Get your patient on Betamethasone Dipropionate - Betamethasone Dipropionate ointment, Augmented (Betamethasone Dipropionate)
Betamethasone Dipropionate - Betamethasone Dipropionate ointment, Augmented prescribing information
RECENT MAJOR CHANGES
Warnings and Precautions,
Ophthalmic Adverse Reactions (5.2 ) 05/2019
INDICATIONS AND USAGE
Betamethasone dipropionate ointment USP (augmented) is a corticosteroid indicated for the relief of the inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses in patients 13 years of age or older.
DOSAGE AND ADMINISTRATION
Apply a thin film of betamethasone dipropionate ointment USP (augmented) to the affected skin areas once or twice daily.
Therapy should be discontinued when control is achieved. If no improvement is seen within 2 weeks, reassessment of diagnosis may be necessary. Betamethasone dipropionate ointment USP (augmented) is a super-high-potency topical corticosteroid. Treatment with betamethasone dipropionate ointment USP (augmented) should not exceed 50 g per week because of the potential for the drug to suppress the hypothalamic-pituitary-adrenal (HPA) axis [see WARNINGS AND PRECAUTIONS (5.1 )].
Betamethasone dipropionate ointment USP (augmented) should not be used with occlusive dressings unless directed by a physician.
Avoid use on the face, groin, or axillae, or if skin atrophy is present at the treatment site.
Avoid contact with eyes. Wash hands after each application.
Betamethasone dipropionate ointment USP (augmented) is for topical use only. It is not for oral, ophthalmic, or intravaginal use.
DOSAGE FORMS AND STRENGTHS
Ointment, 0.05%. Each gram of betamethasone dipropionate ointment USP (augmented), 0.05% contains 0.643 mg betamethasone dipropionate USP (equivalent to 0.5 mg betamethasone), in a white to off-white opaque ointment base.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no available data on betamethasone dipropionate ointment (augmented) use in pregnant women to identify a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes.
Observational studies suggest an increased risk of low birthweight infants with the use of greater than 300 grams of potent or very potent topical corticosteroid during a pregnancy. Advise pregnant women that betamethasone dipropionate ointment (augmented) may increase the risk of having a low birthweight infant and to use betamethasone dipropionate ointment (augmented) on the smallest area of skin and for the shortest duration possible.
In animal reproduction studies, increased malformations, including umbilical hernias, cephalocele, and cleft palate, were observed after intramuscular administration of betamethasone dipropionate to pregnant rabbits. The available data do not allow the calculation of relevant comparisons between the systemic exposure of betamethasone dipropionate in animal studies to the systemic exposure that would be expected in humans after topical use of betamethasone dipropionate ointment (augmented) (see Data) .
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Data
Animal Data
Betamethasone dipropionate has been shown to cause malformations in rabbits when given by the intramuscular route at doses of 0.05 mg/kg. The abnormalities observed included umbilical hernias, cephalocele, and cleft palate.
Lactation
Risk Summary
There are no data regarding the presence of betamethasone dipropionate in human milk, the effects on the breastfed infant, or the effects on milk production after topical application of betamethasone dipropionate ointment (augmented) to women who are breastfeeding.
It is possible that topical administration of betamethasone dipropionate could result in sufficient systemic absorption to produce detectable quantities in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for betamethasone dipropionate ointment (augmented) and any potential adverse effects on the breastfed infant from betamethasone dipropionate ointment (augmented) or from the underlying maternal condition.
Clinical Considerations
To minimize potential exposure to the breastfed infant via breast milk, use betamethasone dipropionate ointment (augmented) on the smallest area of skin and for the shortest duration possible while breastfeeding. Advise breastfeeding women not to apply betamethasone dipropionate ointment (augmented) directly to the nipple and areola to avoid direct infant exposure [see Use in Specific Populations (8.4 )] .
Pediatric Use
Use of betamethasone dipropionate ointment (augmented) in pediatric patients younger than 13 years of age is not recommended due to the potential for HPA axis suppression [see WARNINGS AND PRECAUTIONS (5.1 )] .
In an open-label HPA axis safety trial in subjects 3 months to 12 years of age with atopic dermatitis, DIPROLENE AF ® Cream 0.05% was applied twice daily for 2 to 3 weeks over a mean body surface area of 58% (range 35% to 95%). In 19 of 60 (32%) evaluable subjects, adrenal suppression was indicated by either a ≤5 mcg/dL pre-stimulation cortisol, or a cosyntropin post-stimulation cortisol ≤18 mcg/dL and/or an increase of <7 mcg/dL from the baseline cortisol. Out of the 19 subjects with HPA axis suppression, 4 subjects were tested 2 weeks after discontinuation of DIPROLENE AF ® Cream, and 3 of the 4 (75%) had complete recovery of HPA axis function. The proportion of subjects with adrenal suppression in this trial was progressively greater, the younger the age group.
Because of a higher ratio of skin surface area to body mass, pediatric patients are at a greater risk than adults of systemic toxicity when treated with topical drugs. They are, therefore, also at greater risk of HPA axis suppression and adrenal insufficiency upon the use of topical corticosteroids.
Rare systemic effects such as Cushing's syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in pediatric patients, especially those with prolonged exposure to large doses of high potency topical corticosteroids.
Local adverse reactions including skin atrophy have also been reported with use of topical corticosteroids in pediatric patients.
Avoid use of betamethasone dipropionate ointment (augmented) in the treatment of diaper dermatitis.
Geriatric Use
Clinical trials of betamethasone dipropionate ointment (augmented) included 225 subjects who were 65 years of age and over and 46 subjects who were 75 years of age and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients. However, greater sensitivity of some older individuals cannot be ruled out.
CONTRAINDICATIONS
Betamethasone dipropionate ointment (augmented) is contraindicated in patients who are hypersensitive to betamethasone dipropionate, to other corticosteroids, or to any ingredient in this preparation.
WARNINGS AND PRECAUTIONS
- Effects on endocrine system: Betamethasone dipropionate ointment (augmented) can cause reversible HPA axis suppression with the potential for glucocorticosteroid insufficiency during and after withdrawal of treatment. Risk factor(s) include the use of high-potency topical corticosteroids, use over a large surface area or to areas under occlusion, prolonged use, altered skin barrier, liver failure, and use in pediatric patients. Modify use should HPA axis suppression develop. (5.1 , 8.4 )
- Opthalmic Adverse Reactions: Betamethasone dipropionate ointment (augmented) may increase the risk of cataracts and glaucoma. If visual symptoms occur, consider referral to an ophthalmologist for evaluation. (5.2 )
Effects on Endocrine System
Betamethasone dipropionate ointment (augmented) can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for glucocorticosteroid insufficiency. This may occur during treatment or after withdrawal of treatment. Factors that predispose to HPA axis suppression include the use of high-potency steroids, large treatment surface areas, prolonged use, use of occlusive dressings, altered skin barrier, liver failure, and young age. Evaluation for HPA axis suppression may be done by using the adrenocorticotropic hormone (ACTH) stimulation test.
In a trial evaluating the effects of betamethasone dipropionate ointment (augmented) on the HPA axis, at 14 g per day, betamethasone dipropionate ointment (augmented) was shown to suppress the plasma levels of adrenal cortical hormones following repeated application to diseased skin in subjects with psoriasis. These effects were reversible upon discontinuation of treatment. At 7 g per day, betamethasone dipropionate ointment (augmented) was shown to cause minimal inhibition of the HPA axis when applied 2 times daily for 2 to 3 weeks in healthy subjects and in subjects with psoriasis and eczematous disorders.
With 6 g to 7 g of betamethasone dipropionate ointment (augmented) applied once daily for 3 weeks, no significant inhibition of the HPA axis was observed in subjects with psoriasis and atopic dermatitis, as measured by plasma cortisol and 24-hour urinary 17-hydroxy-corticosteroid levels.
If HPA axis suppression is documented, gradually withdraw the drug, reduce the frequency of application, or substitute with a less potent corticosteroid. Infrequently, signs and symptoms of steroid withdrawal may occur, requiring supplemental systemic corticosteroids.
Cushing's syndrome and hyperglycemia may also occur with topical corticosteroids. These events are rare and generally occur after prolonged exposure to excessively large doses, especially of high-potency topical corticosteroids.
Pediatric patients may be more susceptible to systemic toxicity due to their larger skin surface to body mass ratios [see USE IN SPECIFIC POPULATIONS (8.4 )] .
5.2 Opthalmic Adverse Reactions
Use of topical corticosteroids, including betamethasone dipropionate ointment (augmented), may increase the risk of posterior subcapsular cataracts and glaucoma. Cataracts and glaucoma have been reported postmarketing with the use of topical corticosteroid products, including betamethasone dipropionate ointment (augmented) [see ADVERSE REACTIONS (6.2 )].
Avoid contact of betamethasone dipropionate ointment (augmented) with eyes. Advise patients to report any visual symptoms and consider referral to an ophthalmologist for evaluation.
Allergic Contact Dermatitis
Allergic contact dermatitis with corticosteroids is usually diagnosed by observing failure to heal rather than noting a clinical exacerbation. Such an observation should be corroborated with appropriate diagnostic patch testing. If irritation develops, topical corticosteroids should be discontinued and appropriate therapy instituted.
ADVERSE REACTIONS
Most common adverse reactions (<1%) are: erythema, folliculitis, pruritus, and vesiculation. (6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Lupin Pharmaceuticals, Inc. at 1-800-399-2561 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
In controlled clinical trials, adverse reactions associated with the use of betamethasone dipropionate ointment (augmented) reported at a frequency of less than 1% included erythema, folliculitis, pruritus, and vesiculation.
Postmarketing Experience
Because adverse reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Postmarketing reports for local adverse reactions to topical corticosteroids may also include: skin atrophy, telangiectasias, burning, irritation, dryness, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, hypertrichosis, striae, and miliaria.
Hypersensitivity reactions, consisting of predominantly skin signs and symptoms, e.g., contact dermatitis, pruritus, bullous dermatitis, and erythematous rash have been reported.
Ophthalmic adverse reactions of cataracts, glaucoma, increased intraocular pressure, and central serous chorioretinopathy have been reported with the use of topical corticosteroids, including topical betamethasone products.
DESCRIPTION
Betamethasone dipropionate ointment USP (augmented), 0.05% contains betamethasone dipropionate USP, a synthetic adrenocorticosteroid, for topical use. Betamethasone, an analog of prednisolone, has a high degree of corticosteroid activity and a slight degree of mineralocorticoid activity. Betamethasone dipropionate is the 17, 21-dipropionate ester of betamethasone.
Chemically, betamethasone dipropionate is 9-fluoro-11β,17,21-trihydroxy-16β-methylpregna-1,4-diene-3,20-dione 17,21-dipropionate, with the empirical formula C 28 H 37 FO 7 , a molecular weight of 504.6 and the following structural formula:
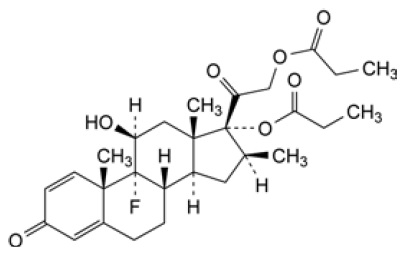
It is a white to cream-white, odorless powder practically insoluble in water, freely soluble in acetone, in methylene chloride and in chloroform, sparingly soluble in ethanol (96%).
Each gram of betamethasone dipropionate ointment USP (augmented), 0.05% contains 0.643 mg betamethasone dipropionate USP (equivalent to 0.5 mg betamethasone), in a white to off-white opaque ointment base of propylene glycol, propylene glycol monopalmitostearate, white petrolatum and white wax.
CLINICAL PHARMACOLOGY
Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action of betamethasone dipropionate ointment (augmented) in corticosteroid responsive dermatoses is unknown.
Pharmacodynamics
Vasoconstrictor Assay
Trials performed with betamethasone dipropionate ointment (augmented), 0.05% indicate that it is in the super-high range of potency as demonstrated in vasoconstrictor trials in healthy subjects when compared with other topical corticosteroids. However, similar blanching scores do not necessarily imply therapeutic equivalence.
Pharmacokinetics
No pharmacokinetics trials have been conducted with betamethasone dipropionate ointment (augmented).
The extent of percutaneous absorption of topical corticosteroids is determined by many factors including the vehicle, the integrity of the epidermal barrier, and the use of occlusive dressings.
Topical corticosteroids can be absorbed through normal intact skin. Inflammation and/or other disease processes in the skin may increase percutaneous absorption. Occlusive dressings substantially increase the percutaneous absorption of topical corticosteroids [see DOSAGE AND ADMINISTRATION (2 )] .
Once absorbed through the skin, topical corticosteroids enter pharmacokinetic pathways similar to systemically administered corticosteroids. Corticosteroids are bound to plasma proteins in varying degrees, are metabolized primarily in the liver, and excreted by the kidneys. Some of the topical corticosteroids and their metabolites are also excreted into the bile.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies have not been performed to evaluate the carcinogenic potential of betamethasone dipropionate.
Betamethasone was negative in the bacterial mutagenicity assay (Salmonella typhimurium and Escherichia coli) , and in the mammalian cell mutagenicity assay (CHO/HGPRT). It was positive in the in vitro human lymphocyte chromosome aberration assay, and equivocal in the in vivo mouse bone marrow micronucleus assay.
Studies in rabbits, mice, and rats using intramuscular doses up to 1, 33, and 2 mg/kg, respectively, resulted in dose-related increases in fetal resorptions in rabbits and mice.
CLINICAL STUDIES
The safety and efficacy of betamethasone dipropionate ointment (augmented) for the treatment of corticosteroid-responsive dermatoses, psoriasis and atopic dermatitis, have been evaluated in three randomized active-controlled trials, two in psoriasis and one in atopic dermatitis. A total of 378 subjects, of whom 152 received betamethasone dipropionate ointment (augmented), were included in these trials. These trials evaluated betamethasone dipropionate ointment (augmented) applied twice daily, for 14 days. Betamethasone dipropionate ointment (augmented) was shown to be effective in relieving signs and symptoms of psoriasis and atopic dermatitis.
HOW SUPPLIED/STORAGE AND HANDLING
Betamethasone dipropionate ointment USP (augmented), 0.05% is a white to off-white opaque ointment supplied in 15-g (NDC 68180-947-01) and 50-g (NDC 68180-947-02) tubes.
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Mechanism of Action
Corticosteroids play a role in cellular signaling, immune function, inflammation, and protein regulation; however, the precise mechanism of action of betamethasone dipropionate ointment (augmented) in corticosteroid responsive dermatoses is unknown.