Triamcinolone Acetonide
Triamcinolone Acetonide Prescribing Information
Triamcinolone Acetonide Ointment is indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses.
Apply a thin film of the 0.1% Triamcinolone Acetonide Ointment, as appropriate, to the affected area two to three times daily.
Topical corticosteroids are contraindicated in those patients with a history of hypersensitivity to any of the components of the preparation.
The following local adverse reactions are reported infrequently with topical corticosteroids, but may occur more frequently with the use of occlusive dressings. These reactions are listed in an approximate decreasing order of occurrence: burning, itching, irritation, dryness, folliculitis, hypertrichosis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, maceration of the skin, secondary infection, skin atrophy, striae, and miliaria.
The topical corticosteroids constitute a class of primarily synthetic steroids used as anti-inflammatory and anti-pruritic agents. The steroids in this class include triamcinolone acetonide. Triamcinolone acetonide is designated chemically as pregna-1,4-diene-3,20-dione, 9-fluoro-11,21-dihydroxy-16,17-[(1-methylethylidene)bis(oxy)]-, (11β,16α)-. The structural formula is:
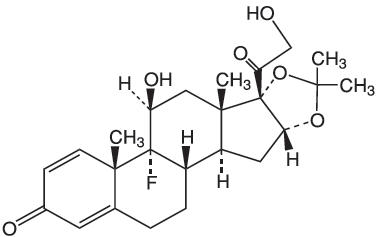 | |
| Molecular Weight: 434.51 | Molecular Formula: C 24H 31FO 6 |
Each gram of Triamcinolone Acetonide Ointment USP, 0.1% contains 1 mg triamcinolone acetonide, in an ointment base of fractionated coconut oil and white petrolatum, with methylparaben and propylparaben as preservatives.
Topical corticosteroids share anti-inflammatory, anti-pruritic and vasoconstrictive actions. The mechanism of anti-inflammatory activity of the topical corticosteroids is unclear. Various laboratory methods, including vasoconstrictor assays, are used to compare and predict potencies and/or clinical efficacies of the topical corticosteroids. There is some evidence to suggest that a recognizable correlation exists between vasoconstrictor potency and therapeutic efficacy in man.