Sucralfate
Sucralfate Prescribing Information
Sucralfate tablets are indicated in:
- Short-term treatment (up to 8 weeks) of active duodenal ulcer. While healing with sucralfate may occur during the first week or two, treatment should be continued for 4 to 8 weeks unless healing has been demonstrated by x-ray or endoscopic examination.
- Maintenance therapy for duodenal ulcer patients at reduced dosage after healing of acute ulcers.
Antacids may be prescribed as needed for relief of pain but should not be taken within one-half hour before or after sucralfate.
While healing with sucralfate may occur during the first week or two, treatment should be continued for 4 to 8 weeks unless healing has been demonstrated by x-ray or endoscopic examination.
Clinical studies of sucralfate tablets did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy (See
This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function (See
Call your doctor for medical advice about side effects. You may report side effects to Viona Pharmaceuticals Inc. at 1-888-304-5011 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Sucralfate tablets are contraindicated in patients with known hypersensitivity reactions to the active substance or to any of the excipients.
Adverse reactions to sucralfate in clinical trials were minor and only rarely led to discontinuation of the drug. In studies involving over 2,700 patients treated with sucralfate tablets, adverse effects were reported in 129 (4.7%).
Constipation was the most frequent complaint (2%). Other adverse effects reported in less than 0.5% of the patients are listed below by body system:
Post-marketing cases of hypersensitivity have been reported with the use of sucralfate tablets, including dyspnea, lip swelling, pruritus, rash, and urticaria.
Cases of anaphylactic reactions, bronchospasm, laryngeal edema, edema of the mouth, pharyngeal edema, respiratory tract edema and swelling of the face have been reported with an unknown oral formulation of sucralfate.
Bezoars have been reported in patients treated with sucralfate. The majority of patients had underlying medical conditions that may predispose to bezoar formation (such as delayed gastric emptying) or were receiving concomitant enteral tube feedings.
Inadvertent injection of insoluble sucralfate and its insoluble excipients has led to fatal complications, including pulmonary and cerebral emboli. Sucralfate is not intended for inteavenous administration.
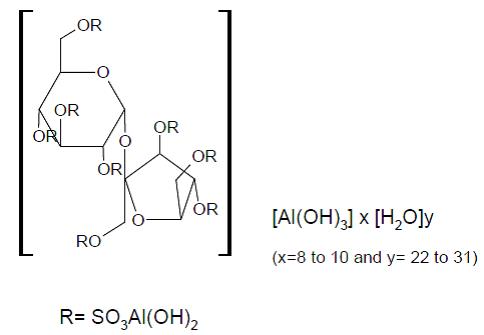
Sucralfate tablets, USP contain sucralfate USP and sucralfate is an α-D-glucopyranoside, β-D fructofuranosyl-, octakis-(hydrogen sulfate), aluminum complex.
Tablets for oral administration contain 1 g of sucralfate, USP.
Also contain: magnesium stearate, microcrystalline cellulose, and corn starch.
Therapeutic category: antiulcer.
Sucralfate is only minimally absorbed from the gastrointestinal tract. The small amounts of the sulfated disaccharide that are absorbed are excreted primarily in the urine.
Although the mechanism of sucralfate's ability to accelerate healing of duodenal ulcers remains to be fully defined, it is known that it exerts its effect through a local, rather than systemic, action.
The following observations also appear pertinent:
1. Studies in human subjects and with animal models of ulcer disease have shown that sucralfate forms an ulcer-adherent complex with proteinaceous exudate at the ulcer site.
2. In vitro, a sucralfate-albumin film provides a barrier to diffusion of hydrogen ions.
3. In human subjects, sucralfate given in doses recommended for ulcer therapy inhibits pepsin activity in gastric juice by 32%.
4. In vitro, sucralfate adsorbs bile salts.
These observations suggest that sucralfate's antiulcer activity is the result of formation of an ulcer-adherent complex that covers the ulcer site and protects it against further attack by acid, pepsin, and bile salts. There are approximately 14 to 16 mEq of acid-neutralizing capacity per 1 g dose of sucralfate.