, nimodipine vs placebo | ||||
| Delayed Ischemic Deficits (DID) | Permanent Deficits | |||
| Nimodipine n (%) | Placebo n (%) | Nimodipine n (%) | Placebo n (%) | |
| DID Spasm Alone | 8 (11)• | 25 (31) | 5 (7)• | 22 (27) |
| DID Spasm Contributing | 18 (25) | 21 (26) | 16 (22) | 17 (21) |
| DID Without Spasm | 7 (10) | 8 (10) | 6 (8) | 7 (9) |
| No DID | 39 (54) | 28 (34) | 45 (63) | 36 (44) |
When data were combined for the Canadian and the United Kingdom studies, the treatment difference on success rate (i.e., good recovery) on the Glasgow Outcome Scale was 25.3% (nimodipine) versus 10.9% (placebo) for Hunt and Hess Grades IV or V. The table below demonstrates that nimodipine tends to improve good recovery of SAH patients with poor neurological status post-ictus, while decreasing the numbers with severe disability and vegetative survival.
• p = 0.045, nimodipine vs placebo | ||
| Glasgow Outcome• | Nimodipine (n=87) | Placebo (n=101) |
| Good Recovery | 22 (25.3%) | 11 (10.9%) |
| Moderate Disability | 8 (9.2%) | 12 (11.9%) |
| Severe Disability | 6 (6.9%) | 15 (14.9%) |
| Vegetative Survival | 4 (4.6%) | 9 (8.9%) |
| Death | 47 (54.0%) | 54 (53.5%) |
HOW SUPPLIED
Nimodipine Capsules 30 mg are available as orange, opaque, oblong shape, soft gelatin capsules, imprinted "HP 512" with black ink. They are supplied as follows:
| Strength | NDC Code | |
| Unit Dose Package of 30: (3 blister cards; each containing 10 capsules) | 30 mg | 23155-512-30 |
| Unit Dose Package of 100: (10 blister cards; each containing 10 capsules) | 30 mg | 23155-512-00 |
The capsules should be stored in the manufacturer's original package.
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature].
Capsules should be protected from light and freezing.
Distributed by:
Avet Pharmaceuticals Inc.
East Brunswick, NJ 08816
1.866.901.DRUG (3784)
![]()
51U000000272US03
Revised: 06/2024