Get your patient on Methylprednisolone Acetate - Methylprednisolone Acetate injection, Suspension (Methylprednisolone Acetate)
Methylprednisolone Acetate - Methylprednisolone Acetate injection, Suspension prescribing information
INDICATIONS AND USAGE
A. For Intramuscular Administration
When oral therapy is not feasible and the strength, dosage form, and route of administration of the drug reasonably lend the preparation to the treatment of the condition, the intramuscular use of methylprednisolone acetate injectable suspension is indicated as follows:
Allergic States : Control of severe or incapacitating allergic conditions intractable to adequate trials of conventional treatment in asthma, atopic dermatitis, contact dermatitis, drug hypersensitivity reactions, serum sickness, transfusion reactions.
Dermatologic Diseases : Bullous dermatitis herpetiformis, exfoliative erythroderma, mycosis fungoides, pemphigus, severe erythema multiforme (Stevens-Johnson syndrome).
Endocrine Disorders : Primary or secondary adrenocortical insufficiency (hydrocortisone or cortisone is the drug of choice; synthetic analogs may be used in conjunction with mineralocorticoids where applicable; in infancy, mineralocorticoid supplementation is of particular importance), congenital adrenal hyperplasia, hypercalcemia associated with cancer, nonsuppurative thyroiditis.
Gastrointestinal Diseases : To tide the patient over a critical period of the disease in regional enteritis (systemic therapy) and ulcerative colitis.
Hematologic Disorders : Acquired (autoimmune) hemolytic anemia, congenital (erythroid) hypoplastic anemia (Diamond Blackfan anemia), pure red cell aplasia, select cases of secondary thrombocytopenia.
Miscellaneous : Trichinosis with neurologic or myocardial involvement, tuberculous meningitis with subarachnoid block or impending block when used concurrently with appropriate antituberculous chemotherapy.
Neoplastic Diseases : For palliative management of leukemias and lymphomas.
Nervous System : Cerebral edema associated with primary or metastatic brain tumor or craniotomy.
Ophthalmic Diseases : Sympathetic ophthalmia, temporal arteritis, uveitis and ocular inflammatory conditions unresponsive to topical corticosteroids.
Renal Diseases : To induce diuresis or remission of proteinuria in idiopathic nephrotic syndrome, or that due to lupus erythematosus.
Respiratory Diseases : Berylliosis, fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate antituberculous chemotherapy, idiopathic eosinophilic pneumonias, symptomatic sarcoidosis.
Rheumatic Disorders : As adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in acute gouty arthritis; acute rheumatic carditis; ankylosing spondylitis; psoriatic arthritis; rheumatoid arthritis, including juvenile rheumatoid arthritis (selected cases may require low-dose maintenance therapy). For the treatment of dermatomyositis, polymyositis, and systemic lupus erythematosus.
B. For Intra-Articular or Soft Tissue Administration (see WARNINGS )
Methylprednisolone acetate injectable suspension is indicated as adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in acute gouty arthritis, acute and subacute bursitis, acute nonspecific tenosynovitis, epicondylitis, rheumatoid arthritis, synovitis of osteoarthritis.
C. For Intralesional Administration
Methylprednisolone acetate injectable suspension is indicated for intralesional use in alopecia areata, discoid lupus erythematosus, keloids, localized hypertrophic, infiltrated, inflammatory lesions of granuloma annulare, lichen planus, lichen simplex chronicus (neurodermatitis), and psoriatic plaques, necrobiosis lipoidica diabeticorum. Methylprednisolone acetate injectable suspension also may be useful in cystic tumors of an aponeurosis or tendon (ganglia).
DOSAGE AND ADMINISTRATION
NOTE: CONTAINS BENZYL ALCOHOL (see WARNINGS and PRECAUTIONS: Pediatric Use ).
Because of possible physical incompatibilities, methylprednisolone acetate injectable suspension should not be diluted or mixed with other solutions.
The initial dosage of parenterally administered methylprednisolone acetate injectable suspension will vary from 4 mg to 120 mg, depending on the specific disease entity being treated. However, in certain overwhelming, acute, life-threatening situations, administration in dosages exceeding the usual dosages may be justified and may be in multiples of the oral dosages.
It Should Be Emphasized that Dosage Requirements Are Variable and Must Be Individualized on the Basis of the Disease Under Treatment and the Response of the Patient. After a favorable response is noted, the proper maintenance dosage should be determined by decreasing the initial drug dosage in small decrements at appropriate time intervals until the lowest dosage which will maintain an adequate clinical response is reached. Situations which may make dosage adjustments necessary are changes in clinical status secondary to remissions or exacerbations in the disease process, the patient’s individual drug responsiveness, and the effect of patient exposure to stressful situations not directly related to the disease entity under treatment. In this latter situation, it may be necessary to increase the dosage of the corticosteroid for a period of time consistent with the patient’s condition. If after long-term therapy the drug is to be stopped, it is recommended that it be withdrawn gradually rather than abruptly.
A. Administration for Local Effect
Therapy with methylprednisolone acetate injectable suspension does not obviate the need for the conventional measures usually employed. Although this method of treatment will ameliorate symptoms, it is in no sense a cure and the hormone has no effect on the cause of the inflammation.
1. Rheumatoid Arthritis and Osteoarthritis : The dose for intra-articular administration depends upon the size of the joint and varies with the severity of the condition in the individual patient. In chronic cases, injections may be repeated at intervals ranging from one to five or more weeks, depending upon the degree of relief obtained from the initial injection. The doses in the following table are given as a general guide:
Size of Joint | Examples | Range of Dosage |
Large | Knees Ankles Shoulders | 20 mg to 80 mg |
Medium | Elbows Wrists | 10 mg to 40 mg |
Small | Metacarpophalangeal Interphalangeal Sternoclavicular Acromioclavicular | 4 mg to 10 mg |
Procedure : It is recommended that the anatomy of the joint involved be reviewed before attempting intra-articular injection. In order to obtain the full anti-inflammatory effect, it is important that the injection be made into the synovial space. Employing the same sterile technique as for a lumbar puncture, a sterile 20 to 24 gauge needle (on a dry syringe) is quickly inserted into the synovial cavity. Procaine infiltration is elective. The aspiration of only a few drops of joint fluid proves the joint space has been entered by the needle. The injection site for each joint is determined by that location where the synovial cavity is most superficial and most free of large vessels and nerves. With the needle in place, the aspirating syringe is removed and replaced by a second syringe containing the desired amount of methylprednisolone acetate injectable suspension. The plunger is then pulled outward slightly to aspirate synovial fluid and to make sure the needle is still in the synovial space. After injection, the joint is moved gently a few times to aid mixing of the synovial fluid and the suspension. The site is covered with a small sterile dressing.
Suitable sites for intra-articular injection are the knee, ankle, wrist, elbow, shoulder, phalangeal, and hip joints. Since difficulty is not infrequently encountered in entering the hip joint, precautions should be taken to avoid any large blood vessels in the area. Joints not suitable for injection are those that are anatomically inaccessible such as the spinal joints and those like the sacroiliac joints that are devoid of synovial space. Treatment failures are most frequently the result of failure to enter the joint space. Little or no benefit follows injection into surrounding tissue. If failures occur when injections into the synovial spaces are certain, as determined by aspiration of fluid, repeated injections are usually futile.
If a local anesthetic is used prior to injection of methylprednisolone acetate injectable suspension, the anesthetic package insert should be read carefully and all the precautions observed.
2. Bursitis : The area around the injection site is prepared in a sterile way and a wheal at the site made with 1 percent procaine hydrochloride solution. A 20 to 24 gauge needle attached to a dry syringe is inserted into the bursa and the fluid aspirated. The needle is left in place and the aspirating syringe changed for a small syringe containing the desired dose. After injection, the needle is withdrawn and a small dressing applied.
3. Miscellaneous: Ganglion, Tendinitis, Epicondylitis : In the treatment of conditions such as tendinitis or tenosynovitis, care should be taken following application of a suitable antiseptic to the overlying skin to inject the suspension into the tendon sheath rather than into the substance of the tendon. The tendon may be readily palpated when placed on a stretch. When treating conditions such as epicondylitis, the area of greatest tenderness should be outlined carefully and the suspension infiltrated into the area. For ganglia of the tendon sheaths, the suspension is injected directly into the cyst. In many cases, a single injection causes a marked decrease in the size of the cystic tumor and may effect disappearance. The usual sterile precautions should be observed, of course, with each injection.
The dose in the treatment of the various conditions of the tendinous or bursal structures listed above varies with the condition being treated and ranges from 4 mg to 30 mg. In recurrent or chronic conditions, repeated injections may be necessary.
4. Injections for Local Effect in Dermatologic Conditions : Following cleansing with an appropriate antiseptic such as 70% alcohol, 20 mg to 60 mg is injected into the lesion. It may be necessary to distribute doses ranging from 20 mg to 40 mg by repeated local injections in the case of large lesions. Care should be taken to avoid injection of sufficient material to cause blanching since this may be followed by a small slough. One to four injections are usually employed, the intervals between injections varying with the type of lesion being treated and the duration of improvement produced by the initial injection.
When multiple-dose vials are used, special care to prevent contamination of the contents is essential (see WARNINGS ).
B. Administration for Systemic Effect
The intramuscular dosage will vary with the condition being treated. When employed as a temporary substitute for oral therapy, a single injection during each 24-hour period of a dose of the suspension equal to the total daily oral dose of MEDROL ® Tablets (methylprednisolone tablets, USP) is usually sufficient. When a prolonged effect is desired, the weekly dose may be calculated by multiplying the daily oral dose by 7 and given as a single intramuscular injection.
In pediatric patients, the initial dose of methylprednisolone may vary depending upon the specific disease entity being treated. The range of initial doses is 0.11 mg/kg/day to 1.6 mg/kg/day. Dosage must be individualized according to the severity of the disease and response of the patient.
In patients with the adrenogenital syndrome , a single intramuscular injection of 40 mg every two weeks may be adequate. For maintenance of patients with rheumatoid arthritis , the weekly intramuscular dose will vary from 40 mg to 120 mg. The usual dosage for patients with dermatologic lesions benefited by systemic corticoid therapy is 40 mg to 120 mg of methylprednisolone acetate administered intramuscularly at weekly intervals for one to four weeks. In acute severe dermatitis due to poison ivy, relief may result within 8 to 12 hours following intramuscular administration of a single dose of 80 mg to 120 mg. In chronic contact dermatitis, repeated injections at 5 to 10 day intervals may be necessary. In seborrheic dermatitis, a weekly dose of 80 mg may be adequate to control the condition.
Following intramuscular administration of 80 mg to 120 mg to asthmatic patients, relief may result within 6 to 48 hours and persist for several days to two weeks.
If signs of stress are associated with the condition being treated, the dosage of the suspension should be increased. If a rapid hormonal effect of maximum intensity is required, the intravenous administration of highly soluble methylprednisolone sodium succinate is indicated.
For the purpose of comparison, the following is the equivalent milligram dose of the various glucocorticoids:
Cortisone, 25 | Triamcinolone, 4 |
Hydrocortisone, 20 | Paramethasone, 2 |
Prednisolone, 5 | Betamethasone, 0.75 |
Prednisone, 5 | Dexamethasone, 0.75 |
Methylprednisolone, 4 |
These dose relationships apply only to oral or intravenous administration of these compounds. When these substances or their derivatives are injected intramuscularly or into joint spaces, their relative properties may be greatly altered.
CONTRAINDICATIONS
Methylprednisolone acetate injectable suspension is contraindicated in patients with known hypersensitivity to the product and its constituents.
Intramuscular corticosteroid preparations are contraindicated for idiopathic thrombocytopenic purpura.
Methylprednisolone acetate injectable suspension is contraindicated for intrathecal administration. Reports of severe medical events have been associated with this route of administration.
Methylprednisolone acetate injectable suspension is contraindicated for use in premature infants because the formulation contains benzyl alcohol (see WARNINGS and PRECAUTIONS : Pediatric Use ).
Methylprednisolone acetate injectable suspension is contraindicated in systemic fungal infections, except when administered as an intra-articular injection for localized joint conditions (see WARNINGS: Immunosuppression and Increased Risk of Infection , Fungal Infections ).
ADVERSE REACTIONS
The following adverse reactions have been reported with methylprednisolone acetate or other corticosteroids:
Allergic reactions : Allergic or hypersensitivity reactions, anaphylactoid reaction, anaphylaxis, angioedema.
Blood and lymphatic system disorders : Leukocytosis.
Cardiovascular : Bradycardia, cardiac arrest, cardiac arrhythmias, cardiac enlargement, circulatory collapse, congestive heart failure, fat embolism, hypertension, hypertrophic cardiomyopathy in premature infants, myocardial rupture following recent myocardial infarction (see WARNINGS ), pulmonary edema, syncope, tachycardia, thromboembolism, thrombophlebitis, vasculitis.
Dermatologic : Acne, allergic dermatitis, cutaneous and subcutaneous atrophy, dry scaly skin, ecchymoses and petechiae, edema, erythema, hyperpigmentation, hypopigmentation, impaired wound healing, increased sweating, rash, sterile abscess, striae, suppressed reactions to skin tests, thin fragile skin, thinning scalp hair, urticaria.
Endocrine : Decreased carbohydrate and glucose tolerance, development of cushingoid state, glycosuria, hirsutism, hypertrichosis, increased requirements for insulin or oral hypoglycemic agents in diabetes, manifestations of latent diabetes mellitus, menstrual irregularities, secondary adrenocortical and pituitary unresponsiveness (particularly in times of stress, as in trauma, surgery, or illness), suppression of growth in pediatric patients.
Fluid and electrolyte disturbances : Congestive heart failure in susceptible patients, fluid retention, hypokalemic alkalosis, potassium loss, sodium retention.
Gastrointestinal : Abdominal distention, bowel/bladder dysfunction (after intrathecal administration), elevation in serum liver enzyme levels (usually reversible upon discontinuation), hepatomegaly, increased appetite, nausea, pancreatitis, peptic ulcer with possible subsequent perforation and hemorrhage, perforation of the small and large intestine (particularly in patients with inflammatory bowel disease), ulcerative esophagitis.
Metabolic : Negative nitrogen balance due to protein catabolism.
Musculoskeletal : Aseptic necrosis of femoral and humeral heads, calcinosis (following intra-articular or intralesional use), Charcot-like arthropathy, loss of muscle mass, muscle weakness, osteoporosis, pathologic fracture of long bones, post injection flare (following intra-articular, soft tissue, and tendon sheath injections), steroid myopathy, tendon rupture, vertebral compression fractures.
Neurologic/Psychiatric : Convulsions, depression, emotional instability, euphoria, headache, increased intracranial pressure with papilledema (pseudotumor cerebri) usually following discontinuation of treatment, insomnia, mood swings, neuritis, neuropathy, paresthesia, personality changes, psychic disorders, vertigo.
Ophthalmic : Exophthalmoses, glaucoma, increased intraocular pressure, posterior subcapsular cataracts.
Vascular: Flushing.
Other : Abnormal fat deposits, decreased resistance to infection, hiccups, increased or decreased motility and number of spermatozoa, injection site infections following non-sterile administration (see WARNINGS ), malaise, moon face, weight gain.
The following adverse reactions have been reported with the following routes of administration:
Intrathecal/Epidural : Arachnoiditis, bowel/bladder dysfunction, headache, meningitis, parapareisis/paraplegia, seizures, sensory disturbances.
Intranasal : Allergic reactions, rhinitis, temporary/permanent visual impairment including blindness.
Ophthalmic : Increased intraocular pressure, infection, ocular and periocular inflammation including allergic reactions, residue or slough at injection site, temporary/permanent visual impairment including blindness.
Miscellaneous injection sites ( scalp, tonsillar fauces, sphenopalatine ganglion): Blindness.
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Pharmaceuticals LLC at 1-877-835-5472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Aminoglutethimide : Aminoglutethimide may lead to a loss of corticosteroid-induced adrenal suppression.
Amphotericin B injection and potassium-depleting agents : When corticosteroids are administered concomitantly with potassium-depleting agents (e.g., amphotericin B, diuretics), patients should be observed closely for development of hypokalemia. There have been cases reported in which concomitant use of amphotericin B and hydrocortisone was followed by cardiac enlargement and congestive heart failure.
Antibiotics : Macrolide antibiotics have been reported to cause a significant decrease in corticosteroid clearance (see PRECAUTIONS : Drug Interactions , Hepatic Enzyme Inhibitors ).
Anticholinesterases : Concomitant use of anticholinesterase agents and corticosteroids may produce severe weakness in patients with myasthenia gravis. If possible, anticholinesterase agents should be withdrawn at least 24 hours before initiating corticosteroid therapy.
Anticoagulants, oral : Co-administration of corticosteroids and warfarin usually results in inhibition of response to warfarin, although there have been some conflicting reports. Therefore, coagulation indices should be monitored frequently to maintain the desired anticoagulant effect.
Antidiabetics : Because corticosteroids may increase blood glucose concentrations, dosage adjustments of antidiabetic agents may be required.
Antitubercular drugs : Serum concentrations of isoniazid may be decreased.
Cholestyramine : Cholestyramine may increase the clearance of oral corticosteroids.
Cyclosporine : Increased activity of both cyclosporine and corticosteroids may occur when the two are used concurrently. Convulsions have been reported with concurrent use.
Digitalis glycosides : Patients on digitalis glycosides may be at increased risk of arrhythmias due to hypokalemia.
Estrogens, including oral contraceptives : Estrogens may decrease the hepatic metabolism of certain corticosteroids, thereby increasing their effect.
Hepatic Enzyme Inducers (e.g., barbiturates, phenytoin, carbamazepine, rifampin) : Drugs which induce cytochrome P450 3A4 enzyme activity may enhance the metabolism of corticosteroids and require that the dosage of the corticosteroid be increased.
Hepatic Enzyme Inhibitors (e.g., ketoconazole, macrolide antibiotics such as erythromycin and troleandomycin) : Drugs which inhibit cytochrome P450 3A4 have the potential to result in increased plasma concentrations of corticosteroids.
Ketoconazole : Ketoconazole has been reported to significantly decrease the metabolism of certain corticosteroids by up to 60%, leading to an increased risk of corticosteroid side effects.
Nonsteroidal anti-inflammatory drugs (NSAIDs) : Concomitant use of aspirin (or other nonsteroidal anti-inflammatory agents) and corticosteroids increases the risk of gastrointestinal side effects. Aspirin should be used cautiously in conjunction with concurrent use of corticosteroids in hypoprothrombinemia. The clearance of salicylates may be increased with concurrent use of corticosteroids.
Skin Tests : Corticosteroids may suppress reactions to skin tests.
Vaccines : Patients on prolonged corticosteroid therapy may exhibit a diminished response to toxoids and live or attenuated vaccines due to inhibition of antibody response. Corticosteroids may also potentiate the replication of some organisms contained in live attenuated vaccines. Routine administration of vaccines or toxoids should be deferred until corticosteroid therapy is discontinued if possible (see WARNINGS: Immunosuppression and Increased Risk of Infection , Vaccinations ).
DESCRIPTION
Methylprednisolone acetate injectable suspension, USP is a sterile anti-inflammatory glucocorticoid for intramuscular, intra-articular, soft tissue, or intralesional injection. It is available in two strengths: 40 mg/mL and 80 mg/mL.
Each mL of these preparations contains:
Strengths | ||
40 mg/mL | 80 mg/mL | |
Active: | ||
Methylprednisolone acetate, USP | 40 mg | 80 mg |
Inactives: | ||
Polyethylene glycol 3350 | 29.1 mg | 28.2 mg |
Polysorbate 80 | 1.94 mg | 1.88 mg |
Monobasic sodium phosphate | 6.8 mg | 6.59 mg |
Dibasic sodium phosphate | 1.42 mg | 1.37 mg |
Benzyl alcohol (added as preservative) | 9.16 mg | 8.88 mg |
Water for injection | q.s. to 1 mL | q.s. to 1 mL |
Sodium chloride was added to adjust tonicity.
When necessary, pH was adjusted with sodium hydroxide and/or hydrochloric acid.
The pH of the finished product remains within the USP specified range (e.g., 5.5 to 6.8).
The chemical name for methylprednisolone acetate is pregna-1,4-diene-3,20-dione,21-(acetoxy)-11,17-dihydroxy-6-methyl,(6α,11ß) and the molecular weight is 416.51 g/mol. The structural formula is represented below:
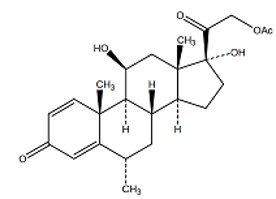
Molecular Formula: C 24 H 32 O 6
Methylprednisolone acetate injectable suspension USP, 400 mg/10 mL (40 mg/mL) and 400 mg/5 mL (80 mg/mL) contains methylprednisolone acetate, USP which is the 6-methyl derivative of prednisolone.
Methylprednisolone acetate, USP is a white or almost white, odorless, crystalline powder which melts at about 213°C with some decomposition. It is soluble in dioxane, sparingly soluble in acetone, alcohol, chloroform and methanol, and slightly soluble in ether. It is practically insoluble in water.
CLINICAL PHARMACOLOGY
Glucocorticoids, naturally occurring and synthetic, are adrenocortical steroids.
Naturally occurring glucocorticoids (hydrocortisone and cortisone), which also have salt retaining properties, are used in replacement therapy in adrenocortical deficiency states. Their synthetic analogs are used primarily for their anti-inflammatory effects in disorders of many organ systems.
Glucocorticoids cause profound and varied metabolic effects. In addition, they modify the body’s immune response to diverse stimuli.
HOW SUPPLIED
Methylprednisolone Acetate Injectable Suspension, USP is a sterile, white to off white homogeneous suspension and is available in the following strengths and package sizes:
400 mg/10 mL (40 mg/mL):
10 mL Multiple-Dose Vial in 1 Carton: NDC 70121-1609-1
25 Multiple-Dose Vials in 1 Carton: NDC 70121-1609-5
400 mg/5 mL (80 mg/mL):
5 mL Multiple-Dose Vial in 1 Carton: NDC 70121-1610-1
25 Multiple-Dose Vials in 1 Carton: NDC 70121-1610-5
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Shake well immediately before using.
This product’s label may have been updated. For current full prescribing information, please visit www.amneal.com.
All trademarks are the property of their respective owners.
For medical information about Methylprednisolone acetate injectable suspension, please visit www.amneal.com or call 1-877-835-5472.
Manufactured by: Amneal Pharmaceuticals Pvt. Ltd. Ahmedabad 382213, INDIA
Distributed by: Amneal Pharmaceuticals LLC Bridgewater, NJ 08807
Rev. 12-2025-05