Get your patient on Hydrocortisone - Hydrocortisone tablet (Hydrocortisone)
Hydrocortisone - Hydrocortisone tablet prescribing information
INDICATIONS AND USAGE
Hydrocortisone Tablets are indicated in the following conditions.
Endocrine Disorders
Primary or secondary adrenocortical insufficiency (hydrocortisone or cortisone is the first choice; synthetic analogs may be used in conjunction with mineralocorticoids where applicable; in infancy mineralocorticoid supplementation is of particular importance) Congenital adrenal hyperplasia Non suppurative thyroiditis Hypercalcemia associated with cancer
Rheumatic Disorders
As adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in: Psoriatic arthritis Rheumatoid arthritis, including juvenile rheumatoid arthritis (selected cases may require low-dose maintenance therapy) Ankylosing spondylitis Acute and subacute bursitis Acute nonspecific tenosynovitis Acute gouty arthritis Post-traumatic osteoarthritis Synovitis of osteoarthritis Epicondylitis
Collagen Diseases
During an exacerbation or as maintenance therapy in selected cases of: Systemic lupus erythematosus Systemic dermatomyositis (polymyositis) Acute rheumatic carditis
Dermatologic Diseases
Pemphigus Bullous dermatitis herpetiformis Severe erythema multiforme (Stevens-Johnson syndrome) Exfoliative dermatitis Mycosis fungoides Severe psoriasis Severe seborrheic dermatitis
Allergic States
Control of severe or incapacitating allergic conditions intractable to adequate trials of conventional treatment: Seasonal or perennial allergic rhinitis Serum sickness Bronchial asthma Contact dermatitis Atopic dermatitis Drug hypersensitivity reactions
Ophthalmic Diseases
Severe acute and chronic allergic and inflammatory processes involving the eye and its adnexa such as: Allergic conjunctivitis Keratitis Allergic corneal marginal ulcers Herpes zoster ophthalmicus Iritis and iridocyclitis Chorioretinitis Anterior segment inflammation Diffuse posterior uveitis and choroiditis Optic neuritis Sympathetic ophthalmia
Respiratory Diseases
Symptomatic sarcoidosis Loeffler's syndrome not manageable by other means Berylliosis Fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate antituberculous chemotherapy Aspiration pneumonitis
Hematologic Disorders
Idiopathic thrombocytopenic purpura in adults Secondary thrombocytopenia in adults Acquired (autoimmune) hemolytic anemia Erythroblastopenia (RBC anemia) Congenital (erythroid) hypoplastic anemia
Neoplastic Diseases
For palliative management of: Leukemias and lymphomas in adults Acute leukemia of childhood
Edematous States
To induce a diuresis or remission of proteinuria in the nephrotic syndrome, without uremia, of the idiopathic type or that due to lupus erythematosus.
Gastrointestinal Diseases
To tide the patient over a critical period of the disease in: Ulcerative colitis Regional enteritis
Miscellaneous
Tuberculous meningitis with subarachnoid block or impending block when used concurrently with appropriate antituberculous chemotherapy Trichinosis with neurologic or myocardial involvement
DOSAGE AND ADMINISTRATION
The initial dosage of hydrocortisone Tablets may vary from 20 mg to 240 mg of hydrocortisone per day depending on the specific disease entity being treated. In situations of less severity lower doses will generally suffice while in selected patients higher initial doses may be required. The initial dosage should be maintained or adjusted until a satisfactory response is noted. If after a reasonable period of time there is a lack of satisfactory clinical response, hydrocortisone should be discontinued and the patient transferred to other appropriate therapy. IT SHOULD BE EMPHASIZED THAT DOSAGE REQUIREMENTS ARE VARIABLE AND MUST BE INDIVIDUALIZED ON THE BASIS OF THE DISEASE UNDER TREATMENT AND THE RESPONSE OF THE PATIENT. After a favorable response is noted, the proper maintenance dosage should be determined by decreasing the initial drug dosage in small decrements at appropriate time intervals until the lowest dosage which will maintain an adequate clinical response is reached. It should be kept in mind that constant monitoring is needed in regard to drug dosage. Included in the situations which may make dosage adjustments necessary are changes in clinical status secondary to remissions or exacerbations in the disease process, the patient's individual drug responsiveness, and the effect of patient exposure to stressful situations not directly related to the disease entity under treatment; in this latter situation it may be necessary to increase the dosage of hydrocortisone tablets for a period of time consistent with the patient's condition. If after long-term therapy the drug is to be stopped, it is recommended that it be withdrawn gradually, rather than abruptly.
CONTRAINDICATIONS
Systemic fungal infections and known hypersensitivity to components
ADVERSE REACTIONS
Fluid and Electrolyte Disturbances Sodium retention Fluid retention Congestive heart failure in susceptible patients Potassium loss Hypokalemic alkalosis Hypertension
Musculoskeletal Muscle weakness Steroid myopathy Loss of muscle mass Osteoporosis Tendon rupture, particularly of the Achilles tendon Vertebral compression fractures Aseptic necrosis of femoral and humeral heads Pathologic fracture of long bones
Gastrointestinal Peptic ulcer with possible perforation and hemorrhage Pancreatitis Abdominal distention Ulcerative esophagitis Increases in alanine transaminase (ALT, SGPT), aspartate transaminase (AST, SGOT) and alkaline phosphatase have been observed following corticosteroid treatment. These changes are usually small, not associated with any clinical syndrome and are reversible upon discontinuation.
Dermatologic Impaired wound healing Thin fragile skin Petechiae and ecchymoses Facial erythema Increased sweating May suppress reactions to skin tests
Neurological Increased intracranial pressure with papilledema (pseudotumor cerebri) usually after treatment Convulsions Vertigo Headache Epidural lipomatosis
Endocrine Development of Cushingoid state Suppression of growth in children Secondary adrenocortical and pituitary unresponsiveness, particularly in times of stress, as in trauma, surgery or illness Menstrual irregularities Decreased carbohydrate tolerance Manifestations of latent diabetes mellitus Increased requirements for insulin or oral hypoglycemic agents in diabetics
Ophthalmic Central serous chorioretinopathy Posterior subcapsular cataracts Increased intraocular pressure Glaucoma Exophthalmos
Metabolic Negative nitrogen balance due to protein catabolism
Blood and lymphatic system disorders Leukocytosis
Drug Interactions
The pharmacokinetic interactions listed below are potentially clinically important. Drugs that induce hepatic enzymes such as phenobarbital, phenytoin and rifampin may increase the clearance of corticosteroids and may require increases in corticosteroid dose to achieve the desired response. Drugs such as troleandomycin and ketoconazole may inhibit the metabolism of corticosteroids and thus decrease their clearance. Therefore, the dose of corticosteroid should be titrated to avoid steroid toxicity. Corticosteroids may increase the clearance of chronic high dose aspirin. This could lead to decreased salicylate serum levels or increase the risk of salicylate toxicity when corticosteroid is withdrawn. Aspirin should be used cautiously in conjunction with corticosteroids in patients suffering from hypoprothrombinemia. The effect of corticosteroids on oral anticoagulants is variable. There are reports of enhanced as well as diminished effects of anticoagulants when given concurrently with corticosteroids. Therefore, coagulation indices should be monitored to maintain the desired anticoagulant effect.
Information for the Patient Persons who are on immunosuppressant doses of corticosteroids should be warned to avoid exposure to chicken pox or measles. Patients should also be advised that if they are exposed, medical advice should be sought without delay.
DESCRIPTION
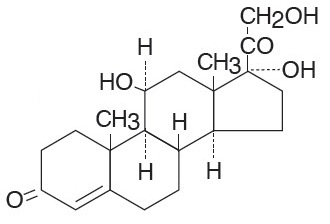
Hydrocortisone Tablets, USP contain hydrocortisone which is a glucocorticoid. Glucocorticoids are adrenocortical steroids, both naturally occurring and synthetic, which are readily absorbed from the gastrointestinal tract. Hydrocortisone, USP is white to practically white, odorless, crystalline powder with a melting point of about 215° C. It is very slightly soluble in water and in ether; sparingly soluble in acetone and in alcohol; slightly soluble in chloroform.
The chemical name for hydrocortisone is pregn-4-ene-3,20-dione,11,17,21-trihydroxy-, (11β)-. Its molecular weight is 362.46 and the structural formula is as outlined below.
Hydrocortisone Tablets, USP are available for oral administration in three strengths: each tablet contains either 5 mg, 10 mg, or 20 mg of hydrocortisone, USP. Inactive ingredients: calcium stearate, corn starch, lactose monohydrate, sorbic acid, sucrose.
FDA approved dissolution test specifications differ from USP.
ACTIONS Naturally occurring glucocorticoids (hydrocortisone and cortisone), which also have salt-retaining properties, are used as replacement therapy in adrenocortical deficiency states. Their synthetic analogs are primarily used for their potent anti-inflammatory effects in disorders of many organ systems.
Glucocorticoids cause profound and varied metabolic effects. In addition, they modify the body's immune responses to diverse stimuli.
HOW SUPPLIED
Hydrocortisone Tablets, USP are available in the following strengths and package sizes: 5 mg ( White to off white, round shaped bevel edged, bi-convex tablets debossed with “5” on one side and scored on the other side.)
Bottles of 50 NDC 71930-078-50
10 mg (White to off white, round shaped bevel edged, bi-convex tablets debossed with “10” on one side and scored on the other side.)
Bottles of 100 NDC 71930-079-12
20 mg ( White to off white, round shaped bevel edged, bi-convex tablets debossed with “20” on one side and scored on the other side.)
Bottles of 100 NDC 71930-080-12
Store at 20° to 25°C (68° to 77°F). Excursions permitted between 15° and 30°C (59° and 86°F). (See USP controlled room temperature).