Get your patient on Oxacillin - Oxacillin injection, Solution (Oxacillin)
Oxacillin - Oxacillin injection, Solution prescribing information
INDICATIONS AND USAGE
Oxacillin is indicated in the treatment of infections caused by penicillinase producing staphylococci which have demonstrated susceptibility to the drug. Cultures and susceptibility tests should be performed initially to determine the causative organism and its susceptibility to the drug. (See CLINICAL PHARMACOLOGY - Susceptibility Test Methods .)
Oxacillin may be used to initiate therapy in suspected cases of resistant staphylococcal infections prior to the availability of susceptibility test results. Oxacillin should not be used in infections caused by organisms susceptible to penicillin G. If the susceptibility tests indicate that the infection is due to an organism other than a resistant Staphylococcus , therapy should not be continued with oxacillin.
To reduce the development of drug-resistant bacteria and maintain the effectiveness of Oxacillin Injection, USP and other antibacterial drugs, Oxacillin Injection, USP should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
DOSAGE AND ADMINISTRATION
Oxacillin Injection, USP supplied as a premixed frozen solution is to be administered as a continuous or intermittent intravenous infusion. The usual dose recommendation is as follows:
Adults | |
250-500 mg | I.V. every 4-6 hours (mild to moderate infections) |
1 gram | I.V. every 4-6 hours (severe infections) |
This container system may be inappropriate for the dosage requirements for children, infants and neonates. Other dosage forms may be more appropriate.
Bacteriologic studies to determine the causative organisms and their susceptibility to oxacillin should always be performed. Duration of therapy varies with the type of severity of infection as well as the overall condition of the patient; therefore, it should be determined by the clinical and bacteriological response of the patient. In severe staphylococcal infections, therapy with oxacillin should be continued for at least 14 days. Therapy should be continued for at least 48 hours after the patient has become afebrile, asymptomatic, and cultures are negative. Treatment of endocarditis and osteomyelitis may require a longer duration of therapy.
Concurrent administration of oxacillin and probenecid increases and prolongs serum penicillin levels. Probenecid decreases the apparent volume of distribution and slows the rate of excretion by competitively inhibiting renal tubular secretion of penicillin. Penicillin-probenecid therapy is generally limited to those infections where very high serum levels of penicillin are necessary.
With intravenous administration, particularly in elderly patients, care should be taken because of the possibility of thrombophlebitis.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit.
Do not add supplementary medication to Oxacillin Injection, USP.
Store in a freezer capable of maintaining a temperature of -20°C/-4°F or less.
DIRECTIONS FOR USE OF GALAXY PLASTIC CONTAINER
Thaw at room temperature (25°C/77°F) or under refrigeration (5°C/41°F). [DO NOT FORCE THAW BY IMMERSION IN WATER BATHS OR BY MICROWAVE IRRADIATION]. Visually inspect the container. If the outlet port protector is damaged, detached, or not present, discard container as sterility may be impaired. Components of the solution may precipitate in the frozen state and will dissolve upon reaching room temperature with little or no agitation. Potency is not affected. Mix after solution has reached room temperature. Check for minute leaks by squeezing bag firmly. If leaks are found, discard solution as sterility may be impaired. Do not use if the solution is cloudy or precipitated or if seals are not intact. The thawed solution is stable for 21 days under refrigeration or 48 hours at room temperature. Do not refreeze.
Use sterile equipment.
Caution: Do not use plastic containers in series connections. Such use could result in air embolism due to residual air being drawn from the primary container before administration of the fluid from the secondary container is complete.
Preparation for intravenous administration
- Suspend container from eyelet support.
- Remove protector from outlet port at bottom of container.
- Attach administration set. Refer to complete directions accompanying set.
CONTRAINDICATIONS
A history of a hypersensitivity (anaphylactic) reaction to any penicillin is a contraindication. Solutions containing dextrose may be contraindicated in patients with known allergy to corn or corn products.
ADVERSE REACTIONS
Body as a Whole
The reported incidence of allergic reactions to penicillin ranges from 0.7 to 10 percent (see WARNINGS ). Sensitization is usually the result of treatment but some individuals have had immediate reactions when first treated. In such cases, it is thought that the patients may have had prior exposure to the drug via trace amounts present in milk and vaccines.
Two types of allergic reactions to penicillins are noted clinically, immediate and delayed.
Immediate reactions usually occur within 20 minutes of administration and range in severity from urticaria and pruritus to angioneurotic edema, laryngospasm, bronchospasm, hypotension, vascular collapse and death. Such immediate anaphylactic reactions are very rare (see WARNINGS ) and usually occur after parenteral therapy but have occurred in patients receiving oral therapy. Another type of immediate reaction, an accelerated reaction, may occur between 20 minutes and 48 hours after administration and may include urticaria, pruritus, and fever. Although laryngeal edema, laryngospasm, and hypotension occasionally occur, fatality is uncommon. Delayed allergic reactions to penicillin therapy usually occur after 48 hours and sometimes as late as 2 to 4 weeks after initiation of therapy. Manifestations of this type of reaction include serum sickness-like symptoms ( i.e. , fever, malaise, urticaria, myalgia, arthralgia, abdominal pain) and various skin rashes. Nausea, vomiting, diarrhea, stomatitis, black or hairy tongue, and other symptoms of gastrointestinal irritation may occur, especially during oral penicillin therapy.
Nervous System Reactions
Neurotoxic reactions similar to those observed with penicillin G may occur with large intravenous doses of oxacillin, especially with patients with renal insufficiency.
Urogenital Reactions
Renal tubular damage and interstitial nephritis have been associated infrequently with the administration of oxacillin. Manifestations of this reaction may include rash, fever, eosinophilia, hematuria, proteinuria, and renal insufficiency.
Gastrointestinal Reactions
Pseudomembranous colitis has been reported with the use of oxacillin. The onset of pseudomembranous colitis symptoms may occur during or after antibiotic treatment (see WARNINGS ).
Metabolic Reactions
Hepatotoxicity, characterized by fever, nausea, and vomiting associated with abnormal liver function tests, mainly elevated SGOT levels, has been associated with the use of oxacillin.
Drug Interactions
Tetracycline, a bacteriostatic antibiotic, may antagonize the bactericidal effect of penicillin and concurrent use of these drugs should be avoided.
Oxacillin blood levels may be prolonged by concurrent administration of probenecid which blocks the renal tubular secretion of penicillins.
DESCRIPTION
Oxacillin Injection, USP is a sterile injectable product containing oxacillin which is added as oxacillin sodium, a semisynthetic penicillin derived from the penicillin nucleus, 6-aminopenicillanic acid. The chemical name of oxacillin sodium is 4-Thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid, 3,3-dimethyl-6-[[(5-methyl-3-phenyl-4- isoxazolyl)carbonyl]-amino]-7-oxo-, monosodium salt, monohydrate, [2S-(2α,5α,6ß)]-. It is resistant to inactivation by the enzyme penicillinase (beta-lactamase). The molecular formula of oxacillin sodium is C 19 H 18 N 3 NaO 5 S•H 2 O. The molecular weight is 441.44.
The structural formula of oxacillin sodium is as follows:
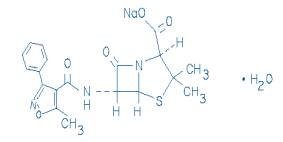
Oxacillin Injection, USP is a frozen, iso-osmotic, sterile, nonpyrogenic premixed 50 mL solution containing 2 g of oxacillin added as oxacillin sodium. Dextrose, USP has been added to the above dosages to adjust osmolality (approximately 300 mg as dextrose hydrous to the 2 g dosages respectively). Sodium Citrate Hydrous, USP has been added as a buffer (approximately 300 mg to the 2 g dosage). The pH has been adjusted with hydrochloric acid and may have been adjusted with sodium hydroxide. The pH is 6.5 (6.0 to 8.5). The solution is intended for intravenous use after thawing to room temperature.
This Galaxy container is fabricated from a specially designed multilayer plastic. Solutions are in contact with the polyethylene layer of this container and can leach out certain chemical components of the plastic in very small amounts within the expiration period. The suitability of the plastic has been confirmed in tests in animals according to the USP biological tests for plastic containers, as well as by tissue culture toxicity studies.
CLINICAL PHARMACOLOGY
Intravenous administration provides peak serum levels approximately 5 minutes after the injection is completed. Slow I.V. administration of 500 mg gives a peak serum level of 43 mcg/mL after 5 minutes with a half-life of 20-30 minutes.
The penicillinase-resistant penicillins bind to serum protein, mainly albumin. The degree of protein binding reported for oxacillin is 94.2% ± 2.1%. Reported values vary with the method of study and the investigator.
The penicillinase-resistant penicillins vary in the extent to which they are distributed in the body fluids. With normal doses, insignificant concentrations are found in the cerebrospinal fluid and aqueous humor. All the drugs in this class are found in therapeutic concentrations in the pleural, bile, and amniotic fluids.
The penicillinase-resistant penicillins are rapidly excreted primarily as unchanged drug in the urine by glomerular filtration and active tubular secretion. The elimination half-life for oxacillin is about 0.5 hours. Nonrenal elimination includes hepatic inactivation and excretion in bile.
Probenecid blocks the renal tubular secretion of penicillins. Therefore, the concurrent administration of probenecid prolongs the elimination of oxacillin and, consequently, increases the serum concentration.
Microbiology
Mechanism of Action
Penicillinase-resistant penicillins exert a bactericidal action against penicillin susceptible microorganisms during the state of active multiplication. All penicillins inhibit the biosynthesis of the bacterial cell wall.
Resistance
Resistance to penicillins may be mediated by destruction of the beta-lactam ring by a beta-lactamase, altered affinity of penicillin for target, or decreased penetration of the antibiotic to reach the target site.
Resistance to oxacillin (or cefoxitin) implies resistance to all other beta-lactam agents, except newer agents with activity against methicillin-resistant Staphylococcus aureus.
Susceptibility Test Methods
For specific information regarding susceptibility test interpretive criteria and associated test methods and quality control standards recognized by FDA for this drug, please see: http://www.fda.gov/STIC .
HOW SUPPLIED1/ STORAGE AND HANDLING
Oxacillin Injection, USP is supplied as a premixed frozen iso-osmotic solution in 50 mL single dose Galaxy plastic containers as follows:
NDC 0338-1015-41 2 grams oxacillin
Store at or below -20°C/-4°F. [See DIRECTIONS FOR USE OF GALAXY PLASTIC CONTAINER ]
Handle frozen product containers with care. Product containers may be fragile in the frozen state.
Mechanism of Action
Penicillinase-resistant penicillins exert a bactericidal action against penicillin susceptible microorganisms during the state of active multiplication. All penicillins inhibit the biosynthesis of the bacterial cell wall.