Get your patient on Timolol Maleate - Timolol Maleate solution (Timolol Maleate)
Timolol Maleate - Timolol Maleate solution prescribing information
INDICATIONS AND USAGE
Preservative-free timolol maleate ophthalmic solution is indicated in the treatment of elevated intraocular pressure in patients with ocular hypertension or open-angle glaucoma.
Preservative-free timolol maleate ophthalmic solution may be used when a patient is sensitive to the preservative in timolol maleate ophthalmic solution, benzalkonium chloride, or when use of a preservative-free topical medication is advisable.
DOSAGE AND ADMINISTRATION
Preservative-free timolol maleate ophthalmic solution is a sterile solution that does not contain a preservative. The solution from one individual unit is to be used immediately after opening for administration to one or both eyes. Since sterility cannot be guaranteed after the individual unit is opened, the remaining contents should be discarded immediately after administration.
Preservative-free timolol maleate ophthalmic solution is available in concentration of 0.5%. The usual starting dose is one drop of 0.25% preservative-free timolol maleate ophthalmic solution in the affected eye(s) administered twice a day. Apply enough gentle pressure on the individual container to obtain a single drop of solution. If the clinical response is not adequate, the dosage may be changed to one drop of 0.5% solution in the affected eye(s) administered twice a day.
Since in some patients the pressure-lowering response to preservative-free timolol maleate ophthalmic solution may require a few weeks to stabilize, evaluation should include a determination of intraocular pressure after approximately 4 weeks of treatment with preservative-free timolol maleate ophthalmic solution.
If the intraocular pressure is maintained at satisfactory levels, the dosage schedule may be changed to one drop once a day in the affected eye(s). Because of diurnal variations in intraocular pressure, satisfactory response to the once-a-day dose is best determined by measuring the intraocular pressure at different times during the day.
Dosages above one drop of 0.5% timolol maleate ophthalmic solution twice a day generally have not been shown to produce further reduction in intraocular pressure. If the patient’s intraocular pressure is still not at a satisfactory level on this regimen, concomitant therapy with other agent(s) for lowering intraocular pressure can be instituted taking into consideration that the preparation(s) used concomitantly may contain one or more preservatives. The concomitant use of two topical beta-adrenergic blocking agents is not recommended (See PRECAUTIONS , Drug Interactions, Beta-adrenergic blocking agents ).
CONTRAINDICATIONS
Preservative-free timolol maleate ophthalmic solution is contraindicated in patients with (1) bronchial asthma; (2) a history of bronchial asthma; (3) severe chronic obstructive pulmonary disease (see WARNINGS ); (4) sinus bradycardia; (5) second or third degree atrioventricular block; (6) overt cardiac failure (see WARNINGS ); (7) cardiogenic shock; or (8) hypersensitivity to any component of this product.
ADVERSE REACTIONS
The most frequently reported adverse experiences have been burning and stinging upon instillation (approximately one in eight patients).
The following additional adverse experiences have been reported less frequently with ocular administration of this or other timolol maleate formulations:
BODY AS A WHOLE
Headache, asthenia/fatigue, and chest pain.
CARDIOVASCULAR
Bradycardia, arrhythmia, hypotension, hypertension, syncope, heart block, cerebral vascular accident, cerebral ischemia, cardiac failure, worsening of angina pectoris, palpitation, cardiac arrest, pulmonary edema, edema, claudication, Raynaud’s phenomenon, and cold hands and feet.
DIGESTIVE
Nausea, diarrhea, dyspepsia, anorexia, and dry mouth.
IMMUNOLOGIC
Systemic lupus erythematosus.
NERVOUS SYSTEM/PSYCHIATRIC
Dizziness, increase in signs and symptoms of myasthenia gravis, paresthesia, somnolence, insomnia, nightmares, behavioral changes and psychic disturbances including depression, confusion, hallucinations, anxiety, disorientation, nervousness, and memory loss.
SKIN
Alopecia and psoriasiform rash or exacerbation of psoriasis.
HYPERSENSITIVITY
Signs and symptoms of systemic allergic reactions including anaphylaxis, angioedema, urticaria, and localized and generalized rash.
RESPIRATORY
Bronchospasm (predominantly in patients with pre-existing bronchospastic disease), respiratory failure, dyspnea, nasal congestion, cough and upper respiratory infections.
ENDOCRINE
Masked symptoms of hypoglycemia in diabetic patients (see WARNINGS ).
SPECIAL SENSES
Signs and symptoms of ocular irritation including conjunctivitis, blepharitis, keratitis, ocular pain, discharge (e.g., crusting), foreign body sensation, itching and tearing, and dry eyes; ptosis; decreased corneal sensitivity; cystoid macular edema; visual disturbances including refractive changes and diplopia; pseudopemphigoid; choroidal detachment following filtration surgery (see PRECAUTIONS , General ); and tinnitus.
UROGENITAL
Retroperitoneal fibrosis, decreased libido, impotence, and Peyronie's disease. The following additional adverse effects have been reported in clinical experience with ORAL timolol maleate or other ORAL beta blocking agents, and may be considered potential effects of ophthalmic timolol maleate: Allergic : Erythematous rash, fever combined with aching and sore throat, laryngospasm with respiratory distress; Body as a Whole : Extremity pain, decreased exercise tolerance, weight loss; Cardiovascular : Worsening of arterial insufficiency, vasodilatation; Digestive : Gastrointestinal pain, hepatomegaly, vomiting, mesenteric arterial thrombosis, ischemic colitis; Hematologic : Nonthrombocytopenic purpura, thrombocytopenic purpura, agranulocytosis; Endocrine : Hyperglycemia, hypoglycemia; Skin : Pruritus, skin irritation, increased pigmentation, sweating; Musculoskeletal : Arthralgia; Nervous System/Psychiatric : Vertigo, local weakness, diminished concentration, reversible mental depression progressing to catatonia, an acute reversible syndrome characterized by disorientation for time and place, emotional lability, slightly clouded sensorium, and decreased performance on neuropsychometrics; Respiratory : Rales, bronchial obstruction; Urogenital : Urination difficulties.
To report SUSPECTED ADVERSE REACTIONS, contact Sentiss at 1-855-573-6847 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
DESCRIPTION
Timolol maleate is a non-selective beta-adrenergic receptor blocking agent. Its chemical name is (-)-1-( tert -butylamino)-3-[(4-morpholino-1,2,5-thiadiazol-3-yl)oxy]-2-propanol maleate (1:1) (salt). Timolol maleate possesses an asymmetric carbon atom in its structure and is provided as the levo-isomer. The optical rotation of timolol maleate is:
25°
[α] in 1.0N HCl (C = 5%) = -12.2° (-11.7° to -12.5°)
405 nm
Its molecular formula is C 13 H 24 N 4 O 3 S•C 4 H 4 O 4 , and its structural formula is:
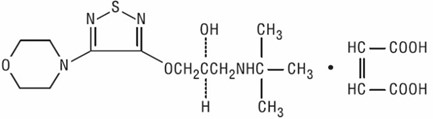
Timolol maleate has a molecular weight of 432.50. It is a white, odorless, crystalline powder which is soluble in water, methanol, and alcohol. Timolol maleate is stable at room temperature.
Timolol maleate ophthalmic solution USP is supplied as the preservative-free formulation.
Preservative-free timolol maleate ophthalmic solution USP is supplied in a single-dose vial, as a sterile, isotonic, buffered, aqueous solution of timolol maleate in one dosage strength. The pH of the solution is approximately 7.0, and the osmolarity is 252-328 mOsm. Each mL of preservative-free timolol maleate ophthalmic solution USP, 0.5% contains 5 mg of timolol (6.8 mg of timolol maleate). Inactive ingredients: monobasic and dibasic sodium phosphate, sodium hydroxide to adjust pH, and water for injection.
CLINICAL PHARMACOLOGY
Mechanism of Action
Timolol maleate is a beta 1 and beta 2 (non-selective) adrenergic receptor blocking agent that does not have significant intrinsic sympathomimetic, direct myocardial depressant, or local anesthetic (membrane-stabilizing) activity.
Beta-adrenergic receptor blockade reduces cardiac output in both healthy subjects and patients with heart disease. In patients with severe impairment of myocardial function, beta-adrenergic receptor blockade may inhibit the stimulatory effect of the sympathetic nervous system necessary to maintain adequate cardiac function.
Beta-adrenergic receptor blockade in the bronchi and bronchioles results in increased airway resistance from unopposed parasympathetic activity. Such an effect in patients with asthma or other bronchospastic conditions is potentially dangerous.
Timolol maleate ophthalmic solution, when applied topically on the eye, has the action of reducing elevated as well as normal intraocular pressure, whether or not accompanied by glaucoma. Elevated intraocular pressure is a major risk factor in the pathogenesis of glaucomatous visual field loss. The higher the level of intraocular pressure, the greater the likelihood of glaucomatous visual field loss and optic nerve damage.
The onset of reduction in intraocular pressure following administration of timolol maleate ophthalmic solution can usually be detected within one-half hour after a single dose. The maximum effect usually occurs in one to two hours, and significant lowering of intraocular pressure can be maintained for periods as long as 24 hours with a single dose. Repeated observations over a period of one year indicate that the intraocular pressure-lowering effect of timolol maleate ophthalmic solution is well maintained.
The precise mechanism of the ocular hypotensive action of timolol maleate ophthalmic solution is not clearly established at this time. Tonography and fluorophotometry studies in man suggest that its predominant action may be related to reduced aqueous formation. However, in some studies a slight increase in outflow facility was also observed.
Pharmacokinetics
In a study of plasma drug concentration in six subjects, the systemic exposure to timolol was determined following twice daily administration of timolol maleate ophthalmic solution, 0.5%. The mean peak plasma concentration following morning dosing was 0.46 ng/mL and following afternoon dosing was 0.35 ng/mL.
Clinical Studies
In controlled multiclinic studies in patients with untreated intraocular pressures of 22 mmHg or greater, timolol maleate ophthalmic solution, 0.25% or 0.5% administered twice a day produced a greater reduction in intraocular pressure than 1, 2, 3, or 4% pilocarpine solution administered four times a day or 0.5, 1, or 2% epinephrine hydrochloride solution administered twice a day.
In these studies, timolol maleate ophthalmic solution was generally well tolerated and produced fewer and less severe side effects than either pilocarpine or epinephrine. A slight reduction of resting heart rate in some patients receiving timolol maleate ophthalmic solution (mean reduction 2.9 beats/minute standard deviation 10.2) was observed.
HOW SUPPLIED
Preservative-free sterile timolol maleate ophthalmic solution USP is a clear, colorless to light yellow solution.
Preservative-free timolol maleate ophthalmic solution USP, 0.5% timolol equivalent, is supplied in single-dose vial, a clear low density polyethylene unit dose container. Each individual unit contains 0.3 mL of solution, and is available in a foil laminate overwrapped pouch as follows:
NDC 72485-602-60; 0.3 mL Single-dose vials in a carton of 60.
Storage
Store at room temperature, 15° to 30°C (59° to 86°F). Protect from freezing. Protect from light.
Because evaporation can occur through the unprotected polyethylene unit dose container and prolonged exposure to direct light can modify the product, the unit dose container should be kept in the protective foil overwrap and used within one month after the foil package has been opened.
Distributed by: Armas Pharmaceuticals, Inc. Freehold, NJ 07728 USA
Manufactured by: Holopack Verpackungstechnik GmbH, Bahnhofstrasse 18, Sulzbach-Laufen, Germany 74429 for Sentiss Origin Germany
Rev. 01/2023