Get your patient on Jesduvroq (Daprodustat)
Jesduvroq patient education
Patient toolkit
Dosage & administration

Jesduvroq prescribing information
WARNING: INCREASED RISK OF DEATH, MYOCARDIAL INFARCTION, STROKE, VENOUS THROMBOEMBOLISM, and THROMBOSIS OF VASCULAR ACCESS
JESDUVROQ increases the risk of thrombotic vascular events, including major adverse cardiovascular events (MACE) [see Warnings and Precautions (5.1 )] .
Targeting a hemoglobin level greater than 11 g/dL is expected to further increase the risk of death and arterial venous thrombotic events, as occurs with erythropoietin stimulating agents (ESAs), which also increase erythropoietin levels [see Warnings and Precautions (5.1 )] .
No trial has identified a hemoglobin target level, dose of JESDUVROQ, or dosing strategy that does not increase these risks [see Dosage and Administration (2.4 )].
Use the lowest dose of JESDUVROQ sufficient to reduce the need for red blood cell transfusions [see Dosage and Administration (2.4 )] .
INDICATIONS AND USAGE
JESDUVROQ is indicated for the treatment of anemia due to chronic kidney disease (CKD) in adults who have been receiving dialysis for at least four months.
Limitations of Use
JESDUVROQ has not been shown to improve quality of life, fatigue, or patient well-being.
JESDUVROQ is not indicated for use:
- As a substitute for red blood cell transfusions in patients who require immediate correction of anemia.
- For treatment of anemia of chronic kidney disease in patients who are not on dialysis.
DOSAGE AND ADMINISTRATION
Pre-Treatment and On-Treatment Evaluations of Anemia, Iron Stores, and Liver Tests
Evaluation of Anemia and Iron Stores
Correct and exclude other causes of anemia (e.g., vitamin deficiency, metabolic or chronic inflammatory conditions, bleeding) before initiating JESDUVROQ. Evaluate the iron status in all patients before and during treatment with JESDUVROQ. Administer supplemental iron therapy when serum ferritin is less than 100 ng/ml or when serum transferrin saturation is less than 20%. The majority of patients with CKD will require supplemental iron during the course of therapy.
Liver Testing
Assess serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, and total bilirubin prior to initiation of JESDUVROQ. Repeat the liver tests if the patient develops signs or symptoms that could be consistent with liver disease during treatment with JESDUVROQ.
Important Dosing Information
Individualize dosing and use the lowest dose of JESDUVROQ sufficient to reduce the need for red blood cell transfusions. Do not target a hemoglobin higher than 11 g/dL.
JESDUVROQ can be taken with or without food, and without regard to concomitant administration of iron or phosphate binders [see Clinical Pharmacology (12.3 )] .
JESDUVROQ should be swallowed whole. Tablets should not be cut, crushed, or chewed.
JESDUVROQ can be administered without regard to the timing or type of dialysis [see Clinical Pharmacology (12.3 )] .
If a dose of JESDUVROQ is missed, it should be taken as soon as possible, unless it is the same day as the next dose. In this case, the missed dose should be skipped, and the next dose taken at the usual time. Double-doses should not be taken to make-up for a missed dose.
Recommended Starting Dose of JESDUVROQ
Adults with Anemia Due to Chronic Kidney Disease Receiving Dialysis for at Least 4 Months
Adults Not Being Treated with an ESA: For adults not being treated with an ESA, the starting dose of JESDUVROQ is based on the hemoglobin level (see Table 1 ). Dose modifications are needed for patients receiving concomitant treatment with a moderate CYP2C8 inhibitor or moderate hepatic impairment [see Dosage and Administration (2.5 , 2.6 ), Drug Interactions (7.1 ), Use in Specific Populations (8.6 ), Clinical Pharmacology (12.3 )] .
Pre-Treatment Hemoglobin Level (g/dL) | Starting Dose of JESDUVROQ (Once Daily Dosing) a |
<9 | 4 mg |
≥9 to ≤10 | 2 mg |
>10 | 1 mg |
- a See dosing modifications in Section 2.5 if the patient has moderate hepatic impairment and Section 2.6 if the patient is on a moderate CYP2C8 inhibitor.
Adults Being Switched from an ESA: For adults being switched from an ESA to JESDUVROQ, the starting dose of JESDUVROQ is based on the dose regimen of the ESA at the time of substitution (see Table 2 ). Dose modifications are needed for patients receiving concomitant treatment with a moderate CYP2C8 inhibitor or moderate hepatic impairment [see Dosage and Administration (2.5 , 2.6 ), Drug Interactions (7.1 ), Use in Specific Populations (8.6 ), Clinical Pharmacology (12.3 )] .
Current Dose of ESA | Dose of JESDUVROQ a | ||
Epoetin Alfa b Intravenous (units/week) | Darbepoetin Alfa Subcutaneous /Intravenous (mcg/4 weeks) | Methoxy PEG-Epoetin Beta Subcutaneous /Intravenous (mcg/month) | Once Daily Dosing |
Less than or equal to 2,000 | 20 to 30 | 30 to 40 | 4 mg |
Greater than 2,000 to less than 10,000 | Greater than 30 to 150 | Greater than 40 to 180 | 6 mg |
Greater than or equal to 10,000 to less than 20,000 | Greater than 150 to 300 | Greater than 180 to 360 | 8 mg |
Greater than or equal to 20,000 | Greater than 300 | Greater than 360 | 12 mg |
ESA = Erythropoiesis stimulating agent.
- a See dosing modifications in Section 2.5 if the patient has moderate hepatic impairment and Section 2.6 if the patient is on a moderate CYP2C8 inhibitor.
- b For patients on subcutaneous epoetin alfa, convert the epoetin alfa subcutaneous dose to intravenous dose equivalent by multiplying the subcutaneous dose received per week by 1.42 to obtain the weekly intravenous dose.
Monitoring Response to Therapy and Dose Adjustment
Following initiation of therapy and after each dose adjustment, monitor hemoglobin every 2 weeks for the first month and then every 4 weeks thereafter.
When adjusting doses of JESDUVROQ, consider hemoglobin rate of rise, rate of decline and hemoglobin variability. Do not increase the dose of JESDUVROQ more frequently than once every 4 weeks.
- If the dose of JESDUVROQ needs to be adjusted, increase or decrease by one dose level at a time (see Table 3 ).
- Decrease the dose of JESDUVROQ if hemoglobin increases rapidly (e.g., greater than 1 g/dL over 2 weeks or greater than 2 g/dL over 4 weeks) or if the hemoglobin exceeds 11 g/dL.
- If hemoglobin exceeds 12 g/dL , interrupt treatment with JESDUVROQ. When the hemoglobin is within the target range, treatment may be restarted at one dose level lower (see Table 3 ).
- Treatment with JESDUVROQ should not be continued beyond 24 weeks of therapy if a clinically meaningful increase in hemoglobin level is not achieved. Alternative explanations for an inadequate response should be sought and treated before re-starting therapy.
Daily dose of JESDUVROQ | 1 mg | 2 mg | 4 mg | 6 mg | 8 mg | 12 mg | 16 mg | 24 mg a |
a 24 mg is the maximum recommended once daily dose.
Dosage Modification for Hepatic Impairment
Reduce the starting dose of JESDUVROQ by half (see Table 1 and Table 2 ) in patients with moderate hepatic impairment (Child-Pugh Class B) except in patients whose starting dose is already 1 mg.
Use of JESDUVROQ in patients with severe hepatic impairment (Child-Pugh Class C) is not recommended [see Use in Specific Populations (8.6 ), Clinical Pharmacology (12.3 )] .
Dosage Modification for Concomitant Treatment with Moderate CYP2C8 Inhibitors
Reduce the starting dose of JESDUVROQ by half (see Table 1 and Table 2 ) in patients who are on clopidogrel or a moderate CYP2C8 inhibitor except in patients whose starting dose is already 1 mg [see Drug Interactions (7.1 ), Clinical Pharmacology (12.3 )] .
Monitor hemoglobin and adjust the dose of JESDUVROQ when initiating or stopping therapy with clopidogrel or a moderate CYP2C8 inhibitor during treatment with JESDUVROQ.
DOSAGE FORMS AND STRENGTHS
Tablets:
- 1 mg, gray, biconvex, round film-coated tablets debossed with “GS KF” on one face.
- 2 mg, yellow, biconvex, round film-coated tablets debossed with “GS V7” on one face.
- 4 mg, white, biconvex, round film-coated tablets debossed with “GS 13” on one face.
- 6 mg, pink, biconvex, round film-coated tablets debossed with “GS IM” on one face.
- 8 mg, orange, biconvex, round film-coated tablets debossed with “GS 5E” on one face.
USE IN SPECIFIC POPULATIONS
- Pregnancy: May cause fetal harm. (8.1 )
- Lactation: Breastfeeding not recommended until one week after the final dose. (8.2 )
- Hepatic Impairment: Reduce the starting dose in patients with moderate hepatic impairment (Child-Pugh Class B). JESDUVROQ not recommended in severe hepatic impairment (Child-Pugh Class C). (8.6 )
Pregnancy
Risk Summary
Available data with JESDUVROQ use in pregnant women are insufficient to establish a drug associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. There are risks to the mother and the fetus associated with CKD ( see Clinical Considerations ) . Daprodustat administered orally to pregnant rats and rabbits during the period of organogenesis was associated with adverse fetal outcomes, including embryonic and fetal loss and reduced fetal weight, at doses that caused maternal toxicity and polycythemia ( see Data ). Advise pregnant women of the potential risk to the fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk: CKD in pregnancy increases the risk for maternal hypertension, preeclampsia, miscarriage, stillbirth, preterm delivery, low birth weight infants, and polyhydramnios.
Data
Animal Data : Daprodustat was orally administered to pregnant rats at 0.5, 7, or 60 mg/kg/day from gestation day 6 to gestation day 17 during the period of organogenesis. No adverse effects were observed at doses less than or equal to 7 mg/kg/day (3 times the maximum recommended human dose [MRHD] based on body surface area). Daprodustat administration resulted in post-implantation loss, increased embryofetal death, and reduction in skeletal ossification in rats at a dose of 60 mg/kg/day (24 times the MRHD based on body surface area), which was associated with maternal toxicity (reduced body weight gain or weight loss). Maternal toxicity occurred at doses associated with polycythemia.
Daprodustat was orally administered to pregnant rabbits at doses of 4, 30, or 60 mg/kg/day from gestation day 7 until gestation day 19 during the period of organogenesis. No adverse effects were observed at doses less than or equal to 30 mg/kg/day (24 times the MRHD based on body surface area). Daprodustat administration was associated with a low incidence of abortions and fetal skeletal malformations (irregularly shaped anterior fontanelle, manubrium, fused sternal centra, and microphthalmia) at a dose of 60 mg/kg/day (49 times the MRHD based on body surface area) in the presence of maternal toxicity (reduced body weight gain or weight loss) and polycythemia.
In a pre- and postnatal development study, pregnant rats were dosed orally with daprodustat from implantation until weaning (gestation day 6 to lactation day 21) at 0.8, 7, or 40 mg/kg/day concomitantly with 3 major human metabolites of daprodustat. No adverse effects were observed at doses less than or equal to 7 mg/kg/day (3 times the MRHD based on body surface area). Maternal toxicity (in the presence of polycythemia) was noted at 40 mg/kg/day (16 times the MRHD based on body surface area), which was associated with increased pup deaths and decreased pup weights.
Lactation
Risk Summary
There are no data on the presence of daprodustat in human milk, the effects on the breastfed child, or the effects on milk production. Daprodustat is present in the milk of lactating rats (see Data) . When a drug is present in animal milk, it is likely that the drug will be present in human milk. Given the serious adverse reactions seen in adults treated with JESDUVROQ, such as thrombotic vascular events, advise patients not to breastfeed during treatment with JESDUVROQ, and for one week after the final dose.
Data
In a pre- and postnatal development study in rats, when daprodustat was orally administered to maternal rats during the lactation period, the drug was detected in plasma of suckling pups on postnatal day 10. The plasma concentration of daprodustat in pups was 2.3% to 3.7% of daprodustat detected in the plasma of dams when dosed at 40 mg/kg/day.
Pediatric Use
Safety and effectiveness of JESDUVROQ in pediatric patients have not been established.
Geriatric Use
Of the total number of subjects treated with JESDUVROQ in the ASCEND-D study (n = 2,964), 480 (32%) subjects were aged 65 years and older, and 159 (11%) were aged 75 years and older. No overall differences in safety or effectiveness were observed between these subjects and younger subjects. No other reported clinical experience has identified differences in responses between the elderly and younger patients.
Hepatic Impairment
No adjustment of the starting dose is required in patients with mild hepatic impairment (Child-Pugh Class A).
Reduce the starting dose of JESDUVROQ by half in patients with moderate hepatic impairment (Child-Pugh Class B) except in patients whose starting dose is already 1 mg [see Clinical Pharmacology (12.3 )] .
JESDUVROQ has not been studied in patients with severe hepatic impairment (Child-Pugh Class C). Therefore, JESDUVROQ is not recommended in patients with severe hepatic impairment.
WARNINGS AND PRECAUTIONS
- Risk of Hospitalization for Heart Failure: Increased in patients with a history of heart failure. (5.2 )
- Hypertension: Worsening hypertension, including hypertensive crisis may occur. Monitor blood pressure. Adjust anti-hypertensive therapy as needed. (5.3 )
- Gastrointestinal Erosion: Gastric or esophageal erosions and gastrointestinal bleeding have been reported. (5.4 )
- Not indicated for treatment of anemia of CKD in patients who are not dialysis-dependent (5.5 )
- Malignancy: May have unfavorable effects on cancer growth. Not recommended if active malignancy. (5.6 )
Increased Risk of Death, Myocardial Infarction, Stroke, Venous Thromboembolism, and Thrombosis of Vascular Access
JESDUVROQ increases the risk of arterial and venous thrombotic events, that may be fatal, including myocardial infarction, stroke, venous thromboembolism and vascular access thrombosis [see Boxed Warning, Adverse Reactions (6.1 )] . Patients with cardiovascular or cerebrovascular disease are at increased risk of these events. Avoid use in patients with a history of myocardial infarction, cerebrovascular event, or acute coronary syndrome within the 3 months prior to starting JESDUVROQ.
A rate of hemoglobin rise of greater than 1 g/dL over 2 weeks may contribute to these risks. Targeting a hemoglobin level of greater than 11 g/dL is expected to further increase the risk of death and arterial and venous thrombotic events, as occurs with ESAs, which also increase erythropoietin levels.
No trial has identified a hemoglobin target level, dose of JESDUVROQ, or dosing strategy that does not increase these risks. Use the lowest dose of JESDUVROQ sufficient to reduce the need for red blood transfusions. Adherence to dosing and hemoglobin monitoring recommendations is important to avoid excessive erythropoiesis [see Dosage and Administration (2.4 )] .
Advise patients to seek immediate medical attention if they develop signs or symptoms of myocardial infarction, stroke, venous thromboembolism, or thrombosis of vascular access. Evaluate and manage promptly if these occur.
Risk of Hospitalization for Heart Failure
In the ASCEND-D trial, hospitalization for heart failure was observed in 7.5% (3.3 per 100 Person Years [PY]) of patients on dialysis receiving JESDUVROQ and 6.8% (3.0 per 100 PY) of patients receiving recombinant human erythropoietin (rhEPO). Patients with a pre-existing history of heart failure were at increased risk of hospitalization for heart failure with JESDUVROQ (14.5%; 6.8 per 100 PY) compared to rhEPO (11.3%; 5.1 per 100 PY).
Consider the patient’s history of heart failure when deciding whether to prescribe JESDUVROQ. Advise patients of the symptoms and signs of heart failure and to immediately report any worsening to their healthcare provider.
Hypertension
JESDUVROQ is contraindicated in patients with uncontrolled hypertension. In the ASCEND-D trial, worsening of hypertension occurred in 24% (12 per 100 PY) of patients receiving JESDUVROQ and 24% (12 per 100 PY) of patients receiving rhEPO [see Adverse Reactions (6.1 )] . Serious worsening of hypertension occurred in 3.1% of patients receiving JESDUVROQ and 3.1% of patients receiving rhEPO. Cases of hypertensive crisis including hypertensive encephalopathy and seizures have also been reported in patients receiving JESDUVROQ. Periodically monitor blood pressure and adjust or initiate anti-hypertensive therapy as needed.
Gastrointestinal Erosion
In the ASCEND-D trial, gastric or esophageal erosions occurred in 5.7% (2.5 per 100 PY) of patients receiving JESDUVROQ and 6.6% (2.9 per 100 PY) of rhEPO-treated patients. Serious erosions, including gastrointestinal bleeding and the need for red blood cell transfusions, were reported in 3.6% and 3.1% of those receiving JESDUVROQ and rhEPO, respectively. Consider this risk particularly in patients at increased risk for gastrointestinal erosions, such as those with a history of gastrointestinal erosion, peptic ulcer disease, use of concomitant medications that increase the risk of gastrointestinal erosion, and current tobacco smokers and alcohol drinkers.
Advise patients of the symptoms and signs of gastric and esophageal erosions and of gastrointestinal bleeding and to seek prompt medical care if these occur.
Serious Adverse Events in Patients with Anemia Due to Chronic Kidney Disease and Not on Dialysis
The safety of JESDUVROQ has not been established for the treatment of anemia due to CKD in adults not on dialysis and its use is not recommended in this setting [see Indications and Usage (1 )] .
In a large cardiovascular outcomes trial in adults with anemia of CKD who were not on dialysis (ASCEND-ND), an increased risk of cardiovascular mortality, stroke, thromboembolism, serious acute kidney injury, hospitalization for heart failure, and serious gastrointestinal erosions was observed in patients treated with JESDUVROQ compared to rhEPO.
Malignancy
Because increased hypoxia inducible factor (HIF)-1 levels may be associated with unfavorable effects on cancer growth, JESDUVROQ has not been studied and is not recommended in patients with active malignancies. Malignancies were observed in 4.4% (1.9 per 100 PY) of patients treated with JESDUVROQ and 5.2% (2.3 per 100 PY) of patients treated with rhEPO. No evidence of increased carcinogenicity was observed in animal studies [see Nonclinical Toxicology (13.1 )] .
ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Increased Risk of Death, Myocardial Infarction, Stroke, Venous Thromboembolism, and Thrombosis of Vascular Access [see Boxed Warning, Warnings and Precautions (5.1 )] .
- Risk of Hospitalization for Heart Failure [see Warnings and Precautions (5.2 )] .
- Hypertension [see Warnings and Precautions (5.3 )] .
- Gastrointestinal Erosion [see Warnings and Precautions (5.4 )] .
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of JESDUVROQ was evaluated in adults with dialysis-dependent chronic kidney disease with anemia in the ASCEND-D trial based on an on-study analysis (on and off treatment) [see Clinical Studies (14.1 )] . Patients were randomized to JESDUVROQ or rhEPO (epoetin alfa for patients on hemodialysis; darbepoetin alfa for patients on peritoneal dialysis). Of the 2,964 patients randomized in the trial, 1,487 were randomized to JESDUVROQ, 1,316 (88.5%) of whom were on hemodialysis and 171 (11.5%) of whom were on peritoneal dialysis.
The median extent of exposure to JESDUVROQ and rhEPO was similar. In the JESDUVROQ treatment arm, 65% of the participants were exposed to at least 18 months of JESDUVROQ and 29% of participants received JESDUVROQ for at least 2.5 years.
JESDUVROQ was non-inferior to rhEPO on the time to first occurrence of major adverse cardiovascular events (MACE) in adults with anemia due to CKD who were on dialysis [see Clinical Studies (14.1 )] .
Permanent treatment discontinuation due to an adverse reaction was reported in 19% of patients treated with JESDUVROQ and 18% of patients treated with rhEPO. No specific adverse reaction resulted in permanent treatment discontinuation in >1% of patients treated with JESDUVROQ.
The most common adverse reactions (≥10% of JESDUVROQ-treated patients) were hypertension, thrombotic vascular events, and abdominal pain.
Table 4 lists the most common adverse reactions (reported in ≥5% of patients treated with JESDUVROQ).
Adverse Reaction | JESDUVROQ (n = 1,482) % | rhEPO (n = 1,474) % |
Hypertension | 24 | 24 |
Abdominal pain a | 11 | 8 |
Dizziness | 7 | 6 |
Hypersensitivity b | 7 | 7 |
rhEPO = Recombinant human erythropoietin.
a Includes unspecified abdominal pain, upper abdominal pain, abdominal discomfort.
b Includes rash, urticaria and dermatitis.
Thrombotic Vascular Events
Adjudicated thrombotic vascular events (fatal and non-fatal) were observed in 9.8 per 100 PY of patients receiving JESDUVROQ and in 11.7 per 100 PY of patients receiving rhEPO (see Table 5 ).
Event | JESDUVROQ (n = 1,482) | rhEPO (n = 1,474) |
Rate per 100 PY | Rate per 100 PY | |
Vascular access thrombosis | 5.0 | 6.3 |
Myocardial infarction | 3.4 | 4.1 |
Stroke | 1.2 | 1.5 |
Deep vein thrombosis | 0.7 | 0.6 |
Pulmonary embolism | 0.3 | 0.4 |
PY = Person Years; rhEPO = Recombinant human erythropoietin.
a These data are not an adequate basis for comparison of rates between the study drug and the active control.
DRUG INTERACTIONS
CYP2C8 Inhibitors
Concomitant administration of strong CYP2C8 inhibitors (e.g., gemfibrozil) with JESDUVROQ is contraindicated due to a marked increase in daprodustat exposure [see Contraindications (4 ), Clinical Pharmacology (12.3 )] . Concomitant administration of moderate CYP2C8 inhibitors (e.g., clopidogrel) increases daprodustat exposure [see Clinical Pharmacology (12.3 )] . Reduce the starting dose of JESDUVROQ by half when initiating treatment in patients on clopidogrel or a moderate CYP2C8 inhibitor except in patients whose starting dose is already 1 mg. Monitor hemoglobin and adjust the dose of JESDUVROQ when initiating or stopping therapy with clopidogrel or a moderate CYP2C8 inhibitor during treatment with JESDUVROQ [see Dosage and Administration (2.6 )] .
CYP2C8 Inducers
CYP2C8 inducers (e.g., rifampin) may decrease daprodustat exposure, which may result in loss of efficacy. Monitor hemoglobin and adjust the dose of JESDUVROQ when initiating or stopping therapy with CYP2C8 inducers during treatment with JESDUVROQ [see Clinical Pharmacology (12.3 )] .
DESCRIPTION
JESDUVROQ contains daprodustat, an inhibitor of hypoxia inducible factor (HIF), prolyl 4-hydroxylases (PH)1, PH2 and PH3. The chemical name of daprodustat is N‑[(1,3‑dicyclohexylhexahydro-2,4,6-trioxopyrimidin-5-yl) carbonyl]glycine. The molecular formula of daprodustat is C 19 H 27 N 3 O 6 , and its molecular mass is 393.43. The structural formula is shown below.
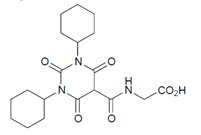
Daprodustat is a white to off-white powder that is poorly soluble in water.
Each JESDUVROQ oral tablet contains 1 mg, 2 mg, 4 mg, 6 mg, or 8 mg of daprodustat. Inactive ingredients include colloidal silicon dioxide, croscarmellose sodium, hypromellose, magnesium stearate, mannitol and microcrystalline cellulose. The tablet film-coating inactive ingredients include hypromellose, iron oxide black (1 mg, 2 mg, and 6 mg tablets), iron oxide red and iron oxide yellow (1 mg, 2 mg, 6 mg, and 8 mg tablets), polyethylene glycol, and titanium dioxide.
CLINICAL PHARMACOLOGY
Mechanism of Action
Daprodustat is a reversible inhibitor of HIF-PH1, PH2 and PH3 (IC 50 in the low nM range). This activity results in the stabilization and nuclear accumulation of HIF-1α and HIF-2α transcription factors, leading to increased transcription of the HIF-responsive genes, including erythropoietin.
Pharmacodynamics
Effects on Erythropoiesis
Daprodustat increases endogenous erythropoietin in a dose-dependent manner within 6 to 8 hours after administration. With repeat doses, peak increases in reticulocyte counts occur between 7 and 15 days, with subsequent increases in red blood cell production. New hemoglobin steady-state levels are reached several weeks (approximately 4 weeks in ESA-users and approximately 16-20 weeks in ESA-non-users) after initial administration.
Effects on Iron Metabolism and Utilization
Daprodustat increased serum transferrin and total iron binding capacity (TIBC) and decreased serum ferritin, transferrin saturation, and hepcidin when administered for 52 weeks in adults on dialysis with anemia due to CKD.
Cardiac Electrophysiology
At a dose 10 times the maximum recommended dose, daprodustat does not prolong the QTc interval to any clinically relevant extent.
Pharmacokinetics
Daprodustat exposure generally increases in a dose-proportional manner over the range of approved doses. Steady-state concentrations are achieved within 24-hours of dosing.
Absorption
Following oral administration, daprodustat is readily absorbed with median time to peak concentration (T max ) in healthy subjects ranging from 1 hour to 4 hours. The absolute bioavailability of daprodustat is 65%. Administration of JESDUVROQ with a high fat/high calorie meal did not significantly alter daprodustat exposure compared to administration in the fasted state.
Distribution
Daprodustat has an approximately equal distribution between plasma and blood cells (blood:plasma ratio of 1.23). Following intravenous dosing, the volume of distribution at steady-state in healthy subjects is 14.3 L. In vitro, plasma protein binding of daprodustat is >99%.
Elimination
The terminal elimination half-life of daprodustat is approximately 1 hour to 4 hours.
Metabolism: In vitro, daprodustat is primarily metabolized by CYP2C8 (95% contribution), with a minor contribution by CYP3A4 (5%).
Following oral or intravenous administration of radiolabeled daprodustat to healthy adults, approximately 40% of the total circulating radioactivity in plasma was daprodustat, and the remaining 60% was metabolites.
In patients treated with JESDUVROQ, the parent drug is the principal circulating component in plasma. Three metabolites, each accounting for more than 10% of circulating drug-related material, have been identified; in vitro and non-clinical data suggest that each may contribute to the pharmacologic response in vivo; however, the extent of this contribution is unknown.
Excretion: Mean clearance from plasma was 18.9 L/h, which correlates to blood clearance of 15 L/h and equates to a hepatic extraction of approximately 18%.
Within seven days of an oral dose of radiolabeled daprodustat, 74% of the radioactivity was recovered in the feces, and 21% in the urine. Approximately 99.5% of the dose was excreted as oxidative metabolites, with the rest accounted for by daprodustat.
Specific Populations
Elderly: Population pharmacokinetic analyses in adults with CKD (22 years to 93 years) showed that age did not influence the pharmacokinetics of daprodustat.
Renal Impairment: The steady-state exposure of daprodustat is similar in patients with normal renal function and those with varying degrees of renal impairment; daprodustat exposure is not significantly impacted by hemodialysis or peritoneal dialysis. The systemic exposure of daprodustat metabolites was higher in patients with Stage 3 to 5 CKD compared to those with normal renal function. Exposures of metabolites were higher on non-dialysis days compared to dialysis days.
Hepatic Impairment: Following administration of a single JESDUVROQ 6 mg dose, mean daprodustat C max and AUC increased by 2-fold and unbound exposure increased by 2.3-fold in subjects with moderate hepatic impairment (Child‑Pugh Class B) compared to subjects with normal hepatic and renal function. For those with mild hepatic impairment (Child‑Pugh Class A), mean daprodustat C max was similar while AUC increased by 1.5-fold and unbound C max and AUC increased by 1.6 and 2.2-fold, respectively, compared to subjects with normal hepatic and renal function. The effect of severe hepatic impairment (Child‑Pugh Class C) on the pharmacokinetics of daprodustat is unknown as there have been no studies of JESDUVROQ in patients with severe hepatic impairment.
Drug Interaction Studies
Clinical Studies: Effect of CYP2C8 Inhibitors on the Pharmacokinetics of Daprodustat: The concomitant administration of gemfibrozil 600 mg twice a day for 5 days (strong CYP2C8 inhibitor) with a single 100 mg dose of JESDUVROQ on Day 4 of gemfibrozil administration resulted in an 18.6‑fold increase in AUC (0-∞) and a 3.9-fold increase in C max of daprodustat [see Contraindications (4 )] .
The concomitant administration of trimethoprim 200 mg twice a day for 5 days (CYP2C8 weak inhibitor) and 25 mg single dose of JESDUVROQ on Day 4 of trimethoprim administration resulted in a 1.5-fold increase in AUC (0-∞) and a 1.3‑fold increase in C max of daprodustat.
Daprodustat AUC and C max are expected to increase at least 4-fold and 3-fold, respectively, following concomitant administration of daprodustat with clopidogrel 75 mg once daily (moderate CYP2C8 inhibitor).
Following 4 weeks of JESDUVROQ dosing, hemoglobin changes from baseline were similar in subjects with and without concomitant use of clopidogrel.
Effect of Daprodustat on the Pharmacokinetics of Other Drugs: Clinical drug interaction studies showed that daprodustat inhibition of CYP2C8 and OATP1B1/OATP1B3 demonstrated no clinically significant effect on pioglitazone (CYP2C8 substrate) or rosuvastatin (OATP1B1/OATP1B3 substrate) C max or AUC.
In vitro studies: Some oxidative metabolites of daprodustat are substrates of Organic Anion Transporter (OAT)1 or OAT3; however, the clinical significance of this is unknown. Daprodustat is a substrate of Breast Cancer Resistance Protein (BCRP); however, the risk of significant drug interactions between daprodustat and BCRP inhibitors is considered low given the absorption and metabolism profile of daprodustat.
Daprodustat is not an inducer of CYP1A2, CYP2B6 and CYP3A4. Daprodustat is not an inhibitor of P-glycoprotein (P-gp) and BCRP.
Daprodustat is not a substrate of CYP1A2, CYP2B6, CYP2C9, CYP2C19, CYP2D6 and P-gp. The major metabolites are not substrates of OATP1B1, OATP1B3, OATP2B1, Organic Cation Transporter (OCT)1, OCT2, Multidrug and Toxin Extrusion (MATE)1 and MATE2-K. Daprodustat and its major metabolites are not inhibitors of CYP1A2, CYP2A6, CYP2B6, CYP2C9, CYP2C19, CYP2D6, CYP3A4, OATP1B1, OATP1B3, OATP2B1, OCT1, OAT1, OAT3, OCT2, MATE1 and MATE2-K.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Daprodustat was not carcinogenic in two-year carcinogenicity studies when administered orally at doses of 0.02, 0.1, 0.8, or 4 mg/kg/day (males) / 7 mg/kg/day (females) in rats (up to 3 times the MRHD based on body surface area) and 0.2, 0.8, or 3 mg/kg/day (including subcutaneous injection of major human metabolites of daprodustat) in mice (approximating the MRHD based on body surface area).
Daprodustat was negative for mutagenic or clastogenic potential in the in vitro bacterial reverse mutation assay, the in vitro human lymphocyte chromosomal aberration assay, and the in vivo rat bone marrow micronucleus assay.
In a fertility and early embryonic development study in rats, daprodustat was administered orally at doses of 2, 7, or 100 mg/kg/day in females, resulting in maternal toxicity of reduced body weight gain and decreased mean uterine weight (in the presence of polycythemia), associated with decreased number of corpora lutea, implantations, and live fetuses, and increased post-implantation loss at the dose of 100 mg/kg/day (41 times the MRHD based on body surface area).
CLINICAL STUDIES
Anemia Due to Chronic Kidney Disease in Adults on Dialysis
The efficacy and safety of JESDUVROQ were evaluated in 2,964 adults with anemia due to CKD on dialysis and receiving an ESA at the time of study entry in a randomized, sponsor-blind, active-controlled, global, multicenter, event-driven clinical trial (ASCEND-D; NCT02879305). Patients were stratified by dialysis type and were required to be on dialysis for at least 4 months prior to the first dose of JESDUVROQ. Patients on hemodialysis (HD) were randomized 1:1 to receive oral JESDUVROQ (n = 1,316) or intravenous epoetin alfa (n = 1,308) while patients on peritoneal dialysis (PD) were randomized 1:1 to receive oral JESDUVROQ (n = 171) or subcutaneous darbepoetin alfa (n = 169).
Key exclusion criteria included: ferritin ≤100 ng/ml (≤100 mcg/L), transferrin saturation ≤20% at screening; evidence of non-renal anemia; cardiovascular abnormalities (including myocardial infarction, acute coronary syndrome, stroke or transient ischemic attack within 4 weeks of screening, New York Heart Association (NYHA) Class IV heart failure, and uncontrolled hypertension); liver disease; history of malignancy within 2 years of screening; current treatment of cancer and complex kidney cyst.
Dosing in each treatment arm followed a protocol-specified adjustment algorithm to achieve and/or maintain a hemoglobin target of 10 to 11 g/dL. The starting dose of JESDUVROQ was 4 mg, 6 mg, 8 mg, or 12 mg orally once daily, based on prior ESA dose. The starting dose of either epoetin alfa (HD patients) or darbepoetin alfa (PD patients) was the same as the patient’s current dose rounded to the nearest study dose. Patients receiving other ESAs were switched to the epoetin alfa or darbepoetin alfa equivalent starting dose. The median doses at Week 52 were 6 mg per day for JESDUVROQ, 8,000 units per week for epoetin alfa, and 150 mcg every four weeks for darbepoetin alfa. Most patients (86%) were exposed to randomized treatment for greater than 6 months (median 26 months for JESDUVROQ and 26 months for rhEPO). The median number of dose adjustments from Day 1 to Week 28 was 2 (interquartile range: 1 to 3) for JESDUVROQ and 2 (interquartile range: 1 to 3) for rhEPO. The median number of dose adjustments from Week 28 to Week 52 was 1 (interquartile range: 1 to 2) for JESDUVROQ and 2 (interquartile range: 1 to 3) for rhEPO.
The mean age of the patients in this study was 57 years (range 18-95), 57% were males, 67% were Caucasian, 16% were Black, and 12% were Asian. In the US region, 39% of patients were Black. Approximately 25% of the population was Hispanic or Latino. The largest regions of enrollment were the US (29%) and Eastern Europe/South Africa (28%). Common comorbid conditions included hypertension (92%), hyperlipidemia (50%) and diabetes mellitus (42%).
Effects on Hemoglobin
The efficacy and safety of JESDUVROQ were evaluated as co-primary endpoints: the mean change in hemoglobin from baseline to the Evaluation Period (Weeks 28 to 52) and time to first adjudicated MACE (defined as all-cause mortality, non-fatal myocardial infarction, or non-fatal stroke), using a non-inferiority comparison to rhEPO (epoetin alfa and darbepoetin alfa) for both endpoints.
The lower limit of the 95% confidence interval (CI) for the overall hemoglobin treatment difference was greater than the pre-specified non-inferiority margin of -0.75 g/dL, demonstrating non-inferiority of JESDUVROQ to rhEPO with respect to the mean change in hemoglobin between baseline and over the Evaluation Period (see Table 6 ). Results were similar in patients receiving either hemodialysis or peritoneal dialysis.
Assessment | JESDUVROQ (n = 1,487) | rhEPO b (n = 1,477) |
Primary endpoint: change in Hgb c | ||
| 10.4 (1.0) | 10.4 (1.0) |
| 0.3 (0.02) | 0.1 (0.02) |
| 0.2 (0.1, 0.2) | |
Change in Hgb - hemodialysis patients f | ||
| 1,316 | 1,308 |
| 10.4 (1.0) | 10.4 (1.0) |
| 0.3 (0.02) | 0.1 (0.02) |
| 0.2 (0.1, 0.3) | |
Change in Hgb - peritoneal dialysis patients f | ||
| 171 | 169 |
| 10.3 (1.0) | 10.2 (1.0) |
| 0.4 (0.1) | 0.2 (0.1) |
| 0.2 (-0.04, 0.3) | |
CI = Confidence interval; Hgb = Hemoglobin; ITT = Intent to treat; rhEPO = Recombinant human erythropoietin; SD = Standard deviation; SE = Standard error.
a Intent to Treat (ITT) analyses included observed and imputed values on and off treatment after randomization. Eight percent of patients had no observed hemoglobin during Weeks 28 to 52.
b Hemodialysis patients received epoetin alfa and peritoneal dialysis patients received darbepoetin alfa.
c Adjusted for multiplicity.
d Mean Hgb change from baseline to Evaluation Period (EP): Weeks 28 to 52.
e Adjusted for baseline covariates.
f Not adjusted for multiplicity.
Cardiovascular Outcomes
The hazard ratio for the time to first occurrence of MACE, a composite of all-cause mortality, non‑fatal myocardial infarction, and non-fatal stroke, comparing JESDUVROQ to rhEPO was 0.93 (95% CI 0.81, 1.07) (Table 7 ). Non-inferiority of JESDUVROQ to rhEPO on MACE was achieved because the upper limit of the 95% CI for the MACE hazard ratio was less than the pre‑specified non-inferiority margin of 1.25.
Co-primary composite endpoint | JESDUVROQ (n = 1,487) | rhEPO b (n = 1,477) |
First occurrence of MACE c , n | 374 | 394 |
| 244 | 233 |
| 101 | 126 |
| 29 | 35 |
Hazard ratio (95% CI) e | 0.93 (0.81, 1.07) | |
Incidence rate per 100 PY | 11.1 | 11.9 |
CI = Confidence interval; ITT = Intent to treat; MACE = Major adverse cardiovascular events; PY = Person Years; rhEPO = Recombinant human erythropoietin.
a ITT analyses included events on and off treatment after randomization.
b Hemodialysis patients received epoetin alfa; peritoneal dialysis patients received darbepoetin alfa.
c Co-primary endpoint.
d Component of composite endpoint.
e Adjusted for baseline covariates.
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
JESDUVROQ tablets contain 1 mg, 2 mg, 4 mg, 6 mg or 8 mg of daprodustat.
Tablet Strength | Package Configuration and NDC Number | Tablet Description and Markings |
1 mg | 30 count bottle (NDC 0173-0897-13) | Round, gray, biconvex, film-coated tablets debossed with “GS KF” on one side |
100 count blister pack (NDC 0173-0897-56) | ||
2 mg | 30 count bottle (NDC 0173-0903-13) | Round, yellow, biconvex, film-coated tablets debossed with “GS V7” on one side |
100 count blister pack (NDC 0173-0903-56) | ||
4 mg | 30 count bottle (NDC 0173-0906-13) | Round, white, biconvex, film-coated tablets debossed with “GS 13” on one side |
100 count blister pack (NDC 0173-0906-56) | ||
6 mg | 30 count bottle (NDC 0173-0911-13) | Round, pink, biconvex, film-coated tablets debossed with “GS IM” on one side |
100 count blister pack (NDC 0173-0911-56) | ||
8 mg | 30 count bottle (NDC 0173-0914-13) | Round, orange, biconvex, film-coated tablets debossed with “GS 5E” on one side |
100 count blister pack (NDC 0173-0914-56) |
Storage and Handling
Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C and 30°C (59°F to 86°F). [See USP Controlled Room Temperature].
Mechanism of Action
Daprodustat is a reversible inhibitor of HIF-PH1, PH2 and PH3 (IC 50 in the low nM range). This activity results in the stabilization and nuclear accumulation of HIF-1α and HIF-2α transcription factors, leading to increased transcription of the HIF-responsive genes, including erythropoietin.