Get your patient on Yorvipath - Palopegteriparatide injection, Solution (Palopegteriparatide)
Yorvipath - Palopegteriparatide injection, Solution prescribing information
INDICATIONS AND USAGE
YORVIPATH is indicated for the treatment of hypoparathyroidism in adults.
Limitations of Use
- YORVIPATH was not studied for acute post-surgical hypoparathyroidism.
- YORVIPATH's titration scheme was only evaluated in adults who first achieved an albumin-corrected serum calcium of at least 7.8 mg/dL using calcium and active vitamin D treatment [see Dosage and Administration (2.3 , 2.4) and Clinical Studies (14) ] .
DOSAGE AND ADMINISTRATION
- Use only one injection to achieve the once daily recommended dosage. (2.1 )
- Maximum recommended YORVIPATH dosage is 30 mcg subcutaneously once daily. (2.1 )
- Individualize YORVIPATH dosage based on serum calcium. (2.1 )
- Refer to the Full Prescribing Information for complete dosage and administration information. (2 )
Overview of Dosage and Monitoring
- Use only one injection to achieve the once daily recommended dosage. Using two injections to achieve the recommended once daily dosage increases the risk of unintended changes in serum calcium levels, including hypocalcemia and hypercalcemia. [see Dosage and Administration (2.4 , 2.6) and Warnings and Precautions (5.1) ] .
- The maximum recommended dosage is 30 mcg subcutaneously once daily. If an adequate response is not achieved with a maximum YORVIPATH dosage of 30 mcg, consider adding or restarting calcium and/or active vitamin D therapy and/or seek other treatment options [see Warnings and Precautions (5.1) ] .
- YORVIPATH's once daily subcutaneous dosage is individualized. The recommended starting dosage is 18 mcg once daily and is titrated in 3 mcg increments or decrements with the goal of maintaining serum calcium within the normal range without the need for active vitamin D (e.g., calcitriol) or therapeutic calcium doses (elemental calcium >600 mg/day). Calcium supplementation sufficient to meet daily dietary requirements may be continued.
- Advise patients to monitor daily for clinical signs and symptoms of hypocalcemia or hypercalcemia.
- Measure serum calcium 7 to 10 days after the first YORVIPATH dose and after any dose change in YORVIPATH, active vitamin D, or calcium supplements, and monitor for clinical signs and symptoms of hypocalcemia or hypercalcemia. Once the YORVIPATH maintenance dosage is achieved, measure serum calcium levels at a minimum every 4 to 6 weeks or as indicated for symptoms of hypocalcemia or hypercalcemia.
- Adjust YORVIPATH, active vitamin D, and/or calcium supplements per Figure 1. Some patients may require an increase in the YORVIPATH dose over time to maintain the same therapeutic effect [see Clinical Studies (14) ] .
- Refer to the Instructions for Use (IFU) for detailed instructions on the proper preparation and administration of YORVIPATH [see Dosage and Administration (2.6) ] .
Laboratory Testing Prior to Initiation of YORVIPATH
- Within two weeks before the first dose of YORVIPATH, confirm serum 25(OH) vitamin D is within the normal range and albumin-corrected serum calcium is ≥7.8 mg/dL.
Modification of Active Vitamin D and Calcium Supplements on Day of YORVIPATH Initiation or Up-titration
- On the day of initiation or up-titration of YORVIPATH, adjust the dose of active vitamin D and calcium supplements based on albumin-corrected serum calcium and current active vitamin D intake (Table 1).
| Albumin-Corrected Serum Calcium | Current Active Vitamin D (calcitriol) Intake | Adjust Active Vitamin D (calcitriol) Intake | Adjust Calcium Supplements |
|---|---|---|---|
| ≥8.3 mg/dL | >1 mcg/day | Reduce calcitriol dosage by ≥50% | Maintain current calcium dosage |
| ≥8.3 mg/dL | ≤1 mcg/day | Discontinue calcitriol | Maintain current calcium dosage |
| ≥7.8 to <8.3 mg/dL | Any amount | Reduce calcitriol dosage by ≥50% | Maintain current calcium dosage |
| ≥7.8 mg/dL | Not currently on active vitamin D | Not applicable | Reduce calcium daily dosage by at least 1500 mg or discontinue If calcium supplements are needed to meet dietary requirements, continuing dietary calcium supplements at elemental dosages ≤600 mg/day may be considered instead of discontinuing the calcium entirely. if current calcium daily dosage is ≤1500 mg/day |
Recommended Dosage, Titration Scheme, and Monitoring
- The recommended starting dosage of YORVIPATH is 18 mcg once daily. Dosage adjustments should be made in 3 mcg increments or decrements. Do not increase the YORVIPATH dosage more often than every 7 days. Do not decrease the YORVIPATH dosage more often than every 3 days.
- The recommended dosage range of YORVIPATH is 6 to 30 mcg once daily.
- Measure serum calcium within 7 to 10 days after the first dose and any dose change in YORVIPATH, active vitamin D, or calcium supplements, and monitor for clinical symptoms of hypocalcemia or hypercalcemia. Adjust YORVIPATH, active vitamin D, and/or calcium supplements per Figure 1.
- The maintenance dosage is individualized and should be the YORVIPATH dose that achieves serum calcium within the normal range, without the need for active vitamin D or therapeutic doses of calcium. Calcium supplementation sufficient to meet daily dietary requirements may be continued. Once the maintenance dosage is achieved, monitor for clinical signs and symptoms of hypocalcemia or hypercalcemia and measure serum calcium levels as indicated, and at a minimum every 4 to 6 weeks, as some patients may require further dose titration. If calcium levels remain low with the maximum recommended dosage of 30 mcg once daily, consider adding or restarting calcium and/or active vitamin D therapy and/or seek other treatment.
Titration Recommendations for Albumin-Corrected Serum Calcium Less Than 12 mg/dL
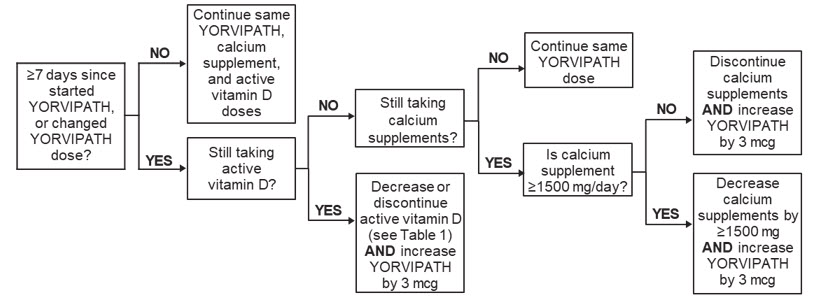
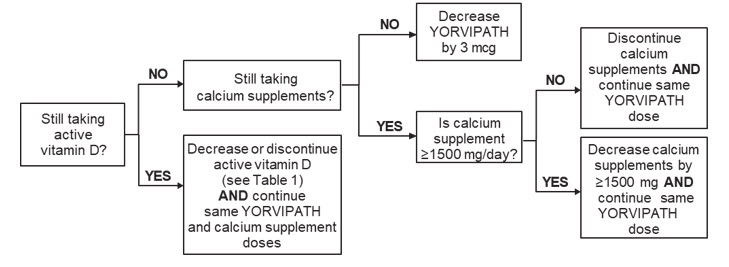
Figure 1 shows dosage titration recommendations for YORVIPATH, active vitamin D, and calcium in adults with specific albumin-corrected serum calcium ranges that are less than or equal to 12 mg/dL. The maximum recommended dosage of YORVIPATH is 30 mcg once daily [see Dosage and Administration (2.1) ] .
Figure 1: Titration of YORVIPATH, Active Vitamin D, and Calcium Supplements
Albumin-Corrected Serum Calcium <8.3 mg/dL:
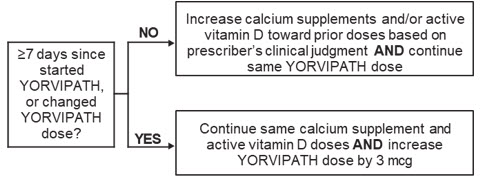
Albumin-Corrected Serum Calcium 8.3 to 10.6 mg/dL:
Albumin-Corrected Serum Calcium 10.7 to 11.9 mg/dL:
Titration Recommendations for Albumin-Corrected Serum Calcium 12 mg/dL or Greater
Withhold YORVIPATH for 2 to 3 days and then recheck serum calcium. If albumin-corrected serum calcium remains ≥12 mg/dL, withhold YORVIPATH for an additional 2 to 3 days and then recheck serum calcium. Once the albumin-corrected serum calcium is <12 mg/dL, resume titration of YORVIPATH, active vitamin D, and calcium supplements per the applicable section of Figure 1 using the most recent serum calcium value.
Dose Delay, Interruption, or Discontinuation of YORVIPATH
Take YORVIPATH as soon as possible if a dose is missed by less than 12 hours. Skip the missed dose if the dose has been missed by more than 12 hours. Take the next dose as scheduled.
If YORVIPATH treatment is delayed or interrupted for 3 days or more, evaluate patients for signs and symptoms of hypocalcemia and consider measuring serum calcium. If indicated, resume treatment with, or increase the dose of, calcium supplements and active vitamin D. Resume YORVIPATH at the previously prescribed dose as soon as possible after an interruption then measure serum calcium within 7 to 10 days and adjust doses of YORVIPATH, active vitamin D, and/or calcium supplements per Figure 1 [see Dosage and Administration (2.4) ] .
Preparation of Pen and Administration Instructions
Patients and caregivers who will administer YORVIPATH should receive appropriate training by a healthcare professional prior to first use.
Follow the Instructions for Use to administer YORVIPATH using pen and needle:
- YORVIPATH must be refrigerated at 2°C to 8°C (36°F to 46°F) until first use.
- YORVIPATH should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. YORVIPATH is a clear, colorless solution. Do not use if solid particles appear or if the solution is cloudy or colored.
- When a pen is used for the first time, test pen flow.
- Click the needle straight onto the pen, then screw the needle onto the pen until secure.
- Administer YORVIPATH subcutaneously to the abdomen or front of the thigh. Rotate the injection site daily.
- YORVIPATH should be administered initially when the patient can sit or lie down because of the potential of orthostatic hypotension [see Warnings and Precautions (5.5) ].
DOSAGE FORMS AND STRENGTHS
Injection: Clear, colorless solution in single-patient-use prefilled pens in three presentations
Table 2 displays the YORVIPATH prefilled pen presentations, strengths, labeled doses, and deliverable dose ranges.
| Pen Type and Strength | Labeled Dose (mcg) | Range of Deliverable Dose Deliverable dose range at each labeled dose setting based on prefilled pen performance. Use only labeled dose for titration (refer to Figure 1). (Minimum – Maximum) (mcg) |
|---|---|---|
| Prefilled pen with blue push button (168 mcg/0.56 mL) | 6 | 4.5 - 7.5 |
| 9 | 7.5 - 10.5 | |
| 12 | 10.5 - 13.5 | |
| Prefilled pen with orange push button (294 mcg/0.98 mL) | 15 | 13.1 - 16.5 |
| 18 | 16.1 - 19.5 | |
| 21 | 19.1 - 22.5 | |
| Prefilled pen with burgundy push button (420 mcg/1.4 mL) | 24 | 21.6 - 25.5 |
| 27 | 24.6 - 28.5 | |
| 30 | 27.6 - 31.5 |
USE IN SPECIFIC POPULATIONS
Lactation : Monitor breastfed infants for symptoms of hypercalcemia or hypocalcemia. Consider monitoring serum calcium in the breastfed infant (8.2 ).
Pregnancy
Risk Summary
Available data from reports of pregnancies in the clinical trials from drug development are insufficient to identify a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. There are disease-associated risks to the mother and fetus related to hypocalcemia in pregnancy (see Clinical Considerations ). In animal reproduction studies, administration of palopegteriparatide to pregnant rats and rabbits during the period of organogenesis resulted in no significant adverse effects up to doses 16- and 13-fold, respectively, the maximum recommended human dose (MRHD), based on PTH(1-34) and active metabolite PTH(1-33) exposure by area under the curve (AUC) (see Data ).
The background risk of birth defects and miscarriages for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriages in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
If YORVIPATH is administered during pregnancy, or if a patient becomes pregnant while receiving YORVIPATH, healthcare providers should report YORVIPATH exposure by calling1-877-229-2184.
Clinical Considerations
Disease-Associated Maternal and Embryo/Fetal Risk
Maternal hypocalcemia can result in an increased rate of spontaneous abortion, premature and dysfunctional labor, and possibly preeclampsia. Infants born to mothers with hypocalcemia can have associated fetal and neonatal hyperparathyroidism, which may cause fetal and neonatal skeletal demineralization, subperiosteal bone resorption, osteitis fibrosa cystica, and neonatal seizures. Infants born to mothers with hypocalcemia should be monitored for signs of hypocalcemia or hypercalcemia, including neuromuscular irritability (e.g., myotonic jerks, seizures), apnea, cyanosis, and cardiac arrhythmias.
Data
Animal Data
In an embryo-fetal developmental toxicity study in rats, palopegteriparatide was administered subcutaneously during the period of organogenesis (gestation days (GD) 6 to 17) at doses of 2, 8, and 30 mcg/kg/day. In pregnant rats, there was no evidence of embryo-lethality, fetotoxicity, or fetal malformations up to the highest dose tested corresponding to 16-fold the MRHD, based on PTH(1-34) and active metabolite PTH(1-33) exposure by AUC.
In an embryo-fetal developmental toxicity study in rabbits, palopegteriparatide was administered subcutaneously to pregnant female rabbits during the period of organogenesis (GD 7 to 19) at doses of 1, 3, and 6 mcg/kg/day. There was no evidence of any palopegteriparatide-related embryo-lethality, fetotoxicity, or fetal malformations at any dose level up to 13-fold the MRHD, based on PTH(1-34) exposure by AUC.
Lactation
Risk Summary
There are no data available on the presence of palopegteriparatide or its metabolite in either human or animal milk, the effects on the breastfed infant, or the effects on milk production. Infants breastfed by females treated with YORVIPATH should be monitored for signs and symptoms of hypercalcemia or hypocalcemia. Monitoring of serum calcium in the infant should be considered.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for YORVIPATH and any potential adverse effects on the breastfed child from YORVIPATH or from the underlying sub-optimally treated maternal condition.
Pediatric Use
The safety and effectiveness of YORVIPATH have not been established in pediatric patients.
Geriatric Use
In Study 1, 8 of 61 (13%) YORVIPATH-treated subjects were 65 years of age or over compared to 2 of 21 (10%) subjects in the placebo group. Clinical studies of YORVIPATH did not include a sufficient number of subjects 65 years of age and older to determine whether they respond differently from younger adult subjects.
Renal Impairment
No dose adjustment is required in patients with mild, moderate, or severe renal impairment (estimated glomerular filtration rate ≥ 15 mL/min/1.73 m 2 ).
In a dedicated renal impairment study, patients with severe renal impairment (estimated glomerular filtration rate 15 to 30 mL/min/1.73 m 2 ) had no clinically significant difference in total PTH compared to subjects with normal renal function upon treatment with YORVIPATH [see Clinical Pharmacology (12.3) ] .
CONTRAINDICATIONS
YORVIPATH is contraindicated in patients with severe hypersensitivity to palopegteriparatide or to any of its excipients. Hypersensitivity reactions, including anaphylaxis, angioedema, and urticaria, have been observed with parathyroid hormone (PTH) analogs.
WARNINGS AND PRECAUTIONS
- Unintended Changes in Serum Calcium Levels Related to Number of Daily Injections : Use only one daily YORVIPATH injection. Using two YORVIPATH injections to achieve the recommended once daily dosage increases the variability of the total delivered dose. (5.1 )
- Serious Hypercalcemia and Hypocalcemia : Have occurred with YORVIPATH. Periodically measure serum calcium and monitor for signs and symptoms of hypercalcemia and hypocalcemia. (5.2 , 5.3 )
- Potential Risk of Osteosarcoma : YORVIPATH is not recommended in patients at increased risk of osteosarcoma. (5.4 )
- Orthostatic Hypotension : Has been reported with YORVIPATH. Monitor for signs and symptoms of orthostatic hypotension. (5.5 )
- Digoxin Toxicity : Concomitant use with digoxin may predispose to digitalis toxicity if hypercalcemia develops. With concomitant use, frequently measure serum calcium and digoxin levels, and monitor for signs and symptoms of digoxin toxicity. (5.6 , 7.1 )
Risk of Unintended Changes in Serum Calcium Levels Related to Number of Daily Injections and Total Delivered Dose
Use only one YORVIPATH injection to achieve the recommended once daily dosage. Using two YORVIPATH injections to achieve the recommended once daily dosage increases the variability of the total delivered dose, which can cause unintended changes in serum calcium levels, including hypercalcemia and hypocalcemia [see Dosage and Administration (2.1) and Warning and Precautions (5.2 , 5.3) ] .
Serious Hypercalcemia
Serious events of hypercalcemia requiring hospitalization have been reported with YORVIPATH. The risk is highest when starting or increasing the dose of YORVIPATH but may occur at any time. Measure serum calcium 7 to 10 days after any dose change or if there are signs or symptoms of hypercalcemia, and at a minimum of every 4 to 6 weeks once the maintenance dose is achieved. Treat hypercalcemia if needed. If albumin-corrected serum calcium is greater than 12 mg/dL, withhold YORVIPATH for at least 2-3 days [see Dosage and Administration (2.4) ]. For less serious hypercalcemia, adjust the dose of YORVIPATH, active vitamin D, and/or calcium supplements [see Dosage and Administration (2) , Adverse Reactions (6.1) ] .
Serious Hypocalcemia
Serious events of hypocalcemia have been observed with PTH products, including YORVIPATH. The risk is highest when YORVIPATH is abruptly discontinued, but may occur at any time, even in patients who have been on stable doses of YORVIPATH. Measure serum calcium 7 to 10 days after any dose change or if there are signs or symptoms of hypocalcemia, and at a minimum of every 4 to 6 weeks once the maintenance dosage is achieved. Treat hypocalcemia if needed, and adjust the dose of YORVIPATH, active vitamin D, and/or calcium supplements if hypocalcemia occurs [see Dosage and Administration (2.4) ] .
Potential Risk of Osteosarcoma
YORVIPATH is a PTH analog. An increased incidence of osteosarcoma (a malignant bone tumor) has been reported in male and female rats treated with PTH analogs, including teriparatide. Osteosarcoma occurrence in rats is dependent on teriparatide or PTH dose and treatment duration. Osteosarcoma has been reported in patients treated with teriparatide in the postmarketing setting; however, an increased risk of osteosarcoma has not been observed in observational studies in humans. There are limited data assessing the risk of osteosarcoma beyond 2 years of teriparatide use.
YORVIPATH is not recommended in patients who are at increased risk of osteosarcoma, such as patients with:
- Open epiphyses. YORVIPATH is not approved in pediatric patients [see Use in Specific Populations (8.4) ] .
- Metabolic bone diseases other than hypoparathyroidism, including Paget's disease of bone.
- Unexplained elevations of alkaline phosphatase.
- Bone metastases or a history of skeletal malignancies.
- History of external beam or implant radiation therapy involving the skeleton.
- Hereditary disorders predisposing to osteosarcoma.
Instruct patients to promptly report clinical symptoms (e.g., persistent localized pain) and signs (e.g., soft tissue mass tender to palpation) that could be consistent with osteosarcoma.
Orthostatic Hypotension
Orthostatic hypotension has been reported with YORVIPATH. Associated signs and symptoms may include decreased blood pressure, dizziness (including postural dizziness), palpitations, tachycardia, presyncope, or syncope. Such symptoms can be managed by dosing at bedtime, while reclining. YORVIPATH should be administered initially when the patient can sit or lie down due to the potential of orthostatic hypotension.
Risk of Digoxin Toxicity With Concomitant Use of Digitalis Compounds
YORVIPATH increases serum calcium, and therefore, concomitant use with digoxin (which has a narrow therapeutic index) may predispose patients to digitalis toxicity if hypercalcemia develops. Digoxin efficacy may be reduced if hypocalcemia is present. When YORVIPATH is used concomitantly with digoxin, measure serum calcium and digoxin levels routinely, and monitor for signs and symptoms of digoxin toxicity. Refer to the digoxin prescribing information for dose adjustments, if needed [see Drug Interactions (7.1) ] .
ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Risk of Unintended Changes in Serum Calcium Levels Related to Number of Daily Injections and Total Delivered Dose [see Warnings and Precautions (5.1) ]
- Serious Hypercalcemia [see Warnings and Precautions (5.2) ]
- Serious Hypocalcemia [see Warnings and Precautions (5.3) ]
- Potential Risk of Osteosarcoma [see Warnings and Precautions (5.4) ]
- Orthostatic Hypotension [see Warnings and Precautions (5.5) ]
- Risk of Digoxin Toxicity with Concomitant Use of Digitalis Compounds [see Warnings and Precautions (5.6) ]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The phase 3 trial included 82 subjects with hypoparathyroidism with a median YORVIPATH treatment duration of 182 days (Study 1) [see Clinical Studies (14) ] .
Adverse reactions associated with YORVIPATH in Study 1 during the 26-week blinded period (incidence ≥5% and occurring ≥2% more frequently than placebo) are shown in Table 3.
| Adverse Reaction | YORVIPATH N=61 n (%) | Placebo N=21 n (%) |
|---|---|---|
| Abbreviations: N, total number of subjects in the treatment arm; n, number of subjects with the adverse reaction; %, percent of subjects with the adverse reaction. | ||
| Injection site reactions Injection site reactions includes the preferred terms injection site bruising, injection site erythema, injection site rash, and injection site reaction. | 24 (39) | 1 (5) |
| Vasodilatory signs and symptoms Vasodilatory signs and symptoms includes the preferred terms blood pressure orthostatic decreased, dizziness, dizziness postural, orthostatic hypotension, palpitations, postural orthostatic tachycardia syndrome, presyncope, syncope, and vertigo. | 17 (28) | 0 |
| Headache | 13 (21) | 2 (10) |
| Diarrhea | 6 (10) | 1 (5) |
| Back pain Back pain includes the preferred terms back pain, flank pain, and spinal pain. | 5 (8) | 0 |
| Hypercalcemia | 5 (8) | 0 |
| Oropharyngeal pain | 4 (7) | 0 |
Description of Selected Adverse Reactions
Hypercalcemia
Table 4 summarizes the number of subjects who had at least one serum calcium measurement greater than the upper limit of the reference range at a post-baseline visit in Study 1. The incidence of hypercalcemia was greater in subjects treated with YORVIPATH.
Symptomatic hypercalcemia was reported in 8% of subjects treated with YORVIPATH, and all occurred within the first 3 months after initiation of YORVIPATH.
| YORVIPATH N=61 | Placebo N=21 | |
|---|---|---|
| Abbreviations: N, total number of subjects in the treatment arm; n, number of subjects meeting criteria. | ||
| Albumin-Corrected Serum Calcium >10.6 mg/dL, n (%) Subjects meeting albumin-corrected serum calcium >10.6 mg/dL criterion includes subjects meeting albumin-corrected serum calcium >12 mg/dL criterion. | 33 (54.1) | 2 (9.5) |
| Albumin-Corrected Serum Calcium >12 mg/dL, n (%) | 8 (13.1) | 0 (0) |
DRUG INTERACTIONS
Drugs Known to Affect Calcium : When used concomitantly with YORVIPATH, measure serum calcium levels more frequently. (7.2 )
Drugs Affected by Serum Calcium
Digoxin
YORVIPATH increases serum calcium, therefore, concomitant use with digoxin (which has a narrow therapeutic index) may predispose patients to digitalis toxicity if hypercalcemia develops. Digoxin efficacy may be reduced if hypocalcemia is present. When YORVIPATH is used concomitantly with digoxin, measure serum calcium and digoxin levels, and monitor for signs and symptoms of digoxin toxicity. Adjustment of the digoxin and/or YORVIPATH dose may be needed.
Drugs Known to Affect Serum Calcium
Drugs that affect serum calcium may alter the therapeutic response to YORVIPATH. Measure serum calcium more frequently when YORVIPATH is used concomitantly with these drugs, particularly after these drugs are initiated, discontinued, or dose-adjusted.
DESCRIPTION
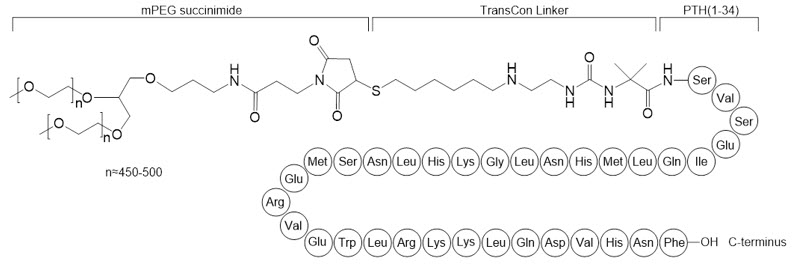
YORVIPATH (palopegteriparatide injection) is a parathyroid hormone analog (PTH(1-34)). Palopegteriparatide is a prodrug of teriparatide (PTH(1-34)) consisting of PTH(1-34) transiently conjugated to an inert carrier via a proprietary TransCon Linker. PTH(1-34) is identical to the 34 N-terminal amino acids (the biologically active region) of the 84-amino acid human parathyroid hormone. The carrier is a branched 40 kDa (2×20 kDa) methoxypolyethylene glycol (mPEG) moiety. The average molecular weight of palopegteriparatide is approximately 47.4 kDa.
The structure of palopegteriparatide drug substance is shown in Figure 2. The theoretical molecular formula is C 209 H 340 N 60 O 59 S 3 + 2 × (C 2 H 4 O) n , where n is between approximately 450 and 500.
Figure 2: Structure of Palopegteriparatide
YORVIPATH is a sterile, clear, and colorless solution in a glass cartridge which is pre-assembled in a single-patient-use prefilled pen for subcutaneous administration. The prefilled pen is co-packaged with disposable needles to administer 14 doses of YORVIPATH. YORVIPATH is available in three presentations containing 0.56 mL, 0.98 mL, or 1.4 mL of YORVIPATH solution, and each pen presentation can deliver one of three distinct doses for 14 days of therapy.
Each mL of YORVIPATH solution contains 3456 mcg of palopegteriparatide, equivalent to 300 mcg of teriparatide (PTH(1-34)), and the following inactive ingredients: 41.7 mg mannitol, 2.5 mg metacresol, 0.13 mg sodium hydroxide, 1.18 mg succinic acid, and water for injection. Hydrochloric acid and/or sodium hydroxide may be added to adjust the pH. YORVIPATH has a pH of 3.7 to 4.3.
Each pen of 0.56 mL contains 168 mcg teriparatide equivalent to 1935 mcg palopegteriparatide.
Each pen of 0.98 mL contains 294 mcg teriparatide equivalent to 3387 mcg palopegteriparatide.
Each pen of 1.4 mL contains 420 mcg teriparatide equivalent to 4838 mcg palopegteriparatide.
CLINICAL PHARMACOLOGY
Mechanism of Action
At physiological conditions, palopegteriparatide releases PTH(1-34) to maintain a continuous systemic exposure. Endogenous PTH maintains extracellular calcium and phosphate homeostasis by increasing serum calcium and decreasing serum phosphate. These effects are mediated by stimulating bone turnover to mobilize calcium and phosphate from bone, promoting renal calcium reabsorption and phosphate excretion, and facilitating active vitamin D synthesis, in turn increasing intestinal absorption of calcium and phosphate. Similar to endogenous PTH, PTH(1-34) released from palopegteriparatide exerts these effects through its main receptor, parathyroid hormone 1 receptor (PTH1R), which is highly expressed on osteoblasts, osteocytes, renal tubular cells, and in several other tissues.
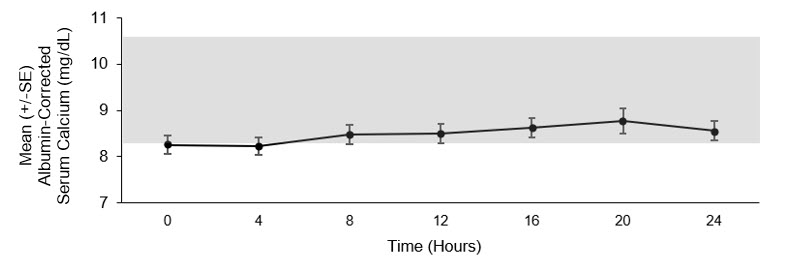
Pharmacodynamics
Serum PTH(1-34) and serum calcium concentrations increased in a dose-related manner when YORVIPATH was administered to healthy volunteers. Exposure-response is not established in subjects with hypoparathyroidism.
Mean steady state concentration-time profile of albumin-corrected serum calcium concentrations over 24 hours following administration of YORVIPATH is presented in Figure 3.
| Figure 3: Mean Steady-State Albumin-Corrected Serum Calcium Concentrations Following Subcutaneous Administration of YORVIPATH Mean dose (range): 22.3 (12-33) mcg/day, n=7. in Subjects with Hypoparathyroidism |
|---|
| The normal range for albumin-corrected serum calcium is 8.3 to 10.6 mg/dL. |
|
Pharmacokinetics
YORVIPATH is a prodrug that releases PTH(1-34) via autocleavage of the TransCon linker.
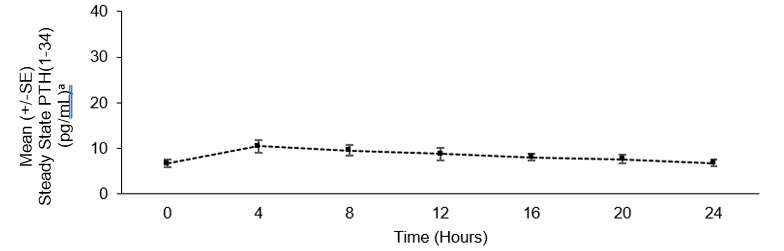
PTH C max and AUC increased proportionally over a YORVIPATH dosage range of 12 to 24 mcg/day. PTH steady state is achieved after administration of YORVIPATH for 7 days.
Mean steady state concentration-time profile of PTH(1-34) over 24 hours following administration of YORVIPATH is presented in Figure 4. At steady state, administration of YORVIPATH resulted in continuous exposure to released PTH throughout the 24-hour dosing period.
| Figure 4: Mean Steady State PTH(1-34) Following Subcutaneous Administration of YORVIPATH Mean dose (range): 22.3 (12-33) mcg/day, n=7. in Subjects with Hypoparathyroidism |
|---|
| a PTH(1-34) concentrations includes PTH(1-34) and active metabolite PTH(1-33). |
|
Absorption
The median (range) time to reach maximum concentrations (T max ) of PTH is 4 (4 to 8) hours.
Distribution
The estimated apparent volume of distribution (CV%) of palopegteriparatide is 4.8 (50) L. A similar distribution pattern as observed for endogenous PTH is expected for PTH released from palopegteriparatide.
Elimination
The apparent half-life of PTH released from palopegteriparatide is approximately 60 hours. The estimated clearance (CV%) of palopegteriparatide at steady state is 0.58 (52) L/day.
Metabolism
Released PTH includes PTH(1-34) and the active metabolite PTH(1-33). PTH(1-33) and PTH(1-34) have comparable affinity to and activation of PTH1R.
Specific Populations
There are no clinically significant differences in the pharmacokinetics of palopegteriparatide based on age, sex, or body weight. The data for race and ethnicity did not show any trends indicating differences, but the available data are too limited to make definitive conclusions.
Patients with Renal Impairment
A dedicated renal impairment study showed that mild, moderate, and severe renal impairment did not have a clinically significant impact on systemic exposure of total PTH following a single 50 mcg subcutaneous dose of palopegteriparatide. No studies were conducted in subjects with hypoparathyroidism who have severe renal impairment.
Patients with Hepatic Impairment
No dedicated hepatic impairment study was conducted. Mild and moderate hepatic impairment is not expected to have a clinically significant impact on the pharmacokinetics of palopegteriparatide.
Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the studies described below with the incidence of anti-drug antibodies in other studies, including those of YORVIPATH or other teriparatide products.
Mean duration of exposure to YORVIPATH in clinical studies was 850 days. Of patients with post-baseline assessments, 0.7% (1 of 139 YORVIPATH-treated patients) had low titer, non-neutralizing antibodies towards PTH and 5% (7 of 139 YORVIPATH-treated patients) had low titer treatment-emergent antibodies against PEG. Three of 139 YORVIPATH-treated patients (2.2%) had pre-existing PEG antibodies that had a transient impact on the pharmacokinetics of palopegteriparatide and serum calcium, however, therapeutic effectiveness was maintained by dose adjustment of YORVIPATH using the trial titration algorithm.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies to address the carcinogenic potential of palopegteriparatide have not been conducted.
Palopegteriparatide was not genotoxic in an in vitro bacterial reverse-mutation assay (Ames test), an in vitro human lymphocyte chromosome-aberration assay, and an in vivo rat bone-marrow micronucleus assay.
In fertility studies, palopegteriparatide was administered by subcutaneous injection at 2, 6, and 20 mcg/kg/day. Palopegteriparatide did not impair fertility in male and female rats up to the highest tested dose, which is 7-fold and 11-fold the MRHD, respectively, based on PTH(1-34) and active metabolite PTH(1-33) exposure by AUC.
Animal Toxicology and/or Pharmacology
In a 26-week rat study, daily subcutaneous administration of palopegteriparatide resulted in bone turnover imbalances in healthy euparathyroid rats. The bone effects tended towards a net catabolic effect (bone resorption) as evidenced by a decrease in proximal tibial trabecular bone volume and bone mineral content (BMC) in both sexes treated at the low dose of 5 mcg/kg/day (5-fold the MRHD, based on PTH(1-34) and active metabolite PTH(1-33) exposure by AUC) and in females treated at 10 mcg/kg/day (9-fold the MRHD, based on PTH(1-34) and PTH(1-33) exposure by AUC). A net anabolic bone effect (bone formation) including histologic increases in bone at several skeletal sites accompanied by increased osteoblast cellularity and increases in proximal tibia trabecular bone volume and BMC were observed in males at 10 mcg/kg/day (10-fold the MRHD, based on PTH(1-34) and PTH(1-33) exposure by AUC) and in both sexes treated at the high dose of 20 mcg/kg/day (19-fold the MRHD, based on PTH(1-34) and PTH(1-33) exposure by AUC). In a 4-week study in hypoparathyroid female rats, daily subcutaneous administration of palopegteriparatide at 5 and 10 mcg/kg/day (5- to 9-fold the MRHD, based on PTH(1-34) and PTH(1-33) exposure by AUC) resulted in a net catabolic bone effect as bone resorption (e.g., high urinary C-telopeptide of type 1 collagen, decreased tibial trabecular bone volume, increase in osteoclast surface, and endocortical eroded surface) appeared to exceed bone formation.
CLINICAL STUDIES
Treatment of Adults With Hypoparathyroidism
The effectiveness and safety of YORVIPATH in adults with hypoparathyroidism were evaluated in a 26-week, randomized, double-blind, placebo-controlled, phase 3 study (Study 1 [NCT04701203]).
Study 1 was conducted in 82 subjects with hypoparathyroidism. Prior to randomization, all subjects underwent an approximate 4-week screening period in which calcium and active vitamin D supplements were adjusted to achieve an albumin-corrected serum calcium concentration between 7.8 and 10.6 mg/dL, a magnesium concentration ≥1.3 mg/dL and below the upper limit of the reference range, and a 25(OH) vitamin D concentration between 20 to 80 ng/mL. During the double-blind period, subjects were randomized to either YORVIPATH (N = 61) or placebo (N= 21), at a starting dose of 18 mcg/day, co-administered with conventional therapy (calcium and active vitamin D). Randomization was stratified by etiology of hypoparathyroidism (postsurgical vs. all other causes). Study drug and conventional therapy were subsequently titrated according to the albumin-corrected serum calcium levels [see Dosage and Administration (2.3 , 2.4) ] .
The mean age at enrollment was 49 years (range: 19 to 78 years), 78% were female, and 93% were Caucasian. Eighty-five percent (85%) of subjects had hypoparathyroidism acquired from neck surgery. Of the subjects with other etiologies of hypoparathyroidism, 7 (8.5%) subjects had idiopathic disease, 2 had autoimmune polyglandular syndrome type 1 (APS-1), 1 had autosomal dominant hypocalcemia type 1 (ADH1, CaSR mutation), 1 had DiGeorge Syndrome, and 1 had hypoparathyroidism, sensorineural deafness and renal dysplasia (HDR) syndrome ( GATA3 mutation). At baseline, the median duration of hypoparathyroidism was 8.5 years (range 1 to 56 years). Baseline mean albumin-corrected serum calcium was 8.8 mg/dL and 8.6 mg/dL and mean 24-hour urine calcium was 392 mg/day and 329 mg/day for YORVIPATH and placebo, respectively. The mean baseline dose of elemental calcium was 1839 mg/day, and the mean baseline doses of active vitamin D were 0.75 mcg/day in calcitriol-treated subjects (n=70), and 2.3 mcg/day in alfacalcidol-treated subjects (n=12).
Efficacy Assessment and Results
Efficacy was assessed based on the proportion of subjects who achieved all of the following at Week 26:
- Albumin-corrected serum calcium in the normal range (8.3 to 10.6 mg/dL),
- Independence from conventional therapy (defined as requiring no active vitamin D and ≤600 mg/day of calcium supplementation, including no use of pro re nata [PRN] doses) since Week 22,
- No increase in the study drug dose since Week 22,
- No missing active vitamin D and calcium data since Week 22, and
- Study drug dose of 30 mcg or less once daily during the 26-week treatment period
In the YORVIPATH group, 68.9% (42/61) of subjects met the efficacy endpoint at Week 26 compared with 4.8% (1/21) of subjects in the placebo group. The treatment difference was 64.2% (95% confidence interval: 49.5%, 78.8%) (Table 5).
| YORVIPATH (N=61) | Placebo (N=21) | Response Rate Difference (95% CI) | |
|---|---|---|---|
| Abbreviations: CI: confidence interval; NA: not applicable; PRN: pro re nata. | |||
| Overall Response at Week 26 | 42 (68.9%) | 1 (4.8%) | 64.2% (49.5%, 78.8%) |
| Response for each component | |||
| Normal albumin-corrected serum calcium Normal range for albumin-corrected serum calcium was 8.3 to 10.6 mg/dL. | 49 (80.3%) | 10 (47.6%) | 32.7% (9.2%, 56.3%) |
| Independence from active vitamin D No daily standing doses of active vitamin D, no PRN doses, and no missing active vitamin D data within 4 weeks prior to Week 26 visit. | 58 (95.1%) | 5 (23.8%) | 71.3% (52.5%, 90.2%) |
| Independence from therapeutic dose of calcium Average daily standing dose of elemental calcium ≤600 mg, no PRN doses, and no missing calcium data within 4 weeks prior to Week 26 visit. | 53 (86.9%) | 1 (4.8%) | 82.2% (70.0%, 94.4%) |
| No increase in study drug dose since Week 22 No increase in study drug dose within 4 weeks prior to Week 26 visit. | 57 (93.4%) | 12 (57.1%) | 36.4% (14.2%, 58.5%) |
| Study drug dose ≤30 mcg/day up to Week 26 Subjects who received more than 30 mcg/day at any timepoint during the 26-week treatment period were considered as non-responders for the efficacy endpoint. | 56 (91.8%) | NA | NA |
The proportion of subjects randomized to YORVIPATH who met the efficacy endpoint decreased over time as follows: 68.9% (42/61) at Week 26 and 39.3% (24/61) at both Week 52 and Week 78 during the open-label extension period. Allowing for dose up-titration, the proportion of subjects who were able to maintain normocalcemia and independence from active vitamin D and therapeutic dose of calcium was 64% (39/61) at Week 52 and 66% (40/61) at Week 78.
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
YORVIPATH is available in a prefilled, disposable, 14-dose pen-injector (Table 6). Each pen contains a clear and colorless solution of 3456 mcg/mL of palopegteriparatide equivalent to 300 mcg/mL of teriparatide. Each pack contains 2 prefilled pens and 28 needles for 28 injections (plus two spare needles).
| Prefilled Pen Presentation | Labeled Doses | Content of Pack | NDC |
|---|---|---|---|
| YORVIPATH (168 mcg/0.56 mL) identified by blue push button | 6, 9, and 12 mcg | 2 prefilled pens 30 needles | 73362-100-01 |
| YORVIPATH (294 mcg/0.98 mL) identified by orange push button | 15, 18, and 21 mcg | 2 prefilled pens 30 needles | 73362-101-01 |
| YORVIPATH (420 mcg/1.4 mL) identified by burgundy push button | 24, 27, and 30 mcg | 2 prefilled pens 30 needles | 73362-102-01 |
Storage and Handling
Do not freeze. Store away from heat. Keep YORVIPATH in the packaging to protect from light.
Until first use, store YORVIPATH in the refrigerator between 2°C to 8°C (36°F to 46°F).
After first use, store YORVIPATH for 14 days at room temperature below 30°C (86°F). After each use, remove the needle and put the pen cap on to protect from light. Discard the prefilled pen 14 days after first use.
| Label | Content |
FRONT  | INSTRUCTIONS FOR USE Yorvipath ® (palopegteriparatide) injection, for subcutaneous use For 6, 9 or 12 mcg doses only This Instructions for Use contains information on how to inject YORVIPATH 168 mcg/0.56 mL (300 mcg/mL) prefilled pen for 6, 9 or 12 mcg doses only ascendis pharma |
Back  | Additional information If you need help, please ask your health care provider or nurse for advice or contact the Ascendis Pharma Helpline: Ascendis Pharma Helpline: Toll-free telephone number: 1-844-442-7236 Ascendis Pharma Bone Diseases A/S Tuborg Boulevard 12 DK-2900 Hellerup Denmark ascendis pharma |
Panel 1 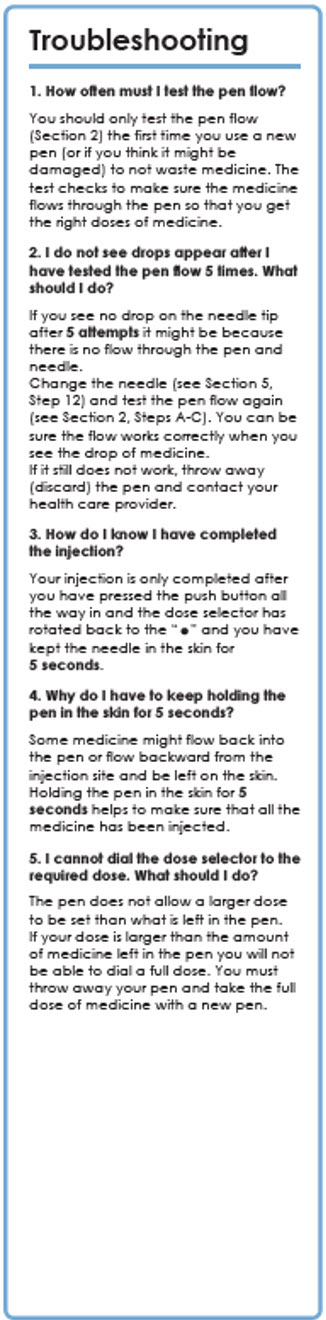 | 1. How often must I test the pen flow? You should only test the pen flow (Section 2) the first time you use a new pen (or if you think it might be damaged) to not waste medicine. The test checks to make sure the medicine flows through the pen so that you get the right doses of medicine. 2. I do not see drops appear after I have tested the pen flow 5 times. What should I do? If you see no drop on the needle tip after 5 attempts it might be because there is no flow through the pen and needle. Change the needle (see Section 5, Step 12 ) and test the pen flow again (see Section 2, Steps A-C ). You can be sure the flow works correctly when you see the drop of medicine. If it still does not work, throw away (discard) the pen and contact your health care provider. 3. How do I know I have completed the injection? Your injection is only completed after you have pressed the push button all the way in and the dose selector has rotated back to the "•" and you have kept the needle in the skin for 5 seconds . 4. Why do I have to keep holding the pen in the skin for 5 seconds? Some medicine might flow back into the pen or flow backward from the injection site and be left on the skin. Holding the pen in the skin for 5 seconds helps to make sure that all the medicine has been injected. 5. I cannot dial the dose selector to the required dose. What should I do? The pen does not allow a larger dose to be set than what is left in the pen. If your dose is larger than the amount of medicine left in the pen you will not be able to dial a full dose. You must throw away your pen and take the full dose of medicine with a new pen. |
Panel 2 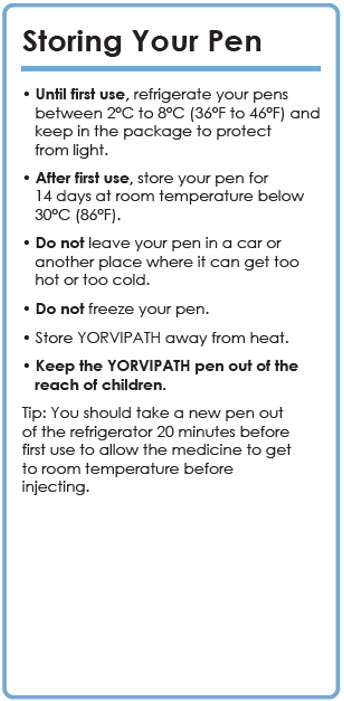 |
|
Panel 3 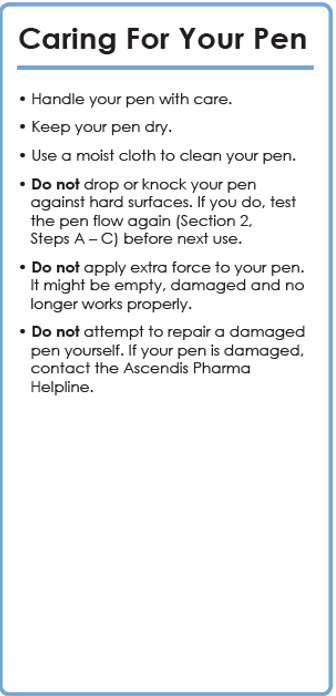 | Caring For Your Pen
|
Panel 4 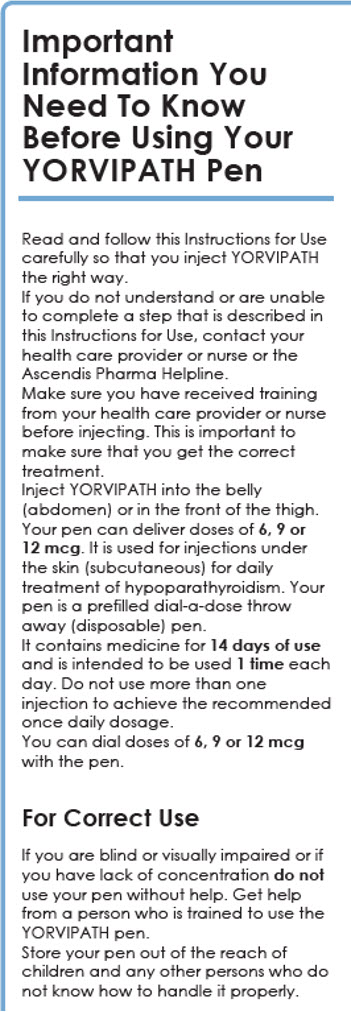 | Important Information You Need To Know Before Using Your YORVIPATH Pen Read and follow this Instructions for Use carefully so that you inject YORVIPATH the right way. If you do not understand or are unable to complete a step that is described in this Instructions for Use, contact your health care provider or nurse or the Ascendis Pharma Helpline. Make sure you have received training from your health care provider or nurse before injecting. This is important to make sure that you get the correct treatment. Inject YORVIPATH into the belly (abdomen) or in the front of the thigh. Your pen can deliver doses of 6, 9 or 12 mcg . It is used for injections under the skin (subcutaneous) for daily treatment of hypoparathyroidism. Your pen is a prefilled dial-a-dose throw away (disposable) pen. It contains medicine for 14 days of use and is intended to be used 1 time each day. Do not use more than one injection to achieve the recommended once daily dosage. You can dial doses of 6, 9 or 12 mcg with the pen. For Correct Use If you are blind or visually impaired or if you have lack of concentration do not use your pen without help. Get help from a person who is trained to use the YORVIPATH pen. Store your pen out of the reach of children and any other persons who do not know how to handle it properly. |
Panel 5 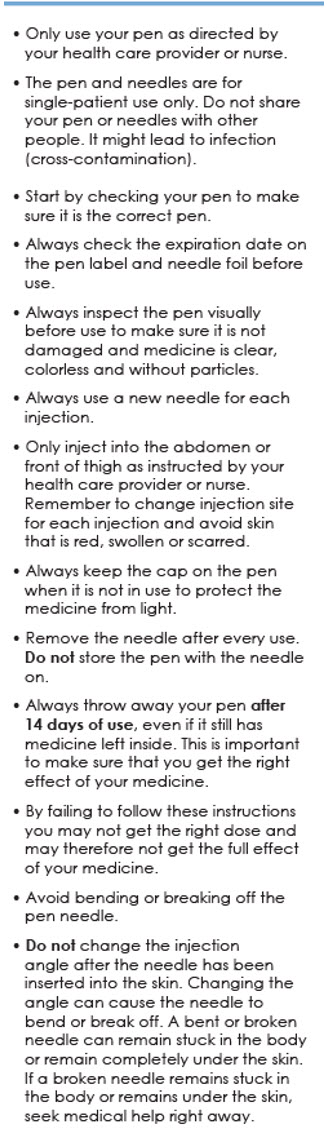 |
|
Panel 6 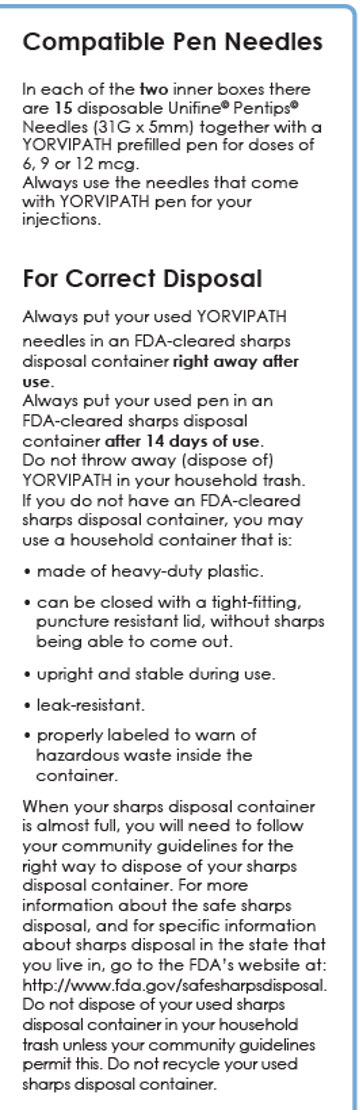 | Compatible Pen Needles In each of the two inner boxes there are 15 disposable Unifine© Pentips© Needles (31G × 5mm) together with a YORVIPATH prefilled pen for doses of 6, 9 or 12 mcg. Always use the needles that come with YORVIPATH pen for your injections. For Correct Disposal Always put your used YORVIPATH needles in an FDA-cleared sharps disposal container right away after use . Always put your used pen in an FDA-cleared sharps disposal container after 14 days of use . Do not throw away (dispose of) YORVIPATH in your household trash. If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
|
Panel 7 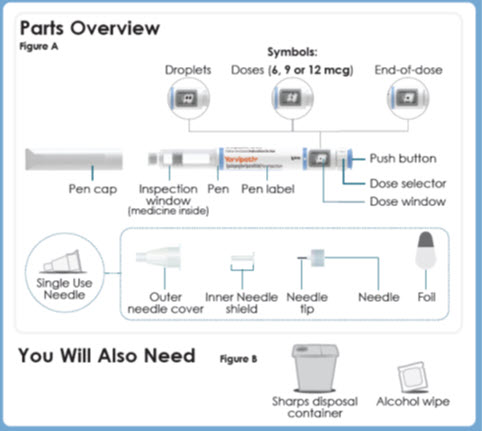 | Parts Overview Figure A Symbols: -Droplets -Doses ( 6, 9 or 12 mcg ) -End-of-dose -Pen cap -Inspection window (medicine inside) -Pen -Pen label -Push button -Dose selector -Dose window -Single Use Needle -Outer needle cover -Inner Needle shield -Needle tip -Needle -Foil You Will Also Need Figure B Sharps disposal container Alcohol wipe |
Panel 8 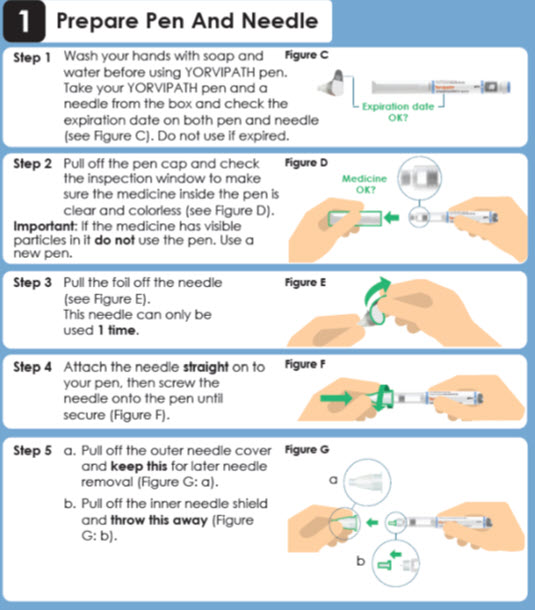 | 1 Prepare Pen And Needle Step 1 Wash your hands with soap and water before using YORVIPATH pen. Take your YORVIPATH pen and a needle from the box and check the expiration date on both pen and needle (see Figure C ). Do not use if expired. Figure C Expiration date OK? Step 2 Pull off the pen cap and check the inspection window to make sure the medicine inside the pen is clear and colorless (see Figure D ). Important: If the medicine has visible particles in it do not use the pen. Use a new pen.Figure D Medicine OK? Step 3 Pull the foil off the needle (see Figure E ). This needle can only be used 1 time .Figure E Step 4 Attach the needle straight on to your pen, then screw the needle onto the pen until secure (see Figure F ).Figure F Step 5
Figure G |
Panel 9 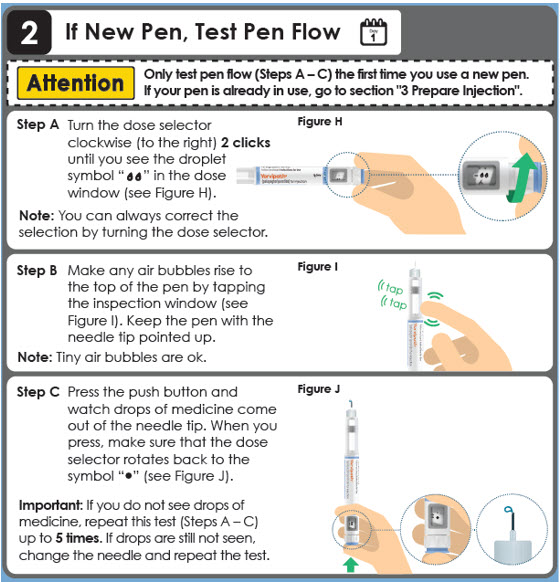 | 2 If New Pen, Test Pen Flow Day 1 Attention Only test pen flow (Steps A – C) the first time you use a new pen. If your pen is already in use, go to section "3 Prepare Injection".Step A Turn the dose selector clockwise (to the right) 2 clicks until you see the droplet symbol " Figure H Step B Make any air bubbles rise to the top of the pen by tapping the inspection window (see Figure I ). Keep the pen with the needle tip pointed up. Note: Tiny air bubbles are ok.Figure I tap tap Step C Press the push button and watch drops of medicine come out of the needle tip. When you press, make sure that the dose selector rotates back to the symbol "•" (see Figure J ). Important: If you do not see drops of medicine, repeat this test (Steps A – C) up to 5 times . If drops are still not seen, change the needle and repeat the test.Figure J |
Panel 10 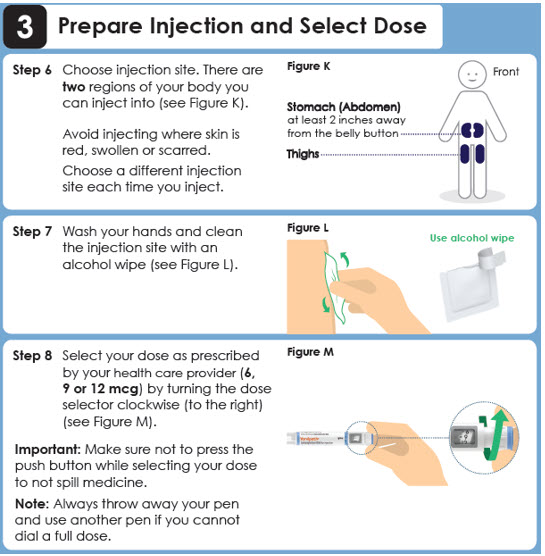 | 3 Prepare Injection and Select Dose Step 6 Choose injection site. There are two regions of your body you can inject into (see Figure K ). Avoid injecting where skin is red, swollen or scarred. Choose a different injection site each time you inject. Figure K Front Stomach (Abdomen) at least 2 inches away from the belly button Thighs Step 7 Wash your hands and clean the injection site with an alcohol wipe (see Figure L ).Figure L Use alcohol wipe Step 8 Select your dose as prescribed by your health care provider ( 6, 9 or 12 mcg ) by turning the dose selector clockwise (to the right) (see Figure M ). Important: Make sure not to press the push button while selecting your dose to not spill medicine. Note: Always throw away your pen and use another pen if you cannot dial a full dose.Figure M |
Panel 11 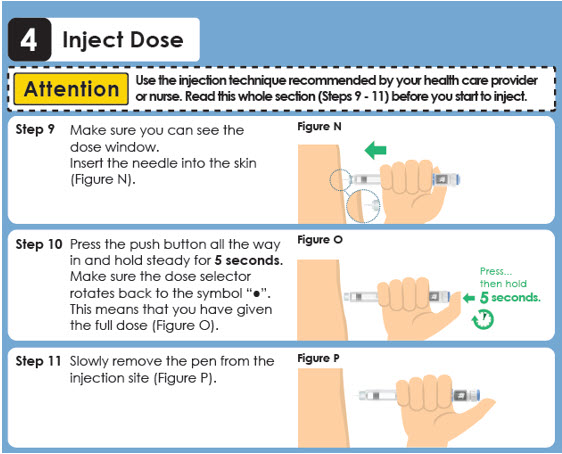 | 4 Inject Dose Attention Use the injection technique recommended by your health care provider or nurse. Read this whole section (Steps 9 - 11) before you start to inject. Step 9 Make sure you can see the dose window. Insert the needle into the skin (see Figure N ). Figure N Step 10 Press the push button all the way in and hold steady for 5 seconds . Make sure the dose selector rotates back to the symbol "●". This means that you have given the full dose (see Figure O ).Figure O Pres… then hold 5 seconds. Step 11 Slowly remove the pen from the injection site (see Figure P ).Figure P |
Panel 12 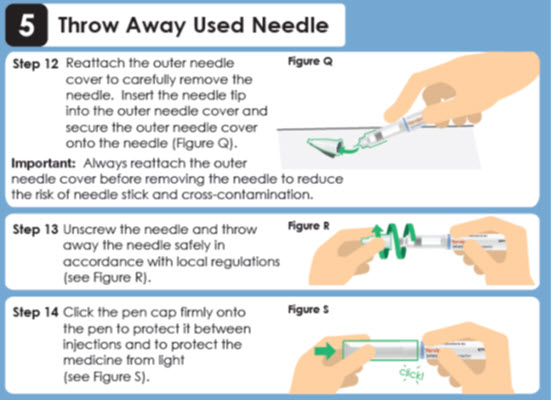 | 5 Throw Away Used Needle Step 12 Reattach the outer needle cover to carefully remove the needle. Insert the needle tip into the outer needle cover and secure the outer needle cover onto the needle (see Figure Q ). Important: Always reattach the outer needle cover before removing the needle to reduce the risk of needle stick and cross-contamination. Figure Q Step 13 Unscrew the needle and throw away the needle safely in accordance with local regulations (see Figure R ).Figure R Step 14 Click the pen cap firmly onto the pen to protect it between injections and to protect the medicine from light (see Figure S ).Figure S click! |
Panel 13  | 6 Throw Away Used Pen Day 14 Important: Always throw away the pen 14 days after first use according to local regulations. Always throw away your pen and any extra needles after 14 days of use , even if it still has medicine inside (see Figure T ). This is important to make sure that you get the full effect of your medicine. Figure T This instructions for Use has been approved by the U.S. Food and Drug Administration. Approved 10/2025 |
 " in the dose window (see
" in the dose window (see Mechanism of Action
At physiological conditions, palopegteriparatide releases PTH(1-34) to maintain a continuous systemic exposure. Endogenous PTH maintains extracellular calcium and phosphate homeostasis by increasing serum calcium and decreasing serum phosphate. These effects are mediated by stimulating bone turnover to mobilize calcium and phosphate from bone, promoting renal calcium reabsorption and phosphate excretion, and facilitating active vitamin D synthesis, in turn increasing intestinal absorption of calcium and phosphate. Similar to endogenous PTH, PTH(1-34) released from palopegteriparatide exerts these effects through its main receptor, parathyroid hormone 1 receptor (PTH1R), which is highly expressed on osteoblasts, osteocytes, renal tubular cells, and in several other tissues.