Get your patient on Varenicline Tartrate - Varenicline Tartrate tablet, Film Coated (Varenicline Tartrate)
Varenicline Tartrate - Varenicline Tartrate tablet, Film Coated prescribing information
INDICATIONS AND USAGE
Varenicline tablets are indicated for use as an aid to smoking cessation treatment.
DOSAGE AND ADMINISTRATION
- Begin varenicline tablets dosing one week before the date set by the patient to stop smoking. Alternatively, the patient can begin varenicline tablets dosing and then quit smoking between days 8 and 35 of treatment. (2.1 )
- Starting Week: 0.5 mg once daily on days 1-3 and 0.5 mg twice daily on days 4-7. (2.1 )
- Continuing Weeks: 1 mg twice daily for a total of 12 weeks. (2.1 )
- An additional 12 weeks of treatment is recommended for successful quitters to increase likelihood of long-term abstinence. (2.1 )
- Consider a gradual approach to quitting smoking with varenicline tablets for patients who are sure that they are not able or willing to quit abruptly. Patients should begin varenicline tablets dosing and reduce smoking by 50% from baseline within the first four weeks, by an additional 50% in the next four weeks, and continue reducing with the goal of reaching complete abstinence by 12 weeks. Continue treatment for an additional 12 weeks, for a total of 24 weeks. (2.1 )
- Severe Renal Impairment (estimated creatinine clearance less than 30 mL/min): Begin with 0.5 mg once daily and titrate to 0.5 mg twice daily. For patients with end-stage renal disease undergoing hemodialysis, a maximum of 0.5 mg daily may be given if tolerated. (2.2 )
- Consider dose reduction for patients who cannot tolerate adverse effects. (2.1 )
- Another attempt at treatment is recommended for those who fail to stop smoking or relapse when factors contributing to the failed attempt have been addressed. (2.1 )
- Provide patients with appropriate educational materials and counseling to support the quit attempt. (2.1 )
Usual Dosage for Adults
Smoking cessation therapies are more likely to succeed for patients who are motivated to stop smoking and who are provided additional advice and support. Provide patients with appropriate educational materials and counseling to support the quit attempt.
The patient should set a date to stop smoking. Begin varenicline tablets dosing one week before this date. Alternatively, the patient can begin varenicline tablets dosing and then quit smoking between days 8 and 35 of treatment.
Varenicline tablets should be taken orally after eating and with a full glass of water.
The recommended dose of varenicline tablets is 1 mg twice daily following a 1-week titration as follows:
Days 1 – 3: | 0.5 mg once daily |
Days 4 – 7: | 0.5 mg twice daily |
Day 8 – end of treatment: | 1 mg twice daily |
Patients should be treated with varenicline tablets for 12 weeks. For patients who have successfully stopped smoking at the end of 12 weeks, an additional course of 12 weeks treatment with varenicline tablets is recommended to further increase the likelihood of long-term abstinence.
For patients who are sure that they are not able or willing to quit abruptly, consider a gradual approach to quitting smoking with varenicline tablets. Patients should begin varenicline tablets dosing and reduce smoking by 50% from baseline within the first four weeks, by an additional 50% in the next four weeks, and continue reducing with the goal of reaching complete abstinence by 12 weeks. Continue varenicline tablets treatment for an additional 12 weeks, for a total of 24 weeks of treatment. Encourage patients to attempt quitting sooner if they feel ready [see Clinical Studies (14.5) ] .
Patients who are motivated to quit, and who did not succeed in stopping smoking during prior varenicline tablets therapy for reasons other than intolerability due to adverse events or who relapsed after treatment, should be encouraged to make another attempt with varenicline tablets once factors contributing to the failed attempt have been identified and addressed.
Consider a temporary or permanent dose reduction in patients who cannot tolerate the adverse effects of varenicline tablets.
Dosage in Special Populations
Patients with Impaired Renal Function
No dosage adjustment is necessary for patients with mild to moderate renal impairment. For patients with severe renal impairment (estimated creatinine clearance less than 30 mL per min), the recommended starting dose of varenicline tablets is 0.5 mg once daily. The dose may then be titrated as needed to a maximum dose of 0.5 mg twice daily. For patients with end-stage renal disease undergoing hemodialysis, a maximum dose of 0.5 mg once daily may be administered if tolerated [see Use in Specific Populations (8.6) , Clinical Pharmacology (12.3) ] .
Elderly and Patients with Impaired Hepatic Function
No dosage adjustment is necessary for patients with hepatic impairment. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function [see Use in Specific Populations (8.5) ].
DOSAGE FORMS AND STRENGTHS
Modified capsule shaped tablets: 0.5 mg (white to off-white, film coated tablets debossed with 'L' on one side and '11' on other side) and 1 mg (light pink to pink color, film coated tablets debossed with 'L' on one side and '12' on other side).
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
Available data have not suggested an increased risk for major birth defects following exposure to varenicline in pregnancy, compared with women who smoke [see Data ]. Smoking during pregnancy is associated with maternal, fetal, and neonatal risks (see Clinical Considerations ) . In animal studies, varenicline did not result in major malformations but caused decreased fetal weights in rabbits when dosed during organogenesis at exposures equivalent to 50 times the exposure at the maximum recommended human dose (MRHD). Additionally, administration of varenicline to pregnant rats during organogenesis through lactation produced developmental toxicity in offspring at maternal exposures equivalent to 36 times human exposure at the MRHD [see Data ] .
The estimated background risk of oral clefts is increased by approximately 30% in infants of women who smoke during pregnancy, compared to pregnant women who do not smoke. The background risk of other major birth defects and miscarriage for the indicated population are unknown. In the US general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
Smoking during pregnancy causes increased risks of orofacial clefts, premature rupture of membranes, placenta previa, placental abruption, ectopic pregnancy, fetal growth restriction and low birth weight, stillbirth, preterm delivery and shortened gestation, neonatal death, sudden infant death syndrome and reduction of lung function in infants. It is not known whether quitting smoking with varenicline tablets during pregnancy reduces these risks.
Data
Human Data
A population-based observational cohort study using the national registers of Denmark and Sweden compared pregnancy and birth outcomes among women exposed to varenicline (N=335, includes 317 first trimester exposed) with women who smoked during pregnancy (N=78,412) and with non-smoking pregnant women (N=806,438). The prevalence of major malformations, the primary outcome, was similar in all groups, including between smoking and non-smoking groups. The prevalence of adverse perinatal outcomes in the varenicline-exposed cohort was not greater than in the cohort of women who smoked, and differed somewhat between the three cohorts. The prevalences of the primary and secondary outcomes are shown in Table 6.
Table 6. Summary of Primary and Secondary Outcomes for Three Birth Cohorts
Outcome | Varenicline Cohort (n=335) | Smoking Cohort (n=78,412) | Non-Smoking Cohort (n=806,438) |
Major congenital malformation• | 12 / 334 (3.6%) | 3,382 / 78,028 (4.3%) | 33,950 /804,020 (4.2%) |
Stillbirth | 1 (0.3%) | 384 (0.5%) | 2,418 (0.3%) |
Small for gestational age | 42 (12.5%) | 13,433 (17.1%) | 73,135 (9.1%) |
Preterm birth | 25 (7.5%) | 6,173 (7.9%) | 46,732 (5.8%) |
Premature rupture of membranes | 12 (3.6%) | 4,246 (5.4%) | 30,641 (3.8%) |
Sudden infant death syndrome•• | 0/307 (0.0%) | 51/71,720 (0.1%) | 58/755,939 (<0.1%) |
•Included only live births in the cohorts. Prevalence among first trimester varenicline-exposed pregnancies (11/317 [3.5%]).
••There was a lag in death data in Denmark, so the cohorts were smaller.
The study limitations include the inability to capture malformations in pregnancies that do not result in a live birth, and possible misclassification of outcome and of exposure to varenicline or to smoking.
Other small epidemiological studies of pregnant women exposed to varenicline did not identify an association with major malformations, consistent with the Danish and Swedish observational cohort study. Methodological limitations of these studies include small samples and lack of adequate controls.
Overall, available studies cannot definitely establish or exclude any varenicline-associated risk during pregnancy.
Animal Data
Pregnant rats and rabbits received varenicline succinate during organogenesis at oral doses up to 15 and 30 mg/kg/day, respectively. While no fetal structural abnormalities occurred in either species, maternal toxicity, characterized by reduced body weight gain, and reduced fetal weights occurred in rabbits at the highest dose (exposures 50 times the human exposure at the MRHD of 1 mg twice daily based on AUC). Fetal weight reduction did not occur in rabbits at exposures 23 times the human exposure at the MRHD based on AUC.
In a pre- and postnatal development study, pregnant rats received up to 15 mg/kg/day of oral varenicline succinate from organogenesis through lactation. Maternal toxicity, characterized by a decrease in body weight gain was observed at 15 mg/kg/day (36 times the human exposure at the MRHD based on AUC). However, decreased fertility and increased auditory startle response occurred in offspring at the highest maternal dose of 15 mg/kg/day.
Lactation
Risk Summary
There are no data on the presence of varenicline in human milk, the effects on the breastfed infant, or the effects on milk production. In animal studies varenicline was present in milk of lactating rats [see Data ] . However, due to species-specific differences in lactation physiology, animal data may not reliably predict drug levels in human milk. The lack of clinical data during lactation precludes a clear determination of the risk of varenicline tablets to an infant during lactation; however the developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for varenicline tablets and any potential adverse effects on the breastfed child from varenicline tablets or from the underlying maternal condition.
Clinical Considerations
Because there are no data on the presence of varenicline in human milk and the effects on the breastfed infant, breastfeeding women should monitor their infant for seizures and excessive vomiting, which are adverse reactions that have occurred in adults that may be clinically relevant in breastfeeding infants.
Data
In a pre- and postnatal development study, pregnant rats received up to 15 mg/kg/day of oral varenicline succinate through gestation and lactation. Mean serum concentrations of varenicline in the nursing pups were 5–22% of maternal serum concentrations.
Pediatric Use
Varenicline tablets are not recommended for use in pediatric patients 16 years of age or younger because its efficacy in this population was not demonstrated.
Single and multiple-dose pharmacokinetics of varenicline have been investigated in pediatric patients aged 12 to 17 years old (inclusive) and were approximately dose-proportional over the 0.5 mg to 2 mg daily dose range studied. Steady-state systemic exposure in adolescent patients of bodyweight >55 kg, as assessed by AUC (0-24), was comparable to that noted for the same doses in the adult population. When 0.5 mg BID was given, steady-state daily exposure of varenicline was, on average, higher (by approximately 40%) in adolescent patients with bodyweight ≤55 kg compared to that noted in the adult population.
The efficacy and safety of varenicline was evaluated in a randomized, double-blind, placebo-controlled study of 312 patients aged 12 to 19 years, who smoked an average of at least 5 cigarettes per day during the 30 days prior to recruitment, had a score of at least 4 on the Fagerstrom Test for Nicotine Dependence scale, and at least one previous failed quit attempt. Patients were stratified by age (12 to 16 years of age, n = 216 and 17 to 19 years of age, n = 96) and by body weight (≤55 kg and >55 kg). Patients were randomized to one of two doses of varenicline, adjusted by weight to provide plasma levels in the efficacious range (based on adult studies) and placebo. Patients received treatment for 12 weeks, followed by a non-treatment period of 40 weeks, along with age-appropriate counseling throughout the study. Results from this study showed that varenicline, at either dose studied, did not improve continuous abstinence rates at weeks 9 through 12 of treatment compared with placebo in subjects 12 to 19 years of age. The varenicline safety profile in this study was consistent with that observed in adult studies.
Geriatric Use
A combined single- and multiple-dose pharmacokinetic study demonstrated that the pharmacokinetics of 1 mg varenicline given once daily or twice daily to 16 healthy elderly male and female smokers (aged 65–75 years) for 7 consecutive days was similar to that of younger subjects. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Varenicline is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function [see Dosage and Administration (2.2) ] .
No dosage adjustment is recommended for elderly patients.
Renal Impairment
Varenicline is substantially eliminated by renal glomerular filtration along with active tubular secretion. Dose reduction is not required in patients with mild to moderate renal impairment. For patients with severe renal impairment (estimated creatinine clearance <30 mL/min), and for patients with end-stage renal disease undergoing hemodialysis, dosage adjustment is needed [see Dosage and Administration (2.2) , Clinical Pharmacology (12.3) ].
CONTRAINDICATIONS
Varenicline tablets are contraindicated in patients with a known history of serious hypersensitivity reactions or skin reactions to varenicline tablets.
WARNINGS AND PRECAUTIONS
- Neuropsychiatric Adverse Events : Postmarketing reports of serious or clinically significant neuropsychiatric adverse events have included changes in mood (including depression and mania), psychosis, hallucinations, paranoia, delusions, homicidal ideation, aggression, hostility, agitation, anxiety, and panic, as well as suicidal ideation, suicide attempt, and completed suicide. Observe patients attempting to quit smoking with varenicline tablets for the occurrence of such symptoms and instruct them to discontinue varenicline tablets and contact a healthcare provider if they experience such adverse events. (5.1 )
- Seizures : New or worsening seizures have been observed in patients taking varenicline tablets. Varenicline tablets should be used cautiously in patients with a history of seizures or other factors that can lower the seizure threshold. (5.2 )
- Interaction with Alcohol : Increased effects of alcohol have been reported. Instruct patients to reduce the amount of alcohol they consume until they know whether varenicline tablets affects them. (5.3 )
- Accidental Injury : Accidental injuries (e.g., traffic accidents) have been reported. Instruct patients to use caution driving or operating machinery until they know how varenicline tablets may affect them. (5.4 )
- Cardiovascular Events : Patients with underlying cardiovascular (CV) disease may be at increased risk of CV events; however, these concerns must be balanced with the health benefits of smoking cessation. Instruct patients to notify their healthcare providers of new or worsening CV symptoms and to seek immediate medical attention if they experience signs and symptoms of myocardial infarction (MI) or stroke. (5.5 and 6.1 )
- Somnambulism : Cases of somnambulism have been reported in patients taking varenicline tablets. Some cases described harmful behavior to self, others, or property. Instruct patients to discontinue varenicline tablets and notify their healthcare provider if they experience somnambulism. (5.6 and 6.2 )
- Angioedema and Hypersensitivity Reactions : Such reactions, including angioedema, infrequently life-threatening, have been reported. Instruct patients to discontinue varenicline tablets and immediately seek medical care if symptoms occur. (5.7 and 6.2 )
- Serious Skin Reactions : Rare, potentially life-threatening skin reactions have been reported. Instruct patients to discontinue varenicline tablets and contact a healthcare provider immediately at first appearance of skin rash with mucosal lesions. (5.8 and 6.2 )
- Nausea : Nausea is the most common adverse reaction (up to 30% incidence rate). Dose reduction may be helpful. (5.9 )
Neuropsychiatric Adverse Events including Suicidality
Serious neuropsychiatric adverse events have been reported in patients being treated with varenicline tablets [see Adverse Reactions (6.2) ] . These postmarketing reports have included changes in mood (including depression and mania), psychosis, hallucinations, paranoia, delusions, homicidal ideation, aggression, hostility, agitation, anxiety, and panic, as well as suicidal ideation, suicide attempt, and completed suicide. Some patients who stopped smoking may have been experiencing symptoms of nicotine withdrawal, including depressed mood. Depression, rarely including suicidal ideation, has been reported in smokers undergoing a smoking cessation attempt without medication. However, some of these adverse events occurred in patients taking varenicline tablets who continued to smoke.
Neuropsychiatric adverse events occurred in patients without and with pre-existing psychiatric disease; some patients experienced worsening of their psychiatric illnesses. Some neuropsychiatric adverse events, including unusual and sometimes aggressive behavior directed to oneself or others, may have been worsened by concomitant use of alcohol [see Warnings and Precautions (5.3) , Adverse Reactions (6.2) ] . Observe patients for the occurrence of neuropsychiatric adverse events. Advise patients and caregivers that the patient should stop taking varenicline tablets and contact a healthcare provider immediately if agitation, depressed mood, or changes in behavior or thinking that are not typical for the patient are observed, or if the patient develops suicidal ideation or suicidal behavior. The healthcare provider should evaluate the severity of the symptoms and the extent to which the patient is benefiting from treatment, and consider options including dose reduction, continued treatment under closer monitoring, or discontinuing treatment. In many postmarketing cases, resolution of symptoms after discontinuation of varenicline tablets was reported. However, the symptoms persisted in some cases; therefore, ongoing monitoring and supportive care should be provided until symptoms resolve.
The neuropsychiatric safety of varenicline tablets was evaluated in a randomized, double-blind, active and placebo-controlled study that included patients without a history of psychiatric disorder (non-psychiatric cohort, N=3912) and patients with a history of psychiatric disorder (psychiatric cohort, N=4003). In the non-psychiatric cohort, varenicline tablets was not associated with an increased incidence of clinically significant neuropsychiatric adverse events in a composite endpoint comprising anxiety, depression, feeling abnormal, hostility, agitation, aggression, delusions, hallucinations, homicidal ideation, mania, panic, and irritability. In the psychiatric cohort, there were more events reported in each treatment group compared to the non-psychiatric cohort, and the incidence of events in the composite endpoint was higher for each of the active treatments compared to placebo: Risk Differences (RDs) (95%CI) vs. placebo were 2.7% (-0.05, 5.4) for varenicline tablets, 2.2% (-0.5, 4.9) for bupropion, and 0.4% (-2.2, 3.0) for transdermal nicotine. In the non-psychiatric cohort, neuropsychiatric adverse events of a serious nature were reported in 0.1% of varenicline tablets-treated patients and 0.4% of placebo-treated patients. In the psychiatric cohort, neuropsychiatric events of a serious nature were reported in 0.6% of varenicline tablets-treated patients, with 0.5% involving psychiatric hospitalization. In placebo-treated patients, serious neuropsychiatric events occurred in 0.6%, with 0.2% requiring psychiatric hospitalization [see Clinical Studies (14.10) ] .
Seizures
During clinical trials and the postmarketing experience, there have been reports of seizures in patients treated with varenicline tablets. Some patients had no history of seizures, whereas others had a history of seizure disorder that was remote or well-controlled. In most cases, the seizure occurred within the first month of therapy. Weigh this potential risk against the potential benefits before prescribing varenicline tablets in patients with a history of seizures or other factors that can lower the seizure threshold. Advise patients to discontinue varenicline tablets and contact a healthcare provider immediately if they experience a seizure while on treatment [see Adverse Reactions (6.2) ] .
Interaction with Alcohol
There have been postmarketing reports of patients experiencing increased intoxicating effects of alcohol while taking varenicline tablets. Some cases described unusual and sometimes aggressive behavior, and were often accompanied by amnesia for the events. Advise patients to reduce the amount of alcohol they consume while taking varenicline tablets until they know whether varenicline tablets affects their tolerance for alcohol [see Adverse Reactions (6.2) ] .
Accidental Injury
There have been postmarketing reports of traffic accidents, near-miss incidents in traffic, or other accidental injuries in patients taking varenicline tablets. In some cases, the patients reported somnolence, dizziness, loss of consciousness or difficulty concentrating that resulted in impairment, or concern about potential impairment, in driving or operating machinery. Advise patients to use caution driving or operating machinery or engaging in other potentially hazardous activities until they know how varenicline tablets may affect them.
Cardiovascular Events
A comprehensive evaluation of cardiovascular (CV) risk with varenicline tablets suggests that patients with underlying CV disease may be at increased risk; however, these concerns must be balanced with the health benefits of smoking cessation. CV risk has been assessed for varenicline tablets in randomized controlled trials (RCT) and meta-analyses of RCTs. In a smoking cessation trial in patients with stable CV disease, CV events were infrequent overall; however, nonfatal myocardial infarction (MI) and nonfatal stroke occurred more frequently in patients treated with varenicline tablets compared to placebo. All-cause and CV mortality was lower in patients treated with varenicline tablets [see Clinical Studies (14.8) ]. This study was included in a meta-analysis of 15 varenicline tablets efficacy trials in various clinical populations that showed an increased hazard ratio for Major Adverse Cardiovascular Events (MACE) of 1.95; however, the finding was not statistically significant (95% CI: 0.79, 4.82). In the large postmarketing neuropsychiatric safety outcome trial, an analysis of adjudicated MACE events was conducted for patients while in the trial and during a 28-week non-treatment extension period. Few MACE events occurred during the trial; therefore, the findings did not contribute substantively to the understanding of CV risk with varenicline tablets. Instruct patients to notify their healthcare providers of new or worsening CV symptoms and to seek immediate medical attention if they experience signs and symptoms of MI or stroke [see Clinical Studies (14.10) ].
Somnambulism
Cases of somnambulism have been reported in patients taking varenicline tablets. Some cases described harmful behavior to self, others, or property. Instruct patients to discontinue varenicline tablets and notify their healthcare provider if they experience somnambulism [see Adverse Reactions (6.2) ].
Angioedema and Hypersensitivity Reactions
There have been postmarketing reports of hypersensitivity reactions including angioedema in patients treated with varenicline tablets [see Adverse Reactions (6.2) , Patient Counseling Information (17) ]. Clinical signs included swelling of the face, mouth (tongue, lips, and gums), extremities, and neck (throat and larynx). There were infrequent reports of life-threatening angioedema requiring emergent medical attention due to respiratory compromise. Instruct patients to discontinue varenicline tablets and immediately seek medical care if they experience these symptoms.
Serious Skin Reactions
There have been postmarketing reports of rare but serious skin reactions, including Stevens-Johnson Syndrome and erythema multiforme, in patients using varenicline tablets [see Adverse Reactions (6.2) ] . As these skin reactions can be life-threatening, instruct patients to stop taking varenicline tablets and contact a healthcare provider immediately at the first appearance of a skin rash with mucosal lesions or any other signs of hypersensitivity.
Nausea
Nausea was the most common adverse reaction reported with varenicline tablets treatment. Nausea was generally described as mild or moderate and often transient; however, for some patients, it was persistent over several months. The incidence of nausea was dose-dependent. Initial dose-titration was beneficial in reducing the occurrence of nausea. For patients treated to the maximum recommended dose of 1 mg twice daily following initial dosage titration, the incidence of nausea was 30% compared with 10% in patients taking a comparable placebo regimen. In patients taking varenicline tablets 0.5 mg twice daily following initial titration, the incidence was 16% compared with 11% for placebo. Approximately 3% of patients treated with varenicline tablets 1 mg twice daily in studies involving 12 weeks of treatment discontinued treatment prematurely because of nausea. For patients with intolerable nausea, a dose reduction should be considered.
ADVERSE REACTIONS
The following serious adverse reactions were reported in postmarketing experience and are discussed in greater detail in other sections of the labeling:
- Neuropsychiatric Adverse Events including Suicidality [see Warnings and Precautions (5.1) ]
- Seizures [see Warnings and Precautions (5.2) ]
- Interaction with Alcohol [see Warnings and Precautions (5.3) ]
- Accidental Injury [see Warnings and Precautions (5.4) ]
- Cardiovascular Events [see Warnings and Precautions (5.5) ]
- Somnambulism [see Warnings and Precautions (5.6) ]
- Angioedema and Hypersensitivity Reactions [see Warnings and Precautions (5.7 )]
- Serious Skin Reactions [see Warnings and Precautions (5.8) ]
In the placebo-controlled premarketing studies, the most common adverse events associated with varenicline tablets (>5% and twice the rate seen in placebo-treated patients) were nausea, abnormal (vivid, unusual, or strange) dreams, constipation, flatulence, and vomiting.
The treatment discontinuation rate due to adverse events in patients dosed with 1 mg twice daily was 12% for varenicline tablets, compared to 10% for placebo in studies of three months' treatment. In this group, the discontinuation rates that are higher than placebo for the most common adverse events in varenicline tablets-treated patients were as follows: nausea (3% vs. 0.5% for placebo), insomnia (1.2% vs. 1.1% for placebo), and abnormal dreams (0.3% vs. 0.2% for placebo).
Smoking cessation, with or without treatment, is associated with nicotine withdrawal symptoms and has also been associated with the exacerbation of underlying psychiatric illness.
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, the adverse reactions rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
During the premarketing development of varenicline tablets, over 4500 subjects were exposed to varenicline tablets, with over 450 treated for at least 24 weeks and approximately 100 for a year. Most study participants were treated for 12 weeks or less.
The most common adverse event associated with varenicline tablets treatment is nausea, occurring in 30% of patients treated at the recommended dose, compared with 10% in patients taking a comparable placebo regimen [see Warnings and Precautions (5.9) ].
Table 1 shows the adverse events for varenicline tablets and placebo in the 12- week fixed dose premarketing studies with titration in the first week [Studies 2 (titrated arm only), 4, and 5]. Adverse events were categorized using the Medical Dictionary for Regulatory Activities (MedDRA, Version 7.1).
MedDRA High Level Group Terms (HLGT) reported in ≥5% of patients in the varenicline tablets 1 mg twice daily dose group, and more commonly than in the placebo group, are listed, along with subordinate Preferred Terms (PT) reported in ≥1% of varenicline tablets patients (and at least 0.5% more frequent than placebo). Closely related Preferred Terms such as 'Insomnia', 'Initial insomnia', 'Middle insomnia', 'Early morning awakening' were grouped, but individual patients reporting two or more grouped events are only counted once.
Table 1. Common Treatment Emergent AEs (%) in the Fixed-Dose, Placebo-Controlled Studies (HLGTs >5% of Patients in the 1 mg BID Varenicline Tablets Group and More Commonly than Placebo and PT ≥1% in the 1 mg BID Varenicline Tablets Group, and 1 mg BID Varenicline Tablets at Least 0.5% More than Placebo)
SYSTEM ORGAN CLASS High Level Group Term Preferred Term | Varenicline Tablets 0.5 mg BID N=129 | Varenicline Tablets 1 mg BID N=821 | Placebo N=805 |
GASTROINTESTINAL (GI) | |||
GI Signs and Symptoms | |||
Nausea | 16 | 30 | 10 |
Abdominal Pain • | 5 | 7 | 5 |
Flatulence | 9 | 6 | 3 |
Dyspepsia | 5 | 5 | 3 |
Vomiting | 1 | 5 | 2 |
GI Motility/Defecation Conditions | |||
Constipation | 5 | 8 | 3 |
Gastroesophageal reflux disease | 1 | 1 | 0 |
Salivary Gland Conditions | |||
Dry mouth | 4 | 6 | 4 |
PSYCHIATRIC DISORDERS | |||
Sleep Disorder/Disturbances | |||
Insomnia •• | 19 | 18 | 13 |
Abnormal dreams | 9 | 13 | 5 |
Sleep disorder | 2 | 5 | 3 |
Nightmare | 2 | 1 | 0 |
NERVOUS SYSTEM | |||
Headaches | |||
Headache | 19 | 15 | 13 |
Neurological Disorders | |||
NEC | |||
Dysgeusia | 8 | 5 | 4 |
Somnolence | 3 | 3 | 2 |
Lethargy | 2 | 1 | 0 |
GENERAL DISORDERS | |||
General Disorders NEC | |||
Fatigue/Malaise/Asthenia | 4 | 7 | 6 |
RESPIR/THORACIC/MEDIAST | |||
Respiratory Disorders NEC | |||
Rhinorrhea | 0 | 1 | 0 |
Dyspnea | 2 | 1 | 1 |
Upper Respiratory Tract Disorder | 7 | 5 | 4 |
SKIN/SUBCUTANEOUS TISSUE | |||
Epidermal and Dermal Conditions | |||
Rash | 1 | 3 | 2 |
Pruritis | 0 | 1 | 1 |
METABOLISM and NUTRITION | |||
Appetite/General Nutrition Disorders | |||
Increased appetite | 4 | 3 | 2 |
Decreased appetite/ Anorexia | 1 | 2 | 1 |
• Includes PTs Abdominal (pain, pain upper, pain lower, discomfort, tenderness, distension) and Stomach discomfort
•• Includes PTs Insomnia/Initial insomnia/Middle insomnia/Early morning awakening
The overall pattern and frequency of adverse events during the longer-term premarketing trials was similar to those described in Table 1, though several of the most common events were reported by a greater proportion of patients with long-term use (e.g., nausea was reported in 40% of patients treated with varenicline tablets 1 mg twice daily in a one year study, compared to 8% of placebo-treated patients).
Following is a list of treatment-emergent adverse events reported by patients treated with varenicline tablets during all premarketing clinical trials and updated based on pooled data from 18 placebo-controlled pre- and postmarketing studies, including approximately 5,000 patients treated with varenicline. Adverse events were categorized using MedDRA, Version 16.0. The listing does not include those events already listed in the previous tables or elsewhere in labeling, those events for which a drug cause was remote, those events which were so general as to be uninformative, and those events reported only once which did not have a substantial probability of being acutely life-threatening.
Blood and Lymphatic System Disorders. Infrequent : anemia, lymphadenopathy. Rare : leukocytosis, splenomegaly, thrombocytopenia.
Cardiac Disorders. Infrequent : angina pectoris, myocardial infarction, palpitations, tachycardia. Rare : acute coronary syndrome, arrhythmia, atrial fibrillation, bradycardia, cardiac flutter, cor pulmonale, coronary artery disease, ventricular extrasystoles.
Ear and Labyrinth Disorders . Infrequent : tinnitus, vertigo. Rare : deafness, Meniere's disease.
Endocrine Disorders. Infrequent : thyroid gland disorders.
Eye Disorders. Infrequent : conjunctivitis, eye irritation, eye pain, vision blurred, visual impairment. Rare : blindness transient, cataract subcapsular, dry eye, night blindness, ocular vascular disorder, photophobia, vitreous floaters.
Gastrointestinal Disorders . Frequent : diarrhea, toothache. Infrequent : dysphagia, eructation, gastritis, gastrointestinal hemorrhage, mouth ulceration. Rare : enterocolitis, esophagitis, gastric ulcer, intestinal obstruction, pancreatitis acute.
General Disorders and Administration Site Conditions . Frequent : chest pain. Infrequent : chest discomfort, chills, edema, influenza-like illness, pyrexia.
Hepatobiliary Disorders. Rare : gall bladder disorder.
Investigations . Frequent : liver function test abnormal, weight increased. Infrequent : electrocardiogram abnormal. Rare : muscle enzyme increased, urine analysis abnormal.
Metabolism and Nutrition Disorders . Infrequent : diabetes mellitus, hypoglycemia. Rare : hyperlipidemia, hypokalemia.
Musculoskeletal and Connective Tissue Disorders . Frequent : arthralgia, back pain, myalgia. Infrequent : arthritis, muscle cramp, musculoskeletal pain. Rare : myositis, osteoporosis.
Nervous System Disorders. Frequent : disturbance in attention, dizziness. Infrequent : amnesia, convulsion, migraine, parosmia, syncope, tremor. Rare : balance disorder, cerebrovascular accident, dysarthria, mental impairment, multiple sclerosis, VII th nerve paralysis, nystagmus, psychomotor hyperactivity, psychomotor skills impaired, restless legs syndrome, sensory disturbance, transient ischemic attack, visual field defect.
Psychiatric Disorders. Infrequent : dissociation, libido decreased, mood swings, thinking abnormal. Rare : bradyphrenia, disorientation, euphoric mood.
Renal and Urinary Disorders . Infrequent : nocturia, pollakiuria, urine abnormality. Rare : nephrolithiasis, polyuria, renal failure acute, urethral syndrome, urinary retention.
Reproductive System and Breast Disorders. Frequent: menstrual disorder. Infrequent : erectile dysfunction. Rare : sexual dysfunction.
Respiratory, Thoracic and Mediastinal Disorders . Frequent: respiratory disorders. Infrequent : asthma, epistaxis, rhinitis allergic, upper respiratory tract inflammation.
Rare: pleurisy, pulmonary embolism.
Skin and Subcutaneous Tissue Disorders . Infrequent: acne, dry skin, eczema, erythema, hyperhidrosis, urticaria. Rare: photosensitivity reaction, psoriasis.
Vascular Disorders . Infrequent : hot flush. Rare: thrombosis.
Varenicline tablets has also been studied in postmarketing trials including (1) a trial conducted in patients with chronic obstructive pulmonary disease (COPD), (2) a trial conducted in generally healthy patients (similar to those in the premarketing studies) in which they were allowed to select a quit date between days 8 and 35 of treatment ("alternative quit date instruction trial"), (3) a trial conducted in patients who did not succeed in stopping smoking during prior varenicline tablets therapy, or who relapsed after treatment ("re-treatment trial"), (4) a trial conducted in patients with stable cardiovascular disease, (5) a trial conducted in patients with stable schizophrenia or schizoaffective disorder, (6) a trial conducted in patients with major depressive disorder, (7) a postmarketing neuropsychiatric safety outcome trial in patients without or with a history of psychiatric disorder, (8) a non-treatment extension of the postmarketing neuropsychiatric safety outcome trial that assessed CV safety, (9) a trial in patients who were not able or willing to quit abruptly and who were instructed to quit gradually ("gradual approach to quitting smoking trial").
Adverse events in the trial of patients with COPD (1), in the alternative quit date instruction trial (2), and in the gradual approach to quitting smoking trial (9) were similar to those observed in premarketing studies. In the re-treatment trial (3), the profile of common adverse events was similar to that previously reported, but, in addition, varenicline-treated patients also commonly reported diarrhea (6% vs. 4% in placebo-treated patients), depressed mood disorders and disturbances (6% vs. 1%), and other mood disorders and disturbances (5% vs. 2%).
In the trial of patients with stable cardiovascular disease (4), more types and a greater number of cardiovascular events were reported compared to premarketing studies, as shown in Table 1 and in Table 2 below.
Table 2. Cardiovascular Mortality and Nonfatal Cardiovascular Events (%) with a Frequency >1% in Either Treatment Group in the Trial of Patients with Stable Cardiovascular Disease
Varenicline tablets 1 mg BID N=353 | Placebo N=350 | |
Adverse Events ≥1% in either treatment group | ||
Up to 30 days after treatment | ||
Angina pectoris | 3.7 | 2.0 |
Chest pain | 2.5 | 2.3 |
Peripheral edema | 2.0 | 1.1 |
Hypertension | 1.4 | 2.6 |
Palpitations | 0.6 | 1.1 |
Adjudicated Cardiovascular Mortality (up to 52 weeks) | 0.3 | 0.6 |
Adjudicated Nonfatal Serious Cardiovascular Events ≥1% in either treatment group | ||
Up to 30 days after treatment | ||
Nonfatal MI | 1.1 | 0.3 |
Hospitalization for angina pectoris | 0.6 | 1.1 |
Beyond 30 days after treatment and up to 52 weeks | ||
Need for coronary revascularization• | 2.0 | 0.6 |
Hospitalization for angina pectoris | 1.7 | 1.1 |
New diagnosis of peripheral vascular disease (PVD) or admission for a PVD procedure | 1.4 | 0.6 |
•some procedures were part of management of nonfatal MI and hospitalization for angina
In the trial of patients with stable schizophrenia or schizoaffective disorder (5), 128 smokers on antipsychotic medication were randomized 2:1 to varenicline (1 mg twice daily) or placebo for 12 weeks with 12-week non-drug follow-up. The most common treatment emergent adverse events reported in this trial are shown in Table 3 below.
Table 3. Common Treatment Emergent AEs (%) in the Trial of Patients with Stable Schizophrenia or Schizoaffective Disorder
Varenicline tablets 1 mg BID N=84 | Placebo N=43 | |
Adverse Events ≥10% in the varenicline group | ||
Nausea | 24 | 14 |
Headache | 11 | 19 |
Vomiting | 11 | 9 |
Psychiatric Adverse Events ≥5% and at a higher rate than in the placebo group | ||
Insomnia | 10 | 5 |
For the trial of patients with major depressive disorder (6), the most common treatment emergent adverse events reported are shown in Table 4 below. Additionally, in this trial, patients treated with varenicline were more likely than patients treated with placebo to report one of events related to hostility and aggression (3% vs. 1%).
Table 4. Common Treatment Emergent AEs (%) in the Trial of Patients with Major Depressive Disorder
Varenicline tablets 1 mg BID N=256 | Placebo N=269 | |
Adverse Events ≥10% in either treatment group | ||
Nausea | 27 | 10 |
Headache | 17 | 11 |
Abnormal dreams | 11 | 8 |
Insomnia | 11 | 5 |
Irritability | 11 | 8 |
Psychiatric Adverse Events ≥2% in any treatment group and not included above | ||
Depressed mood disorders and disturbances | 11 | 9 |
Anxiety | 7 | 9 |
Agitation | 7 | 4 |
Tension | 4 | 3 |
Hostility | 2 | 0.4 |
Restlessness | 2 | 2 |
In the trial of patients without or with a history of psychiatric disorder (7), the most common adverse events in subjects treated with varenicline were similar to those observed in premarketing studies. Most common treatment-emergent adverse events reported in this trial are shown in Table 5 below.
Table 5. Treatment Emergent Common AEs (%) in the Trial of Patients without or with a History of Psychiatric Disorder
Varenicline tablets 1 mg BID | Placebo | |
Adverse Events ≥10% in the varenicline group | ||
Entire study population, N | 1982 | 1979 |
Nausea | 25 | 7 |
Headache | 12 | 10 |
Psychiatric Adverse Events ≥2% in any treatment group | ||
Non-psychiatric cohort, N | 975 | 982 |
Abnormal dreams | 8 | 4 |
Agitation | 3 | 3 |
Anxiety | 5 | 6 |
Depressed mood | 3 | 3 |
Insomnia | 10 | 7 |
Irritability | 3 | 4 |
Sleep disorder | 3 | 2 |
Psychiatric cohort, N | 1007 | 997 |
Abnormal dreams | 12 | 5 |
Agitation | 5 | 4 |
Anxiety | 8 | 6 |
Depressed mood | 5 | 5 |
Depression | 5 | 5 |
Insomnia | 9 | 7 |
Irritability | 5 | 7 |
Nervousness | 2 | 3 |
Sleep disorder | 3 | 2 |
In the non-treatment extension of the postmarketing neuropsychiatric safety outcomes trial that assessed CV safety (8), the most common adverse events in subjects treated with varenicline and occurring up to 30 days after last dose of treatment were similar to those observed in premarketing studies.
Postmarketing Experience
The following adverse events have been reported during post-approval use of varenicline tablets. Because these events are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
There have been reports of depression, mania, psychosis, hallucinations, paranoia, delusions, homicidal ideation, aggression, hostility, anxiety, and panic, as well as suicidal ideation, suicide attempt, and completed suicide in patients attempting to quit smoking while taking varenicline tablets [see Warnings and Precautions (5.1) ].
There have been postmarketing reports of new or worsening seizures in patients treated with varenicline tablets [see Warnings and Precautions (5.2) ].
There have been postmarketing reports of patients experiencing increased intoxicating effects of alcohol while taking varenicline tablets. Some reported neuropsychiatric events, including unusual and sometimes aggressive behavior [see Warnings and Precautions (5.1) and (5.3 )].
There have been reports of hypersensitivity reactions, including angioedema [see Warnings and Precautions (5.7) ].
There have also been reports of serious skin reactions, including Stevens-Johnson Syndrome and erythema multiforme, in patients taking varenicline tablets [see Warnings and Precautions (5.8) ].
There have been reports of myocardial infarction (MI) and cerebrovascular accident (CVA) including ischemic and hemorrhagic events in patients taking varenicline tablets. In the majority of the reported cases, patients had pre-existing cardiovascular disease and/or other risk factors. Although smoking is a risk factor for MI and CVA, based on temporal relationship between medication use and events, a contributory role of varenicline cannot be ruled out [see Warnings and Precautions (5.5) ].
There have been reports of hyperglycemia in patients following initiation of varenicline tablets.
There have been reports of somnambulism, some resulting in harmful behavior to self, others, or property in patients treated with varenicline tablets [see Warnings and Precautions (5.6) ].
DRUG INTERACTIONS
Based on varenicline characteristics and clinical experience to date, varenicline tablets has no clinically meaningful pharmacokinetic drug interactions [see Clinical Pharmacology (12.3) ].
Use with Other Drugs for Smoking Cessation
Safety and efficacy of varenicline tablets in combination with other smoking cessation therapies have not been studied.
Bupropion
Varenicline (1 mg twice daily) did not alter the steady-state pharmacokinetics of bupropion (150 mg twice daily) in 46 smokers. The safety of the combination of bupropion and varenicline has not been established.
Nicotine replacement therapy (NRT )
Although co-administration of varenicline (1 mg twice daily) and transdermal nicotine (21 mg/day) for up to 12 days did not affect nicotine pharmacokinetics, the incidence of nausea, headache, vomiting, dizziness, dyspepsia, and fatigue was greater for the combination than for NRT alone. In this study, eight of twenty-two (36%) patients treated with the combination of varenicline and NRT prematurely discontinued treatment due to adverse events, compared to 1 of 17 (6%) of patients treated with NRT and placebo.
Effect of Smoking Cessation on Other Drugs
Physiological changes resulting from smoking cessation, with or without treatment with varenicline tablets, may alter the pharmacokinetics or pharmacodynamics of certain drugs (e.g., theophylline, warfarin, insulin) for which dosage adjustment may be necessary.
DESCRIPTION
Varenicline tablets contain varenicline (as the tartrate salt), which is a partial nicotinic agonist selective for α 4 β 2 nicotinic acetylcholine receptor subtypes.
Varenicline, as the tartrate salt, is a powder which is white to off white to slightly yellow solid with the following chemical name: 7,8,9,10-tetrahydro-6,10-methano-6 H -pyrazino[2,3- h][3]benzazepine, (2 R ,3 R )-2,3-dihydroxybutanedioate (1:1). It is freely soluble in water and very slightly soluble in methanol. Varenicline tartrate has a molecular weight of 361.35 Daltons, and a molecular formula of C 13 H 13 N 3 • C 4 H 6 O 6 . The chemical structure is:
Varenicline tablets are supplied for oral administration in two strengths: a 0.5 mg white to off-white, modified capsule shaped, film-coated tablets debossed with 'L' on one side and '11' on other side and a 1 mg light pink to pink color, modified capsule shaped, film coated tablets debossed with 'L' on one side and '12' on other side. Each 0.5 mg varenicline tablets contains 0.85 mg of varenicline tartrate equivalent to 0.5 mg of varenicline free base; each 1 mg varenicline tablets contains 1.71 mg of varenicline tartrate equivalent to 1 mg of varenicline free base. The following inactive ingredients are included in the tablets: anhydrous dibasic calcium phosphate, butylated hydroxyanisole, colloidal silicon dioxide, croscarmellose sodium, magnesium stearate, maltodextrin, microcrystalline cellulose. The tablet film coating contains hydroxypropyl cellulose, hypromellose, and titanium dioxide. In addition to these, the 1 mg tablet film coating also includes D&C Red #27/phloxine aluminum lake, D&C yellow #10 aluminum lake, and FD&C blue #1/brilliant blue FCF aluminum lake and talc.
CLINICAL PHARMACOLOGY
Mechanism of Action
Varenicline binds with high affinity and selectivity at α4β2 neuronal nicotinic acetylcholine receptors. The efficacy of varenicline tablets in smoking cessation is believed to be the result of varenicline's activity at α4β2 sub-type of the nicotinic receptor where its binding produces agonist activity, while simultaneously preventing nicotine binding to these receptors.
Electrophysiology studies in vitro and neurochemical studies in vivo have shown that varenicline binds to α4β2 neuronal nicotinic acetylcholine receptors and stimulates receptor-mediated activity, but at a significantly lower level than nicotine. Varenicline blocks the ability of nicotine to activate α4β2 receptors and thus to stimulate the central nervous mesolimbic dopamine system, believed to be the neuronal mechanism underlying reinforcement and reward experienced upon smoking. Varenicline is highly selective and binds more potently to α4β2 receptors than to other common nicotinic receptors (>500-fold α3β4, >3,500-fold α7, >20,000-fold α1βγδ), or to nonnicotinic receptors and transporters (>2,000-fold). Varenicline also binds with moderate affinity (Ki = 350 nM) to the 5-HT3 receptor.
Pharmacokinetics
Absorption
Maximum plasma concentrations of varenicline occur typically within 3–4 hours after oral administration. Following administration of multiple oral doses of varenicline, steady-state conditions were reached within 4 days. Over the recommended dosing range, varenicline exhibits linear pharmacokinetics after single or repeated doses.
In a mass balance study, absorption of varenicline was virtually complete after oral administration and systemic availability was ~90%.
Food Effect
Oral bioavailability of varenicline is unaffected by food or time-of-day dosing.
Distribution
Plasma protein binding of varenicline is low (≤20%) and independent of both age and renal function.
Elimination
The elimination half-life of varenicline is approximately 24 hours.
Metabolism
Varenicline undergoes minimal metabolism, with 92% excreted unchanged in the urine.
Excretion
Renal elimination of varenicline is primarily through glomerular filtration along with active tubular secretion possibly via the organic cation transporter, OCT2.
Specific Populations
There are no clinically meaningful differences in varenicline pharmacokinetics due to age, race, gender, smoking status, or use of concomitant medications, as demonstrated in specific pharmacokinetic studies and in population pharmacokinetic analyses.
Age: Geriatric Patients
A combined single- and multiple-dose pharmacokinetic study demonstrated that the pharmacokinetics of 1 mg varenicline given once daily or twice daily to 16 healthy elderly male and female smokers (aged 65–75 years) for 7 consecutive days was similar to that of younger subjects.
Age: Pediatric Patients
Varenicline tablets are not recommended for use in pediatric patients 16 years of age or younger because its efficacy in this population was not demonstrated [see Use in Specific Populations (8.4) ].
Renal Impairment
Varenicline pharmacokinetics were unchanged in subjects with mild renal impairment (estimated creatinine clearance >50 mL/min and ≤80 mL/min). In subjects with moderate renal impairment (estimated creatinine clearance ≥30 mL/min and ≤50 mL/min), varenicline exposure increased 1.5-fold compared with subjects with normal renal function (estimated creatinine clearance >80 mL/min). In subjects with severe renal impairment (estimated creatinine clearance <30 mL/min), varenicline exposure was increased 2.1-fold. In subjects with end-stage-renal disease (ESRD) undergoing a three-hour session of hemodialysis for three days a week, varenicline exposure was increased 2.7-fold following 0.5 mg once daily administration for 12 days. The plasma Cmax and AUC of varenicline noted in this setting were similar to those of healthy subjects receiving 1 mg twice daily [see Dosage and Administration (2.2) , Use in Specific Populations (8.6) ] . Additionally, in subjects with ESRD, varenicline was efficiently removed by hemodialysis [see Overdosage (10) ].
Hepatic Impairment
Due to the absence of significant hepatic metabolism, varenicline pharmacokinetics should be unaffected in patients with hepatic impairment.
Drug-Drug Interactions
In vitro studies demonstrated that varenicline does not inhibit the following cytochrome P450 enzymes (IC50 >6400 ng/mL): 1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, and 3A4/5. Also, in human hepatocytes in vitro , varenicline does not induce the cytochrome P450 enzymes 1A2 and 3A4.
In vitro studies demonstrated that varenicline does not inhibit human renal transport proteins at therapeutic concentrations. Therefore, drugs that are cleared by renal secretion (e.g., metformin [see below] ) are unlikely to be affected by varenicline.
In vitro studies demonstrated the active renal secretion of varenicline is mediated by the human organic cation transporter OCT2. Co-administration with inhibitors of OCT2 (e.g., cimeditine [see below] ) may not necessitate a dose adjustment of varenicline tablets as the increase in systemic exposure to varenicline tablets are not expected to be clinically meaningful. Furthermore, since metabolism of varenicline represents less than 10% of its clearance, drugs known to affect the cytochrome P450 system are unlikely to alter the pharmacokinetics of varenicline tablets [see Clinical Pharmacology (12.3) ] ; therefore, a dose adjustment of varenicline tablets would not be required.
Drug interaction studies were performed with varenicline and digoxin, warfarin, transdermal nicotine, bupropion, cimetidine, and metformin. No clinically meaningful pharmacokinetic drug-drug interactions have been identified.
Metformin
When co-administered to 30 smokers, varenicline (1 mg twice daily) did not alter the steady-state pharmacokinetics of metformin (500 mg twice daily), which is a substrate of OCT2. Metformin had no effect on varenicline steady-state pharmacokinetics.
Cimetidine
Co-administration of an OCT2 inhibitor, cimetidine (300 mg four times daily), with varenicline (2 mg single dose) to 12 smokers increased the systemic exposure of varenicline by 29% (90% CI: 21.5%, 36.9%) due to a reduction in varenicline renal clearance.
Digoxin
Varenicline (1 mg twice daily) did not alter the steady-state pharmacokinetics of digoxin administered as a 0.25 mg daily dose in 18 smokers.
Warfarin
Varenicline (1 mg twice daily) did not alter the pharmacokinetics of a single 25 mg dose of (R, S)-warfarin in 24 smokers. Prothrombin time (INR) was not affected by varenicline. Smoking cessation itself may result in changes to warfarin pharmacokinetics [see Drug Interactions (7.2) ] .
Use with Other Drugs for Smoking Cessation
Bupropion: Varenicline (1 mg twice daily) did not alter the steady-state pharmacokinetics of bupropion (150 mg twice daily) in 46 smokers [see Drug Interactions (7.1) ].
NRT: Although co-administration of varenicline (1 mg twice daily) and transdermal nicotine (21 mg/day) for up to 12 days did not affect nicotine pharmacokinetics, the incidence of adverse reactions was greater for the combination than for NRT alone [see Drug Interactions (7.1) ].
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Lifetime carcinogenicity studies were performed in CD-1 mice and Sprague-Dawley rats. There was no evidence of a carcinogenic effect in mice administered varenicline by oral gavage for 2 years at doses up to 20 mg/kg/day (47 times the maximum recommended human daily (MRHD) exposure based on AUC). Rats were administered varenicline (1, 5, and 15 mg/kg/day) by oral gavage for 2 years. In male rats (n = 65 per sex per dose group), incidences of hibernoma (tumor of the brown fat) were increased at the mid dose (1 tumor, 5 mg/kg/day, 23 times the MRHD exposure based on AUC) and maximum dose (2 tumors, 15 mg/kg/day, 67 times the MRHD exposure based on AUC). The clinical relevance of this finding to humans has not been established. There was no evidence of carcinogenicity in female rats.
Mutagenesis
Varenicline was not genotoxic, with or without metabolic activation, in the following assays: Ames bacterial mutation assay; mammalian CHO/HGPRT assay; and tests for cytogenetic aberrations in vivo in rat bone marrow and in vitro in human lymphocytes.
Impairment of Fertility
There was no evidence of impairment of fertility in either male or female Sprague-Dawley rats administered varenicline succinate up to 15 mg/kg/day (67 and 36 times, respectively, the MRHD exposure based on AUC at 1 mg twice daily). Maternal toxicity, characterized by a decrease in body weight gain, was observed at 15 mg/kg/day. However, a decrease in fertility was noted in the offspring of pregnant rats who were administered varenicline succinate at an oral dose of 15 mg/kg/day. This decrease in fertility in the offspring of treated female rats was not evident at an oral dose of 3 mg/kg/day (9 times the MRHD exposure based on AUC at 1 mg twice daily).
CLINICAL STUDIES
The efficacy of varenicline tablets in smoking cessation was demonstrated in six clinical trials in which a total of 3659 chronic cigarette smokers (≥10 cigarettes per day) were treated with varenicline tablets. In all clinical studies, abstinence from smoking was determined by patient self-report and verified by measurement of exhaled carbon monoxide (CO≤10 ppm) at weekly visits. Among the varenicline tablets-treated patients enrolled in these studies, the completion rate was 65%. Except for the dose-ranging study (Study 1) and the maintenance of abstinence study (Study 6), patients were treated for 12 weeks and then were followed for 40 weeks post-treatment. Most patients enrolled in these trials were white (79-96%). All studies enrolled almost equal numbers of men and women. The average age of patients in these studies was 43 years. Patients on average had smoked about 21 cigarettes per day for an average of approximately 25 years. Patients set a date to stop smoking (target quit date) with dosing starting 1 week before this date.
Seven additional studies evaluated the efficacy of varenicline tablets in patients with cardiovascular disease, in patients with chronic obstructive pulmonary disease [see Clinical Studies (14.7) ] , in patients instructed to select their quit date within days 8 and 35 of treatment [see Clinical Studies (14.4) ], patients with major depressive disorder [see Clinical Studies (14.9) ], patients who had made a previous attempt to quit smoking with varenicline tablets, and either did not succeed in quitting or relapsed after treatment [see Clinical Studies (14.6) ], in patients without or with a history of psychiatric disorder enrolled in a postmarketing neuropsychiatric safety outcome trial [see Warnings and Precautions (5.1) , Clinical Studies (14.10) ], and in patients who were not able or willing to quit abruptly and were instructed to quit gradually [see Clinical studies (14.5) ].
In all studies, patients were provided with an educational booklet on smoking cessation and received up to 10 minutes of smoking cessation counseling at each weekly treatment visit according to Agency for Healthcare Research and Quality guidelines.
Initiation of Abstinence
Study 1
This was a six-week dose-ranging study comparing varenicline tablets to placebo. This study provided initial evidence that varenicline tablets at a total dose of 1 mg per day or 2 mg per day was effective as an aid to smoking cessation.
Study 2
This study of 627 patients compared varenicline tablets 1 mg per day and 2 mg per day with placebo. Patients were treated for 12 weeks (including one-week titration) and then were followed for 40 weeks post-treatment. Varenicline tablets was given in two divided doses daily. Each dose of varenicline tablets was given in two different regimens, with and without initial dose-titration, to explore the effect of different dosing regimens on tolerability. For the titrated groups, dosage was titrated up over the course of one week, with full dosage achieved starting with the second week of dosing. The titrated and nontitrated groups were pooled for efficacy analysis.
Forty-five percent of patients receiving varenicline tablets 1 mg per day (0.5 mg twice daily) and 51% of patients receiving 2 mg per day (1 mg twice daily) had CO-confirmed continuous abstinence during weeks 9 through 12 compared to 12% of patients in the placebo group (Figure 1). In addition, 31% of the 1 mg per day group and 31% of the 2 mg per day group were continuously abstinent from one week after TQD through the end of treatment as compared to 8% of the placebo group.
Study 3
This flexible-dosing study of 312 patients examined the effect of a patient-directed dosing strategy of varenicline tablets or placebo. After an initial one-week titration to a dose of 0.5 mg twice daily, patients could adjust their dosage as often as they wished between 0.5 mg once daily to 1 mg twice daily per day. Sixty-nine percent of patients titrated to the maximum allowable dose at any time during the study. For 44% of patients, the modal dose selected was 1 mg twice daily; for slightly over half of the study participants, the modal dose selected was 1 mg/day or less.
Of the patients treated with varenicline tablets, 40% had CO-confirmed continuous abstinence during weeks 9 through 12 compared to 12% in the placebo group. In addition, 29% of the varenicline tablets group were continuously abstinent from one week after TQD through the end of treatment as compared to 9% of the placebo group.
Study 4 and Study 5
These identical double-blind studies compared varenicline tablets 2 mg per day, bupropion sustained-release (SR) 150 mg twice daily, and placebo. Patients were treated for 12 weeks and then were followed for 40 weeks post-treatment. The varenicline tablets dosage of 1 mg twice daily was achieved using a titration of 0.5 mg once daily for the initial 3 days followed by 0.5 mg twice daily for the next 4 days. The bupropion SR dosage of 150 mg twice daily was achieved using a 3-day titration of 150 mg once daily. Study 4 enrolled 1022 patients and Study 5 enrolled 1023 patients. Patients inappropriate for bupropion treatment or patients who had previously used bupropion were excluded.
In Study 4, patients treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (44%) compared to patients treated with bupropion SR (30%) or placebo (17%). The bupropion SR quit rate was also superior to placebo. In addition, 29% of the varenicline tablets group were continuously abstinent from one week after TQD through the end of treatment as compared to 12% of the placebo group and 23% of the bupropion SR group.
Similarly in Study 5, patients treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (44%) compared to patients treated with bupropion SR (30%) or placebo (18%). The bupropion SR quit rate was also superior to placebo. In addition, 29% of the varenicline tablets group were continuously abstinent from one week after TQD through the end of treatment as compared to 11% of the placebo group and 21% of the bupropion SR group.
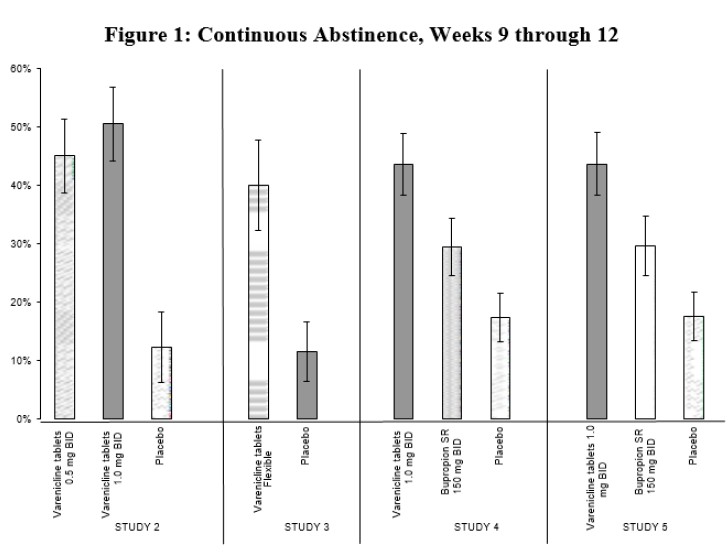
Table 7. Continuous Abstinence, Weeks 9 through 12 (95% confidence interval)
Varenicline tablets 0.5 mg BID | Varenicline tablets 1 mg BID | Varenicline tablets Flexible | Bupropion SR | Placebo |
Study 2 | 45% (39%, 51%) | 51% (44%, 57%) | 12% (6%, 18%) | |
Study 3 | 40% (32%, 48%) | 12% (7%, 17%) | ||
Study 4 | 44% (38%, 49%) | 30% (25%, 35%) | 17% (13%, 22%) | |
Study 5 | 44% (38%, 49%) | 30% (25%, 35%) | 18% (14%, 22%) |
BID = twice daily
Urge to Smoke
Based on responses to the Brief Questionnaire of Smoking Urges and the Minnesota Nicotine Withdrawal scale "urge to smoke" item, varenicline tablets reduced urge to smoke compared to placebo.
Long-Term Abstinence
Studies 1 through 5 included 40 weeks of post-treatment follow-up. In each study, varenicline tablets-treated patients were more likely to maintain abstinence throughout the follow-up period than were patients treated with placebo (Figure 2, Table 8).
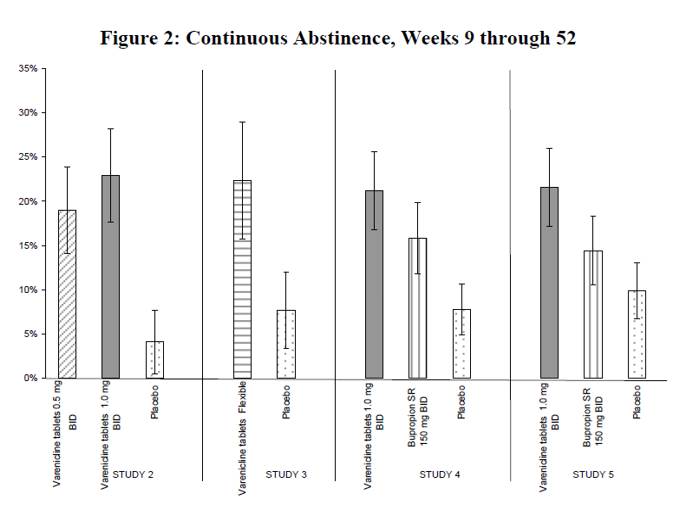
Table 8. Continuous Abstinence, Weeks 9 through 52 (95% confidence interval) Across Different Studies
Varenicline tablets 0.5 mg BID | Varenicline tablets 1 mg BID | Varenicline tablets Flexible | Bupropion SR | Placebo |
Study 2 | 19% (14%, 24%) | 23% (18%, 28%) | 4% (1%, 8%) | |
Study 3 | 22% (16%, 29%) | 8% (3%, 12%) | ||
Study 4 | 21% (17%, 26%) | 16% (12%, 20%) | 8% (5%, 11%) | |
Study 5 | 22% (17%, 26%) | 14% (11%, 18%) | 10% (7%, 13%) |
BID = twice daily
Study 6
This study assessed the effect of an additional 12 weeks of varenicline tablets therapy on the likelihood of long-term abstinence. Patients in this study (N=1927) were treated with open-label varenicline tablets 1 mg twice daily for 12 weeks. Patients who had stopped smoking for at least a week by Week 12 (N= 1210) were then randomized to double-blind treatment with varenicline tablets (1 mg twice daily) or placebo for an additional 12 weeks and then followed for 28 weeks post-treatment.
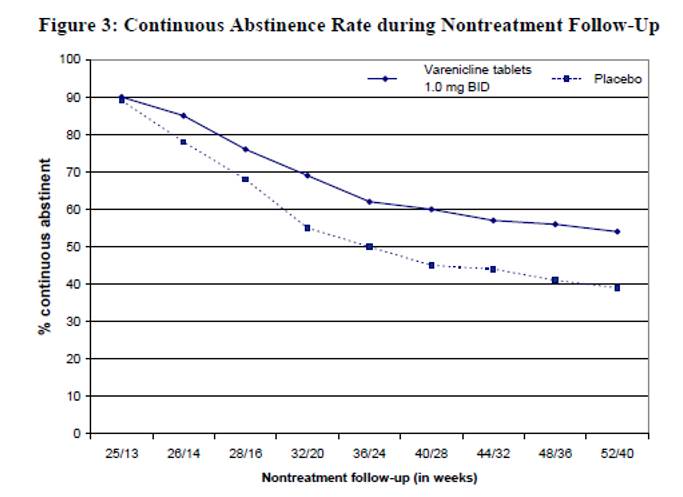
The continuous abstinence rate from Week 13 through Week 24 was higher for patients continuing treatment with varenicline tablets (70%) than for patients switching to placebo (50%). Superiority to placebo was also maintained during 28 weeks post-treatment follow-up (varenicline tablets 54% versus placebo 39%).
In Figure 3 below, the x-axis represents the study week for each observation, allowing a comparison of groups at similar times after discontinuation of varenicline tablets; post varenicline tablets follow-up begins at Week 13 for the placebo group and Week 25 for the varenicline tablets group. The y-axis represents the percentage of patients who had been abstinent for the last week of varenicline tablets treatment and remained abstinent at the given timepoint.
Alternative Instructions for Setting a Quit Date
Varenicline tablets was evaluated in a double-blind, placebo-controlled trial where patients were instructed to select a target quit date between Day 8 and Day 35 of treatment. Subjects were randomized 3:1 to varenicline tablets 1 mg twice daily (N=486) or placebo (N=165) for 12 weeks of treatment and followed for another 12 weeks posttreatment. Patients treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (54%) compared to patients treated with placebo (19%) and from weeks 9 through 24 (35%) compared to subjects treated with placebo (13%).
Gradual Approach to Quitting Smoking
Varenicline tablets was evaluated in a 52-week double-blind placebo-controlled study of 1,510 subjects who were not able or willing to quit smoking within four weeks, but were willing to gradually reduce their smoking over a 12 week period before quitting. Subjects were randomized to either varenicline tablets 1 mg twice daily (N=760) or placebo (N=750) for 24 weeks and followed up post-treatment through week 52. Subjects were instructed to reduce the number of cigarettes smoked by at least 50 percent by the end of the first four weeks of treatment, followed by a further 50 percent reduction from week four to week eight of treatment, with the goal of reaching complete abstinence by 12 weeks. After the initial 12-week reduction phase, subjects continued treatment for another 12 weeks. Subjects treated with varenicline tablets had a significantly higher Continuous Abstinence Rate compared with placebo at weeks 15 through 24 (32% vs. 7%) and weeks 15 through 52 (24% vs. 6%).
Re-Treatment Study
Varenicline tablets was evaluated in a double-blind, placebo-controlled trial of patients who had made a previous attempt to quit smoking with varenicline tablets, and either did not succeed in quitting or relapsed after treatment. Subjects were randomized 1:1 to varenicline tablets 1 mg twice daily (N=249) or placebo (N=245) for 12 weeks of treatment and followed for 40 weeks post-treatment. Patients included in this study had taken varenicline tablets for a smoking-cessation attempt in the past (for a total treatment duration of a minimum of two weeks), at least three months prior to study entry, and had been smoking for at least four weeks.
Patients treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (45%) compared to patients treated with placebo (12%) and from weeks 9 through 52 (20%) compared to subjects treated with placebo (3%).
Table 9. Continuous Abstinence (95% confidence interval), Re-Treatment Study
Weeks 9 through 12 | Weeks 9 through 52 | |||
Varenicline tablets 1 mg BID | Placebo | Varenicline tablets 1 mg BID | Placebo | |
Retreatment Study | 45% (39%, 51%) | 12% (8%, 16%) | 20% (15%, 25%) | 3% (1%, 5%) |
BID = twice daily
Subjects with Chronic Obstructive Pulmonary Disease
Varenicline tablets was evaluated in a randomized, double-blind, placebo-controlled study of subjects aged ≥ 35 years with mild-to-moderate COPD with post-bronchodilator FEV 1 /FVC <70% and FEV 1 ≥ 50% of predicted normal value. Subjects were randomized to varenicline tablets 1 mg twice daily (N=223) or placebo (N=237) for a treatment of 12 weeks and then were followed for 40 weeks post-treatment. Subjects treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (41%) compared to subjects treated with placebo (9%) and from week 9 through 52 (19%) compared to subjects treated with placebo (6%).
Table 10. Continuous Abstinence (95% confidence interval), Studies in Patients with Chronic Obstructive Pulmonary Disease (COPD)
Weeks 9 through 12 | Weeks 9 through 52 | |||
Varenicline tablets 1 mg BID | Placebo | Varenicline tablets 1 mg BID | Placebo | |
COPD Study | 41% (34%, 47%) | 9% (6%, 13%) | 19% (14%, 24%) | 6% (3%, 9%) |
BID = twice daily
Subjects with Cardiovascular Disease and Other Cardiovascular Analyses
Varenicline tablets was evaluated in a randomized, double-blind, placebo-controlled study of subjects aged 35 to 75 years with stable, documented cardiovascular disease (diagnoses other than, or in addition to, hypertension) that had been diagnosed for more than 2 months. Subjects were randomized to varenicline tablets 1 mg twice daily (N=353) or placebo (N=350) for a treatment period of 12 weeks and then were followed for 40 weeks post-treatment. Subjects treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (47%) compared to subjects treated with placebo (14%) and from week 9 through 52 (20%) compared to subjects treated with placebo (7%).
Table 11. Continuous Abstinence (95% confidence interval), Studies in Patients with Cardiovascular Disease (CVD)
Weeks 9 through 12 | Weeks 9 through 52 | |||
Varenicline tablets 1 mg BID | Placebo | Varenicline tablets 1 mg BID | Placebo | |
CVD Study | 47% (42%, 53%) | 14% (11%, 18%) | 20% (16%, 24%) | 7% (5%, 10%) |
BID = twice daily
In this study, all-cause and CV mortality was lower in patients treated with varenicline tablets, but certain nonfatal CV events occurred more frequently in patients treated with varenicline tablets than in patients treated with placebo [see Warnings and Precautions (5.5) , Adverse Reactions (6.1) ] . Table 12 below shows mortality and the incidence of selected nonfatal serious CV events occurring more frequently in the varenicline tablets arm compared to the placebo arm. These events were adjudicated by an independent blinded committee. Nonfatal serious CV events not listed occurred at the same incidence or more commonly in the placebo arm. Patients with more than one CV event of the same type are counted only once per row. Some of the patients requiring coronary revascularization underwent the procedure as part of management of nonfatal MI and hospitalization for angina.
Table 12. Mortality and Adjudicated Nonfatal Serious Cardiovascular Events in the Placebo-Controlled Varenicline Tablets Trial in Patients with Stable Cardiovascular Disease
Mortality and Cardiovascular Events | Varenicline tablets (N=353) n (%) | Placebo (N=350) n (%) |
Mortality (Cardiovascular and All-cause up to 52 weeks) | ||
Cardiovascular | 1 (0.3) | 2 (0.6) |
All-cause | 2 (0.6) | 5 (1.4) |
Nonfatal Cardiovascular Events (rate on varenicline tablets > Placebo) | ||
Up to 30 days after treatment | ||
Nonfatal myocardial infarction | 4 (1.1) | 1 (0.3) |
Nonfatal Stroke | 2 (0.6) | 0 (0) |
Beyond 30 days after treatment and up to 52 weeks | ||
Nonfatal myocardial infarction | 3 (0.8) | 2 (0.6) |
Need for coronary revascularization | 7 (2.0) | 2 (0.6) |
Hospitalization for angina pectoris | 6 (1.7) | 4 (1.1) |
Transient ischemia attack | 1 (0.3) | 0 (0) |
New diagnosis of peripheral vascular disease (PVD) or admission for a PVD procedure | 5 (1.4) | 2 (0.6) |
Following the CVD study, a meta-analysis of 15 clinical trials of ≥12 weeks treatment duration, including 7002 patients (4190 varenicline tablets, 2812 placebo), was conducted to systematically assess the CV safety of varenicline tablets. The study in patients with stable CV disease described above was included in the meta-analysis. There were lower rates of all-cause mortality (varenicline tablets 6 [0.14%]; placebo 7 [0.25%]) and CV mortality (varenicline tablets 2 [0.05%]; placebo 2 [0.07%]) in the varenicline tablets arms compared with the placebo arms in the meta-analysis.
The key CV safety analysis included occurrence and timing of a composite endpoint of Major Adverse Cardiovascular Events (MACE), defined as CV death, nonfatal MI, and nonfatal stroke. These events included in the endpoint were adjudicated by a blinded, independent committee. Overall, a small number of MACE occurred in the trials included in the meta-analysis, as described in Table 13. These events occurred primarily in patients with known CV disease.
Table 13. Number of MACE cases, Hazard Ratio and Rate Difference in a Meta-Analysis of 15 Clinical Trials Comparing Varenicline tablets to Placebo•
Varenicline tablets N=4190 | Placebo N=2812 | |
MACE cases, n (%) | 13 (0.31%) | 6 (0.21%) |
Patient-years of exposure | 1316 | 839 |
Hazard Ratio (95% CI) | ||
1.95 (0.79, 4.82) | ||
Rate Difference per 1,000 patient-years (95% CI) | ||
6.30 (-2.40, 15.10) | ||
•Includes MACE occurring up to 30 days post-treatment.
The meta-analysis showed that exposure to varenicline tablets resulted in a hazard ratio for MACE of 1.95 (95% confidence interval from 0.79 to 4.82) for patients up to 30 days after treatment; this is equivalent to an estimated increase of 6.3 MACE events per 1,000 patient-years of exposure. The meta-analysis showed higher rates of CV endpoints in patients on varenicline tablets relative to placebo across different time frames and pre-specified sensitivity analyses, including various study groupings and CV outcomes. Although these findings were not statistically significant they were consistent. Because the number of events was small overall, the power for finding a statistically significant difference in a signal of this magnitude is low.
Additionally, a cardiovascular endpoint analysis was added to the postmarketing neuropsychiatric safety outcome study along with a non-treatment extension, [see Warnings and Precautions (5.5) , Adverse Reactions (6.1) , Clinical Studies (14.10) ].
Subjects with Major Depressive Disorder
Varenicline tablets was evaluated in a randomized, double-blind, placebo-controlled study of subjects aged 18 to 75 years with major depressive disorder without psychotic features (DSM-IV TR). If on medication, subjects were to be on a stable antidepressant regimen for at least two months. If not on medication, subjects were to have experienced a major depressive episode in the past 2 years, which was successfully treated. Subjects were randomized to varenicline tablets 1 mg twice daily (N=256) or placebo (N=269) for a treatment of 12 weeks and then followed for 40 weeks post-treatment. Subjects treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 (36%) compared to subjects treated with placebo (16%) and from week 9 through 52 (20%) compared to subjects treated with placebo (10%).
Table 14. Continuous Abstinence (95% confidence interval), Study in Patients with Major Depressive Disorder (MDD)
Weeks 9 through 12 | Weeks 9 through 52 | |||
Varenicline tablets 1 mg BID | Placebo | Varenicline tablets 1 mg BID | Placebo | |
MDD Study | 36% (30%, 42%) | 16% (11%, 20%) | 20% (15%, 25%) | 10% (7%, 14%) |
BID = twice daily
Postmarketing Neuropsychiatric Safety Outcome Trial
Varenicline tablets was evaluated in a randomized, double-blind, active and placebo-controlled trial that included subjects without a history of psychiatric disorder (non-psychiatric cohort, N=3912) and with a history of psychiatric disorder (psychiatric cohort, N=4003). Subjects aged 18-75 years, smoking 10 or more cigarettes per day were randomized 1:1:1:1 to varenicline tablets 1 mg BID, bupropion SR 150 mg BID, NRT patch 21 mg/day with taper or placebo for a treatment period of 12 weeks; they were then followed for another 12 weeks post-treatment. [See Warnings and Precautions (5.1) ]
A composite safety endpoint intended to capture clinically significant neuropsychiatric (NPS) adverse events included the following NPS adverse events: anxiety, depression, feeling abnormal, hostility, agitation, aggression, delusions, hallucinations, homicidal ideation, mania, panic, paranoia, psychosis, irritability, suicidal ideation, suicidal behavior or completed suicide.
As shown in Table 15, the use of varenicline tablets, bupropion, and NRT in the non-psychiatric cohort was not associated with an increased risk of clinically significant NPS adverse events compared with placebo. Similarly, in the non-psychiatric cohort, the use of varenicline tablets was not associated with an increased risk of clinically significant NPS adverse events in the composite safety endpoint compared with bupropion or NRT.
Table 15. Number of Patients with Clinically Significant or Serious NPS Adverse Events by Treatment Group Among Patients without a History of Psychiatric Disorder
Varenicline tablets (N=975) n (%) | Bupropion (N=968) n (%) | NRT (N=987) n (%) | Placebo (N=982) n (%) | |
Clinically Significant NPS | 30 (3.1) | 34 (3.5) | 33 (3.3) | 40 (4.1) |
Serious NPS | 1 (0.1) | 5 (0.5) | 1 (0.1) | 4 (0.4) |
Psychiatric Hospitalizations | 1 (0.1) | 2 (0.2) | 0 (0.0) | 1 (0.1) |
As shown in Table 16, there were more clinically significant NPS adverse events reported in patients in the psychiatric cohort in each treatment group compared with the non-psychiatric cohort. The incidence of events in the composite endpoint was higher for each of the active treatments compared to placebo: Risk Differences (RDs) (95%CI) vs placebo were 2.7% (-0.05, 5.4) for varenicline tablets, 2.2% (-0.5, 4.9) for bupropion, and 0.4% (-2.2, 3.0) for NRT transdermal nicotine.
Table 16. Number of Patients with Clinically Significant or Serious NPS Adverse Events by Treatment Group Among Patients with a History of Psychiatric Disorder
Varenicline tablets N=1007) n (%) | Bupropion (N=1004) n (%) | NRT (N=995) n (%) | Placebo (N=997) n (%) | |
Clinically Significant NPS | 123 (12.2) | 118 (11.8) | 98 (9.8) | 95 (9.5) |
Serious NPS | 6 (0.6) | 8 (0.8) | 4 (0.4) | 6 (0.6) |
Psychiatric hospitalizations | 5 (0.5) | 8 (0.8) | 4 (0.4) | 2 (0.2) |
There was one completed suicide, which occurred during treatment in a patient treated with placebo in the non-psychiatric cohort. There were no completed suicides reported in the psychiatric cohort.
In both cohorts, subjects treated with varenicline tablets had a superior rate of CO-confirmed abstinence during weeks 9 through 12 and 9 through 24 compared to subjects treated with bupropion, nicotine patch and placebo.
Table 17 Continuous Abstinence (95% confidence interval), Study in Patients with or without a History of Psychiatric Disorder
Varenicline tablets 1 mg BID | Bupropion SR 150 mg BID | NRT 21 mg/day with taper | Placebo | |
Weeks 9 through 12 | ||||
Non- | 38% | 26% | 26% | 14% |
Psychiatric | (35%, 41%) | (23%, 29%) | (24%, 29%) | (12%, 16%) |
Cohort | ||||
Psychiatric | 29% | 19% | 20% | 11% |
Cohort | (26%, 32%) | (17%, 22%) | (18%, 23%) | (10%, 14%) |
Weeks 9 through 24 | ||||
Non- | 25% | 19% | 18% | 11% |
Psychiatric | (23%, 28%) | (16%, 21%) | (16%, 21%) | (9%, 13%) |
Cohort | ||||
Psychiatric | 18% | 14% | 13% | 8% |
Cohort | (16%, 21%) | (12%, 16%) | (11%, 15%) | (7%, 10%) |
BID = twice daily
Cardiovascular Outcome Analysis
To obtain another source of data regarding the CV risk of varenicline tablets, a cardiovascular endpoint analysis was added to the postmarketing neuropsychiatric safety outcome study along with a non-treatment extension. In the parent study (N=8027), subjects aged 18-75 years, smoking 10 or more cigarettes per day were randomized 1:1:1:1 to varenicline tablets 1 mg BID, bupropion SR 150 mg BID, nicotine replacement therapy (NRT) patch 21 mg/day or placebo for a treatment period of 12 weeks; they were then followed for another 12 weeks post-treatment. The extension study enrolled 4590 (57.2%) of the 8027 subjects who were randomized and treated in the parent study and followed them for additional 28 weeks. Of all treated subjects, 1743 (21.7%) had a medium CV risk and 640 (8.0%) had a high CV risk, as defined by Framingham score. Note that one site from the parent study was excluded in the assessment of CV safety and two sites were excluded in the assessment of neuropsychiatric safety.
The primary CV endpoint was the time to major adverse CV event (MACE), defined as CV death, nonfatal myocardial infarction or nonfatal stroke during treatment. Deaths and CV events were adjudicated by a blinded, independent committee. Table 18 below shows the incidence of MACE and Hazard Ratios compared to placebo for all randomized subjects exposed to at least 1 partial dose of study treatment in the parent study.
Table 18. The Incidence of MACE and Hazard Ratios in the Cardiovascular Safety Assessment Trial in Subjects without or with a History of Psychiatric Disorder
Varenicline tablets N=2006 | Bupropion N=1997 | NRT N=2017 | Placebo N=2007 | |
During treatment• | ||||
MACE, n [IR] | 1 [2.4] | 2 [4.9] | 1 [2.4] | 4 [9.8] |
Hazard Ratio (95% CI) vs. placebo | 0.24 (0.03, 2.18) | 0.49 (0.09, 2.69) | 0.24 (0.03, 2.18) | |
Through end of study•• | ||||
MACE, n [IR] | 3 [2.1] | 9 [6.3] | 6 [4.3] | 8 [5.7] |
Hazard Ratio (95% CI) vs. placebo | 0.36 (0.10, 1.36) | 1.09 (0.42, 2.83) | 0.74 (0.26, 2.13) | |
[IR] indicates incidence rate per 1000 person-years
•during treatment in the parent neuropsychiatric safety study
••either the end of the extension study or the end of parent neuropsychiatric safety study for those subjects not enrolled into the extension study
For this study, MACE+ was defined as any MACE or a new onset or worsening peripheral vascular disease (PVD) requiring intervention, a need for coronary revascularization, or hospitalization for unstable angina. Incidence rates of MACE+ and all-cause mortality for all randomized subjects exposed to at least 1 partial dose of study treatment in the parent study are shown for all treatment groups during treatment, and through end of study in the Table 19 below.
Table 19. The Incidence of MACE+ and All-Cause Death in the Cardiovascular Safety Assessment Trial in Subjects without or with a History of Psychiatric Disorder
Varenicline tablets N=2006 | Bupropion N=1997 | NRT N=2017 | Placebo N=2007 | |
During treatment• | ||||
MACE+, n [IR] | 5 [12.1] | 4 [9.9] | 2 [4.8] | 5 [12.2] |
All-cause deaths, n [IR] | 0 | 2 [4.9] | 0 | 2 [4.9] |
Through end of study•• | ||||
MACE+, n [IR] | 10 [6.9] | 15 [10.5] | 10 [7.1] | 12 [8.6] |
All-cause deaths, n [IR] | 2 [1.4] | 4 [2.8] | 3 [2.1] | 4 [2.9] |
[IR] indicates incidence rate per 1000 person-years
•during treatment in the parent neuropsychiatric safety study
••either the end of the extension study or the end of the parent neuropsychiatric safety study for those subjects not enrolled into the extension study
The number of subjects who experienced MACE, MACE+ and all-cause death was similar or lower among patients treated with varenicline tablets than patients treated with placebo. The number of events observed overall was too low to distinguish meaningful differences between the treatment arms.
HOW SUPPLIED/STORAGE AND HANDLING
Varenicline tablets are supplied for oral administration in two strengths: a 0.5 mg modified capsule shaped, white to off-white, film coated tablets debossed with 'L' on one side and '11' on other side and a 1 mg modified capsule shaped, light pink to pink color, film coated tablets debossed with 'L' on one side and '12' on other side.
Varenicline tablets are supplied in the following package configurations:
Description | NDC | |
Packs | Starting 4-week card: 0.5 mg x 11 tablets and 1 mg x 42 tablets | NDC 68462-895-04 |
Continuing 4-week card: 1 mg x 56 tablets | NDC 68462-894-04 | |
Starting Month Box: 0.5 mg x 11 tablets and 1 mg x 42 tablets | NDC 68462-895-04 | |
Continuing Month Box: 1 mg x 56 tablets | NDC 68462-894-04 | |
Bottles | 0.5 mg - bottle of 56 | NDC 68462-893-56 |
1 mg - bottle of 56 | NDC 68462-894-56 |
Store at 20º to 25ºC (68º to 77ºF); excursions permitted to 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature].
Dispense in a tight, light-resistant container as defined in the USP.
This package is child-resistant
Mechanism of Action
Varenicline binds with high affinity and selectivity at α4β2 neuronal nicotinic acetylcholine receptors. The efficacy of varenicline tablets in smoking cessation is believed to be the result of varenicline's activity at α4β2 sub-type of the nicotinic receptor where its binding produces agonist activity, while simultaneously preventing nicotine binding to these receptors.
Electrophysiology studies in vitro and neurochemical studies in vivo have shown that varenicline binds to α4β2 neuronal nicotinic acetylcholine receptors and stimulates receptor-mediated activity, but at a significantly lower level than nicotine. Varenicline blocks the ability of nicotine to activate α4β2 receptors and thus to stimulate the central nervous mesolimbic dopamine system, believed to be the neuronal mechanism underlying reinforcement and reward experienced upon smoking. Varenicline is highly selective and binds more potently to α4β2 receptors than to other common nicotinic receptors (>500-fold α3β4, >3,500-fold α7, >20,000-fold α1βγδ), or to nonnicotinic receptors and transporters (>2,000-fold). Varenicline also binds with moderate affinity (Ki = 350 nM) to the 5-HT3 receptor.