Get your patient on Etoposide - Etoposide capsule (Etoposide)
Etoposide - Etoposide capsule prescribing information
WARNINGS
Etoposide should be administered under the supervision of a qualified physician experienced in the use of cancer chemotherapeutic agents. Severe myelosuppression with resulting infection or bleeding may occur.
INDICATIONS AND USAGE
Etoposide capsules are indicated in the management of the following neoplasms:
Small Cell Lung Cancer
Etoposide capsules in combination with other approved chemotherapeutic agents as first line treatment in patients with small cell lung cancer.
DOSAGE AND ADMINISTRATION
Etoposide Capsules
In small cell lung cancer, the recommended dose of etoposide capsules is two times the IV dose rounded to the nearest 50 mg (i.e., Two times 35 mg/m 2 /day for 4 days to 50 mg/m 2 /day for 5 days).
The dosage should be modified to take into account the myelosuppressive effects of other drugs in the combination or the effects of prior x-ray therapy or chemotherapy which may have compromised bone marrow reserve.
Stability
Etoposide capsules must be stored under refrigeration 2° to 8°C (36° to 46°F). The capsules are stable for 36 months under such refrigeration conditions.
Procedures for proper handling and disposal of anticancer drugs should be considered. Several guidelines on this subject have been published 1-8 . There is no general agreement that all of the procedures recommended in the guidelines are necessary or appropriate.
CONTRAINDICATIONS
Etoposide capsules are contraindicated in patients who have demonstrated a previous hypersensitivity to etoposide or any component of the formulation.
ADVERSE REACTIONS
The following data on adverse reactions are based on both oral and intravenous administration of etoposide as a single agent, using several different dose schedules for treatment of a wide variety of malignancies.
Hematologic Toxicity
Myelosuppression is dose related and dose limiting, with granulocyte nadirs occurring 7 to 14 days after drug administration and platelet nadirs occurring 9 to 16 days after drug administration. Bone marrow recovery is usually complete by day 20, and no cumulative toxicity has been reported. Fever and infection have also been reported in patients with neutropenia. Death associated with myelosuppression has been reported.
The occurrence of acute leukemia with or without a preleukemic phase has been reported rarely in patients treated with etoposide in association with other antineoplastic agents (see WARNINGS ).
Gastrointestinal Toxicity
Nausea and vomiting are the major gastrointestinal toxicities. The severity of such nausea and vomiting is generally mild to moderate with treatment discontinuation required in 1% of patients. Nausea and vomiting can usually be controlled with standard antiemetic therapy. Mild to severe mucositis/esophagitis may occur. Gastrointestinal toxicities are slightly more frequent after oral administration than after intravenous infusion.
Hypotension
Transient hypotension following rapid intravenous administration has been reported in 1% to 2% of patients. It has not been associated with cardiac toxicity or electrocardiographic changes. No delayed hypotension has been noted. To prevent this rare occurrence, it is recommended that etoposide be administered by slow intravenous infusion over a 30- to 60-minute period. If hypotension occurs, it usually responds to cessation of the infusion and administration of fluids or other supportive therapy as appropriate. When restarting the infusion, a slower administration rate should be used.
Allergic Reactions
Anaphylactic-like reactions characterized by chills, fever, tachycardia, bronchospasm, dyspnea and/or hypotension have been reported to occur in 0.7% to 2% of patients receiving intravenous etoposide and in less than 1% of the patients treated with the oral capsules. These reactions have usually responded promptly to the cessation of the infusion and administration of pressor agents, corticosteroids, antihistamines or volume expanders as appropriate; however, the reactions can be fatal. Hypertension and/or flushing have also been reported. Blood pressure usually normalizes within a few hours after cessation of the infusion. Anaphylactic-like reactions have occurred during the initial infusion of etoposide.
Facial/tongue swelling, coughing, diaphoresis, cyanosis, tightness in throat, laryngospasm, back pain and/or loss of consciousness have sometimes occurred in association with the above reactions. In addition, an apparent hypersensitivity-associated apnea has been reported rarely.
Rash, urticaria, and/or pruritus have infrequently been reported at recommended doses. At investigational doses, a generalized pruritic erythematous maculopapular rash, consistent with perivasculitis, has been reported.
Alopecia
Reversible alopecia, sometimes progressing to total baldness, was observed in up to 66% of patients.
Other Toxicities
The following adverse reactions have been infrequently reported: abdominal pain, aftertaste, constipation, dysphagia, asthenia, fatigue, malaise, somnolence, transient cortical blindness, optic neuritis, interstitial pneumonitis/pulmonary fibrosis, fever, seizure (occasionally associated with allergic reactions), Stevens-Johnson Syndrome, and toxic epidermal necrolysis, pigmentation, and a single report of radiation recall dermatitis.
Hepatic toxicity, generally in patients receiving higher doses of the drug than those recommended, has been reported with etoposide. Metabolic acidosis has also been reported in patients receiving higher doses.
The incidences of adverse reactions in the table that follows are derived from multiple data bases from studies in 2,081 patients when etoposide was used either orally or by injection as a single agent.
ADVERSE DRUG EFFECT | PERCENT RANGE OF REPORTED INCIDENCE |
Hematologic toxicity Leukopenia (less than 1,000 WBC/mm 3 ) Leukopenia (less than 4,000 WBC/mm 3 ) Thrombocytopenia (less than 50,000 platelets/mm 3 ) Thrombocytopenia (less than 100,000 platelets/mm 3 ) Anemia | 3 to 17 60 to 91 1 to 20 22 to 41 0 to 33 |
Gastrointestinal toxicity Nausea and vomiting Abdominal pain Anorexia Diarrhea Stomatitis Hepatic | 31 to 43 0 to 2 10 to 13 1 to 13 1 to 6 0 to 3 |
Alopecia Peripheral neurotoxicity Hypotension Allergic reaction | 8 to 66 1 to 2 1 to 2 1 to 2 |
Drug Interactions
High-dose cyclosporin A resulting in concentrations above 2000 ng/mL administered with oral etoposide has led to an 80% increase in etoposide exposure with a 38% decrease in total body clearance of etoposide compared to etoposide alone.
DESCRIPTION
Etoposide (also commonly known as VP-16) is a semisynthetic derivative of podophyllotoxin used in the treatment of certain neoplastic diseases. It is 4’-Demethylepipodophyllotoxin 9-[4,6-O-( R )-ethylidene-β-D-glucopyranoside]. It is very soluble in methanol and chloroform, slightly soluble in ethanol, and sparingly soluble in water and ether. It is made more miscible with water by means of organic solvents. It has a molecular weight of 588.56 and a molecular formula of C 29 H 32 O 13 .
Etoposide may be administered either intravenously or orally. Etoposide capsules, USP are available as 50 mg opaque dark pink, oblong capsules. Each liquid filled, soft gelatin capsule contains 50 mg of etoposide, USP in a vehicle consisting of citric acid anhydrous, glycerol and polyethylene glycol. The soft gelatin capsules contain anidrisorb, gelatin and glycerol with the following dye system: red iron oxide and titanium dioxide; the capsules are printed with edible black ink containing FD&C Blue No. 1 Aluminum Lake, FD&C Red No. 40 Aluminum Lake, hypromellose and propylene glycol.
The structural formula is:
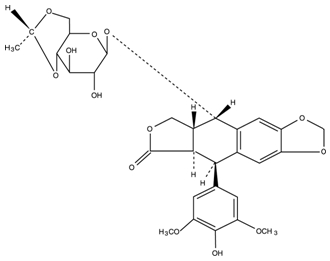
CLINICAL PHARMACOLOGY
Etoposide has been shown to cause metaphase arrest in chick fibroblasts. Its main effect, however, appears to be at the G 2 portion of the cell cycle in mammalian cells. Two different dose dependent responses are seen. At high concentrations (10 mcg/mL or more), lysis of cells entering mitosis is observed. At low concentrations (0.3 mcg/mL to 10 mcg/mL), cells are inhibited from entering prophase. It does not interfere with microtubular assembly. The predominant macromolecular effect of etoposide appears to be the induction of DNA strand breaks by an interaction with DNA topoisomerase II or the formation of free radicals.
Pharmacokinetics
On intravenous administration, the disposition of etoposide is best described as a biphasic process with a distribution half-life of about 1.5 hours and terminal elimination half-life ranging from 4 to 11 hours. Total body clearance values range from 33 mL/min to 48 mL/min or 16 mL/min/m 2 to 36 mL/min/m 2 and, like the terminal elimination half-life, are independent of dose over a range 100 mg/m 2 to 600 mg/m 2 . Over the same dose range, the areas under the plasma concentration vs. time curves (AUC) and the maximum plasma concentration (C max ) values increase linearly with dose. Etoposide does not accumulate in the plasma following daily administration of 100 mg/m 2 for 4 to 5 days.
The mean volumes of distribution at steady-state fall in the range of 18 to 29 liters or 7 L/m 2 to 17 L/m 2 . Etoposide enters the CSF poorly. Although it is detectable in CSF and intracerebral tumors, the concentrations are lower than in extracerebral tumors and in plasma. Etoposide concentrations are higher in normal lung than in lung metastases and are similar in primary tumors and normal tissues of the myometrium. In vitro , etoposide is highly protein bound (97%) to human plasma proteins. An inverse relationship between plasma albumin levels and etoposide renal clearance is found in children. In a study determining the effect of other therapeutic agents on the in vitro binding of 14 C-etoposide to human serum proteins, only phenylbutazone, sodium salicylate and aspirin displaced protein bound etoposide at concentrations achieved in vivo .
Etoposide binding ratio correlates directly with serum albumin in patients with cancer and in normal volunteers. The unbound fraction of etoposide significantly correlated with bilirubin in a population of cancer patients. Data have suggested a significant inverse correlation between serum albumin concentration and free fraction of etoposide (see PRECAUTIONS ).
After intravenous administration of 14 C-etoposide (100 mg/m 2 to 124 mg/m 2 ), mean recovery of radioactivity in the urine was 56% of the dose at 120 hours, 45% of which was excreted as etoposide; fecal recovery of radioactivity was 44% of the dose at 120 hours.
In children, approximately 55% of the dose is excreted in the urine as etoposide in 24 hours. The mean renal clearance of etoposide is 7 mL/min/m 2 to 10 mL/min/m 2 or about 35% of the total body clearance over a dose range of 80 mg/m 2 to 600 mg/m 2 . Etoposide, therefore, is cleared by both renal and nonrenal processes, i.e., metabolism and biliary excretion. The effect of renal disease on plasma etoposide clearance is not known.
Biliary excretion of unchanged drug and/or metabolites is an important route of etoposide elimination as fecal recovery of radioactivity is 44% of the intravenous dose. The hydroxy acid metabolite [4’-demethylepipodophyllic acid-9-(4,6-0-( R )-ethylidene-ß-D-glucopyranoside)], formed by opening of the lactone ring, is found in the urine of adults and children. It is also present in human plasma, presumably as the trans isomer. Glucoronide and/or sulfate conjugates of etoposide are also excreted in human urine. Only 8% or less of an intravenous dose is excreted in the urine as radiolabeled metabolites of 14 C-etoposide. In addition, 0-demethylation of the dimethoxyphenol ring occurs through the CYP450 3A4 isoenzyme pathway to produce the corresponding catechol.
After either intravenous infusion or oral capsule administration, the C max and AUC values exhibit marked intra- and inter-subject variability. This results in variability in the estimates of the absolute oral bioavailability of etoposide oral capsules.
C max and AUC values for orally administered etoposide capsules consistently fall in the same range as the C max and AUC values for an intravenous dose of one-half the size of the oral dose. The overall mean value of oral capsule bioavailability is approximately 50% (range 25% to 75%). The bioavailability of etoposide capsules appears to be linear up to a dose of at least 250 mg/m 2 .
There is no evidence of a first-pass effect for etoposide. For example, no correlation exists between the absolute oral bioavailability of etoposide capsules and nonrenal clearance. No evidence exists for any other differences in etoposide metabolism and excretion after administration of oral capsules as compared to intravenous infusion.
In adults, the total body clearance of etoposide is correlated with creatinine clearance, serum albumin concentration and nonrenal clearance. Patients with impaired renal function receiving etoposide have exhibited reduced total body clearance, increased AUC and a lower volume of distribution at steady-state (see PRECAUTIONS ). Use of cisplatin therapy is associated with reduced total body clearance. In children, elevated serum SGPT levels are associated with reduced drug total body clearance. Prior use of cisplatin may also result in a decrease of etoposide total body clearance in children.
Although some minor differences in pharmacokinetic parameters between age and gender have been observed, these differences were not considered clinically significant.
HOW SUPPLIED
Etoposide Capsules, USP are available containing 50 mg of etoposide, USP.
The 50 mg capsule is an opaque dark pink, soft gelatin capsule printed with E50 in black ink. They are available as follows:
NDC 0378-3266-94 20 Capsules - Unit Dose
Capsules are to be stored under refrigeration, between 2° to 8°C (36° to 46°F).
Protect from freezing.
Dispense in a tight, light-resistant container as defined in the USP using a child-resistant closure.