Get your patient on Livdelzi (Seladelpar Lysine)
Livdelzi patient education
Patient toolkit
Dosage & administration

Livdelzi prescribing information
INDICATIONS AND USAGE
LIVDELZI is indicated for the treatment of primary biliary cholangitis (PBC) in combination with ursodeoxycholic acid (UDCA) in adults who have had an inadequate response to UDCA, or as monotherapy in patients unable to tolerate UDCA.
This indication is approved under accelerated approval based on a reduction of alkaline phosphatase (ALP) [see Clinical Studies (14) ] . Improvement in survival or prevention of liver decompensation events have not been demonstrated. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trial(s).
Limitations of Use
Use of LIVDELZI is not recommended in patients who have or develop decompensated cirrhosis (e.g., ascites, variceal bleeding, hepatic encephalopathy) [see Use in Specific Populations (8.7) ] .
DOSAGE AND ADMINISTRATION
The recommended dosage of LIVDELZI is 10 mg orally once daily. Administer LIVDELZI with or without food. (2.1 )
Recommended Dosage and Administration
The recommended dosage of LIVDELZI is 10 mg orally once daily. Administer LIVDELZI with or without food [see Clinical Pharmacology (12.3) ] .
Administration Modification for Bile Acid Sequestrants
Administer LIVDELZI at least 4 hours before or 4 hours after taking bile acid sequestrants, or at as great an interval as possible [see Drug Interactions (7.1) ] .
DOSAGE FORMS AND STRENGTHS
Capsules: 10 mg, opaque, hard gelatin capsules, size 1, with light gray opaque body and a dark blue opaque cap, printed with "CBAY" on the cap and "10" on the body.
USE IN SPECIFIC POPULATIONS
Hepatic Impairment: Monitor patients with cirrhosis for evidence of decompensation. Consider discontinuation if patient progresses to moderate or severe hepatic impairment (Child-Pugh B or C). (8.7 )
Pregnancy
Risk Summary
There are insufficient data from human pregnancies exposed to LIVDELZI to allow an assessment of a drug-associated risk of major birth defects, miscarriage, or other adverse maternal or fetal outcomes. In animal reproduction studies, no malformations or effects on embryo-fetal survival occurred in pregnant rats or rabbits after seladelpar treatment at exposures of up to 176-times and 49-times the recommended dose based on AUC (area under the plasma concentration-time curve), respectively. Reduction of fetal growth associated with maternal toxicity occurred in pregnant rabbits at 49-times the recommended dose based on AUC, but not at 3-times the recommended dose. In a pre- and postnatal development study in rats with maternal dosing of seladelpar during organogenesis through lactation, postnatal growth and pre-weaning survival of offspring was reduced at 115-times the recommended dose based on AUC, but not at the lower exposure of 16-times the recommended dose (see Data ) .
The background risks of major birth defects and miscarriage for the indicated population are unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Report pregnancies to Gilead Sciences, Inc. at 1-800-445-3235.
Data
Animal Data
No effects on embryo-fetal development were observed in pregnant rats treated orally with up to 100 mg/kg/day seladelpar (176-times the recommended dose based on AUC) during the period of organogenesis.
Oral administration of 40 mg/kg/day seladelpar in pregnant rabbits (49-times the recommended dose based on AUC) during organogenesis resulted in reduced fetal body weight, which was likely due to maternal toxicity (i.e., decreases in food consumption, body weight, and gravid uterine weight) and distended stomach. No treatment-related fetal malformations or effects on embryo-fetal survival occurred in rabbits at 49-times the recommended dose. No adverse effects on embryo-fetal development were observed at 10 mg/kg/day (3-times the recommended dose based on AUC).
A pre- and postnatal development study was performed using oral administration of seladelpar at doses of 0 (vehicle), 5, 20, or 100 mg/kg/day in pregnant rats during organogenesis through lactation. Treatment with 5 mg/kg/day or higher (4-times the recommended dose based on AUC) resulted in a dose-dependent reduction in pup body weight during the pre-weaning period. The weight reduction in offspring was associated with delays in developmental milestones (i.e., eye opening and pinna unfolding at 5 mg/kg/day and higher; hair growth and sexual maturity at 100 mg/kg/day). Reduction in pup body weight at 100 mg/kg/day (115-times the recommended dose based on AUC), which continued into the post-weaning maturation period, was associated with a slight decrease in pre-weaning survival and was considered adverse. No adverse effects were found in clinical observations, neurobehavioral assessment, or reproductive performance testing in the offspring of females treated with seladelpar. At 20 mg/kg/day (16-times the recommended dose based on AUC), none of the observed effects in offspring were considered to be adverse.
Lactation
Risk Summary
There are no data on the presence of seladelpar or its metabolite in either human or animal milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for LIVDELZI and any potential adverse effects on the breastfed infant from LIVDELZI or from the underlying maternal condition.
Pediatric Use
The safety and effectiveness of LIVDELZI in pediatric patients have not been established.
Geriatric Use
Of the 128 LIVDELZI-treated patients in Trial 1, 29 (23%) patients were 65 years of age and older and 2 (2%) were 75 years of age and older. No overall differences in safety or effectiveness were observed between patients 65 to 75 years of age and younger adult patients. No dosage adjustment for patients 65 years of age and older is necessary.
Clinical studies of LIVDELZI did not include sufficient numbers of patients 75 years of age and older to determine whether they respond differently from younger adult patients. Because of limited clinical experience with LIVDELZI in patients older than 75 years old, closer monitoring of adverse events in patients older than 75 years is recommended [see Clinical Pharmacology (12.3) ] .
Renal Impairment
The recommended dosage in patients with mild, moderate, or severe renal impairment is the same as in patients with normal renal function. Patients with end-stage renal disease on dialysis have not been studied [see Clinical Pharmacology (12.3) ] .
Hepatic Impairment
No dosage adjustment is recommended for PBC patients with mild hepatic impairment (Child-Pugh A) [see Clinical Pharmacology (12.3) ] .
The safety and efficacy of LIVDELZI in patients with decompensated cirrhosis have not been established. Use of LIVDELZI is not recommended in patients who have or develop decompensated cirrhosis (e.g., ascites, variceal bleeding, hepatic encephalopathy).
Monitor patients with cirrhosis for evidence of decompensation. Consider discontinuing LIVDELZI if the patient progresses to moderate or severe hepatic impairment (Child-Pugh B or C).
CYP2C9 Poor Metabolizers
Monitor CYP2C9 poor metabolizers who receive a concomitant moderate to strong CYP3A4 inhibitor more frequently for adverse reactions.
Seladelpar is a CYP2C9 and CYP3A4 substrate. Increased seladelpar AUC is expected in patients who are CYP2C9 poor metabolizers with concomitant use of a moderate to strong CYP3A4 inhibitor [see Drug Interactions (7.1) , Clinical Pharmacology (12.5) ] .
CONTRAINDICATIONS
None.
WARNINGS AND PRECAUTIONS
- Fractures : Consider the risk of fracture in patients treated with LIVDELZI. Monitor bone health according to current standards of care. (5.1 )
- Liver Test Abnormalities : Obtain baseline clinical and laboratory liver assessments prior to starting LIVDELZI and monitor during treatment. Interrupt or discontinue LIVDELZI if the liver tests worsen. (5.2 )
- Biliary Obstruction : Avoid use in patients with complete biliary obstruction. If biliary obstruction is suspected, interrupt LIVDELZI and treat as clinically indicated. (5.3 )
Fractures
Fractures occurred in 4% of LIVDELZI-treated patients compared to no placebo-treated patients [see Adverse Reactions (6.1) ] .
Consider the risk of fracture in the care of patients treated with LIVDELZI and monitor bone health according to current standards of care.
Liver Test Abnormalities
LIVDELZI has been associated with dose-related increases in serum transaminase (aspartate aminotransferase [AST] and alanine aminotransferase [ALT]) levels greater than 3-times upper limit of normal (ULN) in PBC patients receiving 50 mg once daily (5-times higher than the recommended dosage) and 200 mg (20-times higher than the recommended dosage) once daily. Transaminase levels returned to pretreatment levels upon LIVDELZI discontinuation. LIVDELZI 10 mg once daily did not show a similar pattern for increases in transaminase levels [see Overdosage (10) ] .
Obtain baseline clinical and laboratory assessments at treatment initiation with LIVDELZI and monitor thereafter according to routine patient management. Interrupt LIVDELZI treatment if the liver tests (ALT, AST, total bilirubin [TB], and/or alkaline phosphatase [ALP]) worsen, or the patient develops signs and symptoms consistent with clinical hepatitis (e.g., jaundice, right upper quadrant pain, eosinophilia). Consider permanent discontinuation if liver tests worsen after restarting LIVDELZI.
Biliary Obstruction
Avoid use of LIVDELZI in patients with complete biliary obstruction. If biliary obstruction is suspected, interrupt LIVDELZI and treat as clinically indicated.
ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in labeling:
- Fractures [see Warnings and Precautions (5.1) ]
- Liver Test Abnormalities [see Warnings and Precautions (5.2) ]
Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In Trial 1, 193 patients were randomized to receive either LIVDELZI 10 mg (N=128) or placebo (N=65) once daily for 12 months [see Clinical Studies (14) ] . LIVDELZI or placebo was administered in combination with UDCA in 94% of patients and as monotherapy in 6% of patients who were unable to tolerate UDCA.
Common Adverse Reactions
Table 1 presents common adverse reactions that occurred in Trial 1.
| Adverse Reaction Occurring in greater than or equal to 5% of patients in the LIVDELZI treatment arm and at an incidence greater than or equal to 1% higher than in the placebo arm. | LIVDELZI 10 mg Once Daily (N=128) % (n) | PLACEBO (N=65) % (n) |
|---|---|---|
| Headache | 8% (10) | 3% (2) |
| Abdominal pain The gastrointestinal adverse reactions were mild to moderate without the need for discontinuation of LIVDELZI. | 7% (9) | 2% (1) |
| Nausea | 6% (8) | 5% (3) |
| Abdominal distension | 6% (8) | 3% (2) |
| Dizziness | 5% (6) | 2% (1) |
Fractures
In Trial 1, fractures occurred in 4% (n=5) of LIVDELZI-treated patients compared to no placebo-treated patients. Baseline bone mineral density was not obtained. The median time to fracture after receiving LIVDELZI was 295 days (range: 89–349).
Less Common Adverse Reactions
Additional adverse reactions that occurred more frequently in the LIVDELZI-treated patients compared to placebo, but in less than 5% of patients, included dyspepsia, rash, alopecia, anemia, and cough.
Laboratory Abnormalities
Estimated Glomerular Filtration Rate
In Trial 1, LIVDELZI-treated patients developed decreased estimated glomerular filtration rate (eGFR) (serum creatinine elevations) more frequently compared to placebo-treated patients. Ten percent (n=12) of LIVDELZI-treated patients had a decline in eGFR of at least 25%, compared to 2% (n=1) of placebo-treated patients. None of the patients experienced an eGFR decline of 50% or more. The decline in eGFR stabilized or returned towards baseline with ongoing LIVDELZI treatment. None of the patients required discontinuation of LIVDELZI and there were no clinical findings associated with the observed changes in eGFR.
DRUG INTERACTIONS
- Probenecid : Avoid concomitant use. (7.1 )
- Strong CYP2C9 Inhibitors : Monitor for adverse effects. (7.1 )
- Dual Moderate CYP2C9 and Moderate to Strong CYP3A4 Inhibitors : Monitor for adverse effects. (7.1 )
- CYP2C9 Poor Metabolizers using Moderate to Strong CYP3A4 Inhibitors : Monitor for adverse effects. (7.1 )
- Dual or Multiple Clinical Inhibitors of Drug Transporters OATP1B1, OATP1B3, and BCRP : Monitor for adverse effects. (7.1 )
- Rifampin : Monitor biochemical response (e.g., ALP and bilirubin) when patients initiate rifampin. (7.1 )
- Bile Acid Sequestrants : Administer at least 4 hours before or 4 hours after taking a bile acid sequestrant, or at as great an interval as possible. (7.1 )
Effect of Other Drugs on LIVDELZI
Table 2 includes clinically significant drug interactions affecting LIVDELZI.
| Concomitant Drug or Class | Potential Effect on Seladelpar Exposure ↑ = Increase, ↓ = Decrease. | Clinical Intervention |
|---|---|---|
| Probenecid | ↑ seladelpar | Avoid concomitant administration of LIVDELZI with probenecid. |
| Strong CYP2C9 Inhibitors | ↑ seladelpar | Monitor patients for adverse effects during concomitant use of LIVDELZI with strong CYP2C9 inhibitors. |
| Dual Moderate CYP2C9 and Moderate or Strong CYP3A4 Inhibitors (e.g., fluconazole) | ↑ seladelpar | Monitor patients for adverse effects during concomitant use of LIVDELZI with drugs that are dual moderate CYP2C9 and moderate or strong CYP3A4 inhibitors. |
| CYP2C9 Poor Metabolizers Using Moderate or Strong CYP3A4 Inhibitors | ↑ seladelpar | Monitor patients who are CYP2C9 poor metabolizers for adverse effects during concomitant use of LIVDELZI with moderate or strong CYP3A4 inhibitor. |
| Dual or Multiple Clinical Inhibitors of Drug Transporters OATP1B1, OATP1B3, and BCRP (e.g, cyclosporine) | ↑ seladelpar | Monitor patients for adverse effects during concomitant use of LIVDELZI with dual or multiple clinical inhibitors of drug transporters OATP1B1, OATP1B3, and BCRP. |
| Rifampin | ↓ seladelpar | Concomitant use of LIVDELZI with rifampin, an inducer of metabolizing enzymes, may result in delayed or suboptimal LIVDELZI biochemical response. Monitor the biochemical response (e.g., ALP and bilirubin) when patients initiate rifampin during LIVDELZI treatment. |
| Bile Acid Sequestrants | ↓ seladelpar | Bile acid sequestrants may interfere with the action of LIVDELZI by reducing its absorption and systemic exposure, which may reduce LIVDELZI efficacy. Administer LIVDELZI at least 4 hours before or 4 hours after taking a bile acid sequestrant, or at as great an interval as possible [see Dosage and Administration (2.2) ] . |
DESCRIPTION
LIVDELZI capsules contain seladelpar lysine, a peroxisome proliferator-activated receptor (PPAR)-delta (δ) agonist. Seladelpar is a single enantiomer of the R-configuration and is present as a lysine dihydrate salt. Seladelpar lysine dihydrate is a white to off-white powder with a molecular formula of C 21 H 23 F 3 O 5 S ∙C 6 H 14 N 2 O 2 ∙2H 2 O and a molecular weight of 626.7 g/mol. Its solubility in water is pH dependent. It is slightly soluble at low pH and very soluble at high pH. The chemical name for seladelpar lysine dihydrate is 2-[4-[[(2R)-2-ethoxy-3-[4-(trifluoromethyl)phenoxy]propyl]thio]-2-methylphenoxy]acetic acid, lysine dihydrate, and the chemical structure is:
LIVDELZI (seladelpar) capsules are supplied in a 10 mg strength for oral administration. Each capsule contains 14.1 mg of seladelpar lysine and the following inactive ingredients: butylated hydroxytoluene, colloidal silicon dioxide, croscarmellose sodium, magnesium stearate, mannitol, microcrystalline cellulose, and hard gelatin shells.
The light gray opaque (body)/dark blue opaque (cap) capsule shells contain gelatin, titanium dioxide, black iron oxide, yellow iron oxide, red iron oxide and the colorant FD&C Blue #2.
CLINICAL PHARMACOLOGY
Mechanism of Action
Seladelpar is a peroxisome proliferator-activated receptor (PPAR)-delta (δ) agonist. However, the mechanism by which seladelpar exerts its therapeutic effects in patients with PBC is not well understood. Pharmacological activity that is potentially relevant to therapeutic effects includes inhibition of bile acid synthesis through activation of PPARδ, which is a nuclear receptor expressed in most tissues, including the liver. Published studies show that PPARδ activation by seladelpar reduces bile acid synthesis through Fibroblast Growth Factor 21 (FGF21)-dependent downregulation of CYP7A1, the key enzyme for the synthesis of bile acids from cholesterol.
Pharmacodynamics
Pharmacodynamic Markers
In patients with PBC treated with 10 mg once daily of LIVDELZI (Trial 1), a greater reduction in mean ALP from baseline was observed as early as 1 month after treatment compared to the placebo group and lower ALP was generally maintained through month 12 [see Clinical Studies (14) ] .
In another study in which patients with PBC were treated with 2, 5, or 10 mg once daily of seladelpar, a dose dependent reduction in mean ALP was observed.
Cardiac Electrophysiology
At 20-times the recommended dose of 10 mg, LIVDELZI did not cause clinically significant QTc interval prolongation.
Pharmacokinetics
Following a single dose administration, seladelpar systemic exposure increased dose-proportionally from 2 mg (0.2 times the recommended dosage) to 15 mg (1.5 times the recommended dosage) and greater than dose proportionally at higher doses. For a dose increase from 10 mg to 200 mg (20 times the recommended dosage), mean C max and mean AUC for seladelpar increased 70-fold and 27-fold, respectively.
Following once daily dosing, seladelpar steady-state was achieved by day 4 and AUC increase was less than 30%. In PBC patients, median (CV) C max and AUC for seladelpar was 90.5 (42.5%) ng/mL and 817 (44%) ng•h/mL, respectively at steady state following once daily dosing of 10 mg.
Absorption
The median time to peak concentration (T max ) was 1.5 hours for seladelpar.
Effect of Food
No clinically significant differences in seladelpar pharmacokinetics were observed following administration of a high-fat meal in healthy subjects.
Distribution
Seladelpar steady state apparent volume of distribution was approximately 110.3 L. Seladelpar plasma protein binding is greater than 99%.
Elimination
The apparent oral clearance of seladelpar is 12.6 L/h. Following administration of a single dose of 10 mg seladelpar in healthy subjects, mean elimination half-life was 6 hours for seladelpar. In PBC patients, the half-life range was 3.8 to 6.7 hours for seladelpar.
Metabolism
Seladelpar is primarily metabolized in vitro by CYP2C9 and to a lesser extent by CYP2C8 and CYP3A4, resulting in the three major metabolites: seladelpar sulfoxide (M1), desethyl-seladelpar (M2), and desethyl-seladelpar sulfoxide (M3). The metabolite-to-parent AUC ratios were 0.36, 2.32 and 0.63 for M1, M2 and M3, respectively. Median T max for metabolites were 10 hours for M1 and 4 hours for M2 and M3. None of the major metabolites have pharmacological activity.
Excretion
Seladelpar is primarily eliminated in urine as metabolites. Following a single oral dose of 10 mg radiolabeled seladelpar in humans, approximately 73.4% of the dose was recovered in urine (less than 0.01% unchanged) and 19.5% in feces (2.02% unchanged) within 216 hours. Biliary excretion of seladelpar was suggested by an animal study.
Specific Populations
No clinically significant differences in the pharmacokinetics of seladelpar were observed based on age (19 to 79 years old), body mass index (BMI) (17.6 to 45.0 kg/m 2 ), weight (45.8 to 127.5 kg), sex, and race (White, Black, or other).
Patients with Renal Impairment
In subjects with mild (eGFR ≥60 to <90 mL/min/1.73 m 2 , MDRD), moderate (eGFR ≥30 to <60 mL/min/1.73 m 2 ), and severe (<30 mL/min/1.73 m 2 and not on dialysis) renal impairment, the AUC inf of seladelpar was 10% higher, 54% higher, and similar to that in subjects with normal renal function, respectively, after administration of a single 10 mg dose of seladelpar. The difference in C max of seladelpar was less than 18% in subjects with renal impairment compared to subjects with normal renal function [see Use in Specific Populations (8.6) ] . The pharmacokinetics of seladelpar have not been studied in patients requiring hemodialysis.
Patients with Hepatic Impairment
Hepatic Impairment of various etiologies:Following a single oral dose of 10 mg seladelpar, seladelpar AUC increased 1.1-fold in subjects with mild (Child-Pugh A), 2.5-fold in moderate (Child-Pugh B), and 2.1-fold in severe (Child-Pugh C) hepatic impairment. Seladelpar C max increased 1.3-fold in subjects with mild (Child-Pugh A), 5.2-fold in moderate (Child-Pugh B), and 5-fold in severe (Child-Pugh C) hepatic impairment.
Hepatic Impairment in patients with PBC:Compared to PBC patients with mild hepatic impairment (Child-Pugh A) without portal hypertension, seladelpar exposures (C max , AUC) were 1.7 to 1.8-fold higher in PBC patients with mild hepatic impairment with portal hypertension, 1.6 to 1.9-fold higher in PBC patients with moderate hepatic impairment (Child-Pugh B), and 2.1 to 2.5-fold higher in PBC patients with severe hepatic impairment (Child-Pugh C) after a single oral dose of 10 mg seladelpar.
Accumulation ratios were less than 1.2-fold in PBC patients with mild hepatic impairment with portal hypertension and PBC patients with moderate hepatic impairment following 10 mg seladelpar once daily dosing for 28 days.
Drug Interaction Studies
Effect of Other Drugs on Seladelpar
Carbamazepine
Seladelpar AUC 0–inf decreased by approximately 44% and C max by 24% following administration of a single 10 mg seladelpar dose after carbamazepine 300 mg twice daily for 8 days in healthy subjects. The carbamazepine (CYP3A and CYP2C9 inducer) dose was escalated from 100 mg twice daily for 3 days followed by 200 mg twice daily for 4 days to 300 mg twice daily.
Fluconazole
Seladelpar AUC 0–inf increased by 2.4-fold and C max by 1.4-fold following concomitant use of a single 10 mg seladelpar dose with 400 mg fluconazole (moderate CYP2C9 and CYP3A4 inhibitor) in healthy subjects.
Cyclosporine
Seladelpar AUC 0–inf increased by 2.1-fold and C max by 2.9-fold following concomitant use of a single 10 mg seladelpar dose with 600 mg cyclosporine (OATP1B1, OATP1B3, and BCRP inhibitor) in healthy subjects.
Probenecid
Seladelpar AUC 0–inf increased by 2-fold and C max by 4.69-fold following concomitant use of a single 10 mg seladelpar dose with 500 mg probenecid in healthy subjects .
Quinidine
Seladelpar exposures were not significantly altered when a single dose of 600 mg quinidine (P-gp inhibitor) was coadministered in healthy subjects.
Other Drugs:No clinically significant differences in seladelpar pharmacokinetics were predicted when used concomitantly with strong CYP3A4 inhibitors or CYP2C8 inhibitors.
In Vitro Studies
Seladelpar is a substrate of CYP2C9, CYP2C8, CYP3A4, and the transporters BCRP, P-gp, OATP1B1, OATP1B3, and OAT3.
Seladelpar is not a substrate of MATE1, MATE2-K, OAT1, OCT1, or OCT2 transporters.
Effects of Seladelpar on other drugs
In clinical studies, no clinically significant differences in the pharmacokinetics of the following drugs were observed when used concomitantly with seladelpar: tolbutamide (CYP2C9 substrate), midazolam (CYP3A4 substrate), simvastatin (CYP3A4 and OATP substrate), atorvastatin (CYP3A4 and OATP substrate), or rosuvastatin (BCRP and OATP substrate).
In Vitro Studies
Based on in vitro studies, 10 mg seladelpar does not significantly affect the pharmacokinetics of concomitant drugs that are substrates of CYP enzymes (1A2, 2B6, 2C8, 2C19, 2D6, 3A4), UGTs, P-gp, MATEs, OCT1, OCT2, OAT1, or OAT3.
Pharmacogenomics
CYP2C9 activity is decreased in individuals with genetic variants such as CYP2C9•2 and CYP2C9•3. Compared to CYP2C9 normal metabolizers (•1/•1, n=84) after a single dose of seladelpar 1 mg to 15 mg, dose-normalized AUC 0–inf was 48% higher in CYP2C9 poor metabolizers (•2/•3, n=2) and 24% higher in CYP2C9 intermediate metabolizers (•1/•2, •1/•8, •1/•3, •2/•2, n=28). Dose-normalized C max was similar for CYP2C9 normal, intermediate, and poor metabolizers. Seladelpar pharmacokinetics was not evaluated in patients who are CYP2C9 poor metabolizers with two no function alleles (e.g., •3/•3). CYP2C9 poor metabolizers may have increased AUC when seladelpar is used concomitantly with a moderate to strong CYP3A4 inhibitor [see Drug Interactions (7.1) , Use in Specific Populations (8.8) ] .
The prevalence of CYP2C9 poor metabolizers is approximately 2 to 3% in White populations, 0.5 to 4% in Asian populations, and <1% in African American populations. Additional decreased or nonfunctional alleles (e.g., •5, •6, •11) are more prevalent in African American populations.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a 2-year study in CD-1 mice, oral administration of seladelpar produced hepatocellular adenoma or carcinoma at a dose of 5 mg/kg/day in males (6-times the recommended dose based on AUC) and 20 mg/kg/day in females (140-times the recommended dose based on AUC). No tumorigenic effects were observed in female mice at doses of up to 10 mg/kg/day (49-times the recommended dose based on AUC).
In a 2-year study in Sprague-Dawley rats, oral administration of seladelpar produced benign interstitial cell tumors in testes and squamous cell carcinoma of the nonglandular stomach in males at a dose of 30 mg/kg/day (79-times the recommended dose based on AUC). No tumorigenic effects were observed in males at doses of up to 10 mg/kg/day (14-times the recommended dose based on AUC) or in females at doses of up to 30 mg/kg/day (26-times the recommended dose based on AUC).
Mutagenesis
Seladelpar was negative in the in vitro bacterial reverse mutation (Ames) assay, the in vitro mouse lymphoma assay, and the in vivo mouse micronucleus test.
Impairment of Fertility
Seladelpar had no effects on fertility or reproductive function in male and female rats at oral doses of up to 100 mg/kg/day (271-times and 115-times the maximum recommended dose in male and female rats, respectively, based on AUC).
Animal Toxicology and/or Pharmacology
In a 2-year study in CD-1 mice, seladelpar produced an increased incidence of lens cataracts at 5 mg/kg/day in both sexes (6-times and 19-times the recommended dose in male and female mice, respectively, based on AUC). In a 2-year study in Sprague-Dawley rats, seladelpar produced an increased incidence of cornea inflammation at 10 mg/kg/day (14-times the recommended dose based on AUC) and cornea mineralization at 30 mg/kg/day (79-times the recommended dose based on AUC), with both effects observed in males only. The incidence of cornea inflammation was not increased in male rats at 3 mg/kg/day (5-times the recommended dose based on AUC).
CLINICAL STUDIES
The efficacy of LIVDELZI was evaluated in Trial 1 (NCT04620733), a 12-month, randomized, double-blind, placebo-controlled trial. The trial included 193 adult patients with PBC with an inadequate response or intolerance to UDCA. Patients were included in the trial if their ALP was greater than or equal to 1.67-times the ULN and total bilirubin (TB) was less than or equal to 2-times the ULN. Patients were excluded from the trial if they had other chronic liver diseases, clinically important hepatic decompensation including portal hypertension with complications, or cirrhosis with complications (e.g., Model for End Stage Liver Disease [MELD] score of 12 or greater, known esophageal varices or history of variceal bleeds, history of hepatorenal syndrome).
Patients were randomized to receive LIVDELZI 10 mg (N=128) or placebo (N=65) once daily for 12 months. LIVDELZI or placebo was administered in combination with UDCA in 181 (94%) patients during the trial, or as a monotherapy in 12 (6%) patients who were unable to tolerate UDCA.
Baseline Demographics and Characteristics
The mean age of patients was 57 (Range: 28 to 75) years; 95% were female; 88% were White, 6% Asian, 2% Black or African American, and 3% American Indian or Alaska Native. Twenty-nine percent of the patients, 23% in the LIVDELZI 10 mg arm and 42% in the placebo arm, identified as Hispanic/Latino. Thirty-two percent of the patients, 38% in the LIVDELZI 10 mg arm and 20% in the placebo arm, were enrolled in the US.
At baseline, 18 (14%) of the LIVDELZI-treated patients and 9 (14%) of the placebo-treated patients met at least one of the following criteria: Fibroscan >16.9kPa; historical biopsy or radiological evidence suggestive of cirrhosis; platelet count <140,000/µL with at least one additional laboratory finding including serum albumin <3.5 g/dL, INR >1.3, or TB > 1-time ULN; or clinical determination of cirrhosis by the investigator.
The mean baseline ALP concentration was 314 (Range: 161 to 786) units per liter (U/L), corresponding to 2.7-times ULN. The mean baseline TB concentration was 0.8 (Range: 0.3 to 1.9) mg/dL and was less than or equal to the ULN in 87% of the patients. Other mean baseline liver biochemistries were 48 (Range: 9 to 115) U/L for ALT and 40 (Range: 16 to 94) U/L for AST.
Biochemical Results
The primary endpoint was biochemical response at Month 12, where biochemical response was defined as achieving ALP less than 1.67-times ULN, an ALP decrease of greater than or equal to 15% from baseline, and TB less than or equal to ULN. ALP normalization (i.e., ALP less than or equal to ULN) at Month 12 was a key secondary endpoint. The ULN for ALP was defined as 116 U/L. The ULN for TB was defined as 1.1 mg/dL.
Table 3 presents results at Month 12 for the percentage of patients who achieved biochemical response, achieved each component of biochemical response, and achieved ALP normalization. LIVDELZI demonstrated greater improvement on biochemical response and ALP normalization at Month 12 compared to placebo. Overall, 87% of patients had a baseline of TB concentration less than or equal to ULN. Therefore, improvement in ALP was the main contributor to the biochemical response rate results at Month 12.
| LIVDELZI 10 mg Once Daily (N=128) | Placebo (N=65) | Treatment Difference % (95% CI) 95% unstratified Miettinen and Nurminen confidence intervals (CIs) are provided. | |
|---|---|---|---|
| Patients who discontinued treatment prior to Month 12 or who had missing data were considered as non-responders. | |||
| Biochemical Response Rate, n (%) , p<0.0001 for LIVDELZI 10 mg versus placebo. P-values were obtained using the Cochran–Mantel–Haenszel test stratified by baseline ALP level (<350 U/L versus ≥350 U/L) and baseline pruritus NRS (<4 versus ≥4). | 79 (62) | 13 (20) | 42 (28, 53) |
| Components of Biochemical Response | |||
| ALP less than 1.67-times ULN, n (%) | 84 (66) | 17 (26) | 39 (25, 52) |
| Decrease in ALP of at least 15%, n (%) | 107 (84) | 21 (32) | 51 (37, 63) |
| TB less than or equal to ULN, n (%) | 104 (81) | 50 (77) | 4 (-7, 17) |
| ALP Normalization, n (%) , ALP normalization is defined as ALP less than or equal to ULN. | 32 (25) | 0 (0) | 25 (18, 33) |
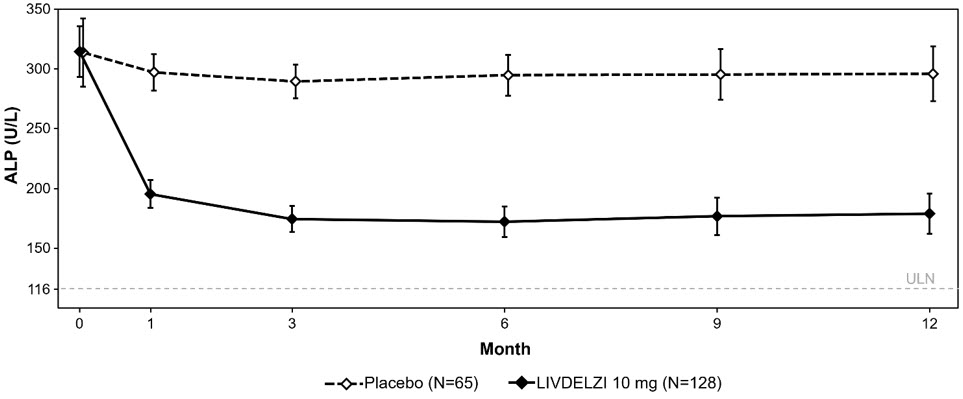
Figure 1 shows the mean (95% CI) levels of ALP over 12 months. There was a trend of lower ALP in LIVDELZI arm compared to placebo arm starting at Month 1 through Month 12.
| Figure 1: Mean Figure 1 presents means and 95% Wald CIs for baseline, and least squares means and corresponding 95% CIs based on a mixed-effect model for repeated measures (MMRM) for Months 1, 3, 6, 9 and 12. The MMRM adjusts for baseline ALP, baseline ALP level (<350 U/L versus ≥350 U/L), baseline pruritus NRS (<4 versus ≥4), time (in months), treatment arm, treatment-by-baseline ALP interaction, and treatment-by-time interaction. The least squares mean change from baseline in ALP at Month 12 was -134 (-151, -117) U/L and -17 (-40, 6) U/L in the LIVDELZI 10 mg and placebo arms, respectively. ALP in Adult Patients with PBC over 12 Months in Trial 1 |
 |
Biochemical response at Month 3 comparing LIVDELZI as a monotherapy to placebo was evaluated in a pooled analysis of a subset of patients from Trial 1 and another randomized, double-blind, placebo-controlled trial in a similar patient population. There was a trend of improvement on biochemical response at Month 3 in the LIVDELZI monotherapy group compared to the placebo group.
Pruritus
A single-item patient-reported outcome (PRO), the pruritus Numerical Rating Scale (NRS), evaluated patients' daily worst itching intensity on an 11-point rating scale with scores ranging from 0 ("no itching") to 10 ("worst itching imaginable") in Trial 1. The pruritus NRS was administered daily in a 14-day run-in period prior to randomization through Month 6.
Table 4 presents the results of the comparison between LIVDELZI and placebo on the key secondary endpoint evaluating the change from baseline in pruritus score at Month 6 in patients with baseline average pruritus scores greater than or equal to 4. The baseline average pruritus score for each patient was calculated by averaging the pruritus NRS scores administered in the run-in period and on Day 1 before treatment initiation. The pruritus scores at Month 6 for each patient were calculated by averaging the pruritus NRS scores within the last week in the month. Patients treated with LIVDELZI demonstrated greater improvement in pruritus compared with placebo.
| LIVDELZI 10 mg Once Daily (N=49) | Placebo (N=23) | |
|---|---|---|
| Baseline Average Pruritus Score, Mean (SD) | 6.1 (1.4) | 6.6 (1.4) |
| Change from Baseline in Pruritus Score at Month 6 | ||
| Mean (SE) | -3.2 (0.3) | -1.7 (0.4) |
| Mean difference vs. placebo (95% CI) | -1.5 (-2.5, -0.5) p=0.0051 | |
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
LIVDELZI (seladelpar) capsules are available as 10 mg, light gray opaque body, and a dark blue opaque cap with "CBAY" imprinted on the cap and "10" on the body.
LIVDELZI is packaged in a high density polyethylene bottle, closed with a polypropylene child resistant cap containing an induction seal.
- 10 mg capsules in a 75 cc bottle (30 count) (NDC 61958-3301-1).
- 10 mg capsules in a 60 cc bottle (30 count) (NDC 61958-3301-2).
Storage and Handling
Store at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) [s ee USP Controlled Room Temperature] .
Dispense only in original container to protect from light.
Mechanism of Action
Seladelpar is a peroxisome proliferator-activated receptor (PPAR)-delta (δ) agonist. However, the mechanism by which seladelpar exerts its therapeutic effects in patients with PBC is not well understood. Pharmacological activity that is potentially relevant to therapeutic effects includes inhibition of bile acid synthesis through activation of PPARδ, which is a nuclear receptor expressed in most tissues, including the liver. Published studies show that PPARδ activation by seladelpar reduces bile acid synthesis through Fibroblast Growth Factor 21 (FGF21)-dependent downregulation of CYP7A1, the key enzyme for the synthesis of bile acids from cholesterol.