Get your patient on Paxlovid (Nirmatrelvir And Ritonavir)
Paxlovid patient education
Patient toolkit
Dosage & administration

Paxlovid prescribing information
WARNING: SIGNIFICANT DRUG INTERACTIONS WITH PAXLOVID
- PAXLOVID includes ritonavir, a strong CYP3A inhibitor, which may lead to greater exposure of certain concomitant medications, resulting in potentially severe, life-threatening, or fatal events [see Contraindications (4) , Warnings and Precautions (5.1) , and Drug Interactions (7) ].
- Prior to prescribing PAXLOVID: 1) Review all medications taken by the patient to assess potential drug-drug interactions with a strong CYP3A inhibitor like PAXLOVID and 2) Determine if concomitant medications require a dose adjustment, interruption, and/or additional monitoring [see Drug Interactions (7) ].
- Consider the benefit of PAXLOVID treatment in reducing hospitalization and death, and whether the risk of potential drug-drug interactions for an individual patient can be appropriately managed [see Warnings and Precautions (5.1) , Drug Interactions (7) , and Clinical Studies (14) ].
Contraindications (4 ) | 02/2026 |
INDICATIONS AND USAGE
PAXLOVID is indicated for the treatment of mild-to-moderate coronavirus disease 2019 (COVID-19) in adults who are at high risk for progression to severe COVID-19, including hospitalization or death.
Limitations of Use
PAXLOVID is not approved for use as pre-exposure or post-exposure prophylaxis for prevention of COVID-19 [see Clinical Studies (14.3) ] .
DOSAGE AND ADMINISTRATION
PAXLOVID is nirmatrelvir tablets co-packaged with ritonavir tablets. (2.1 )
Nirmatrelvir must be co-administered with ritonavir. (2.1 )
- Initiate PAXLOVID treatment as soon as possible after diagnosis of COVID-19 and within 5 days of symptom onset. (2.1 )
- Administer orally with or without food. (2.1 )
- Administer at approximately the same time each day. (2.2 , 2.3 )
- Dosage: 300 mg nirmatrelvir (two 150 mg tablets) with 100 mg ritonavir (one 100 mg tablet), with all 3 tablets taken together twice daily for 5 days. (2.2 )
- Dose Reduction for Renal Impairment (2.3 , 8.6 , 12.3 )
| Abbreviation: eGFR=estimated glomerular filtration rate. | ||
| Days of Treatment |
|
|
|
|
|
|
|
|
| |
Important Dosage and Administration Information
PAXLOVID is nirmatrelvir tablets co-packaged with ritonavir tablets. There are three different dose packs available:
- PAXLOVID (nirmatrelvir; ritonavir) co-packaged for oral use 300 mg;100 mg [see Dosage and Administration (2.2) ] .
- PAXLOVID (nirmatrelvir; ritonavir) co-packaged for oral use 150 mg;100 mg for patients with moderate renal impairment [see Dosage and Administration (2.3) ].
- PAXLOVID (nirmatrelvir; ritonavir) co-packaged for oral use 300 mg;100 mg (Day 1) and 150 mg;100 mg (Days 2-5) for patients with severe renal impairment [see Dosage and Administration (2.3) ].
Nirmatrelvir must be co-administered with ritonavir. Failure to correctly co-administer nirmatrelvir with ritonavir may result in plasma levels of nirmatrelvir that are insufficient to achieve the desired therapeutic effect.
Prescriptions should specify the numeric dose of each active ingredient within PAXLOVID [see Dosage and Administration (2.2 , 2.3 )]. Completion of the full 5-day treatment course and continued isolation in accordance with public health recommendations are important to maximize viral clearance and minimize transmission of SARS-CoV-2.
The 5-day treatment course of PAXLOVID should be initiated as soon as possible after a diagnosis of COVID-19 has been made, and within 5 days of symptom onset even if baseline COVID-19 symptoms are mild. Should a patient require hospitalization due to severe or critical COVID-19 after starting treatment with PAXLOVID, the patient should complete the full 5-day treatment course per the healthcare provider's discretion.
If the patient misses a dose of PAXLOVID within 8 hours of the time it is usually taken, the patient should take it as soon as possible and resume the normal dosing schedule. If the patient misses a dose by more than 8 hours, the patient should not take the missed dose and instead take the next dose at the regularly scheduled time. The patient should not double the dose to make up for a missed dose.
PAXLOVID (both nirmatrelvir and ritonavir tablets) can be taken with or without food [see Clinical Pharmacology (12.3) ] . The tablets should be swallowed whole and not chewed, broken, or crushed.
Recommended Dosage
The recommended dosage for PAXLOVID is 300 mg nirmatrelvir (two 150 mg tablets) with 100 mg ritonavir (one 100 mg tablet) with all 3 tablets taken together orally twice daily in the morning and at bedtime for 5 days.
Dosage in Patients with Renal Impairment
Prescriptions should specify the numeric dose of each active ingredient within PAXLOVID. Providers should counsel patients about renal dosing instructions [see Patient Counseling Information (17) ].
No dosage adjustment is recommended in patients with mild renal impairment [estimated glomerular filtration rate (eGFR) ≥60 to <90 mL/min].
In patients with moderate renal impairment (eGFR ≥30 to <60 mL/min) or with severe renal impairment (eGFR <30 mL/min) including those requiring hemodialysis, the dosage of PAXLOVID should be reduced as shown in Table 1. PAXLOVID should be administered at approximately the same time each day for 5 days. On days patients with severe renal impairment undergo hemodialysis, the PAXLOVID dose should be administered after hemodialysis [see Use in Specific Populations (8.6) , Clinical Pharmacology (12.3) , and How Supplied/Storage and Handling (16) ] .
Table 1: Recommended Dose and Regimen for Patients with Renal Impairment
| Abbreviation: eGFR=estimated glomerular filtration rate. | ||
Renal Function | Days of Treatment | Dose and Dose Frequency PAXLOVID should be administered at approximately the same time each day for 5 days. |
Moderate renal impairment (eGFR ≥30 to <60 mL/min) | Days 1-5 | 150 mg nirmatrelvir (one 150 mg tablet) with 100 mg ritonavir (one 100 mg tablet) twice daily |
Severe renal impairment (eGFR <30 mL/min) including those requiring hemodialysis On days of hemodialysis, the PAXLOVID dose should be administered after hemodialysis. | Day 1 | 300 mg nirmatrelvir (two 150 mg tablets) with 100 mg ritonavir (one 100 mg tablet) once |
Days 2-5 | 150 mg nirmatrelvir (one 150 mg tablet) with 100 mg ritonavir (one 100 mg tablet) once daily | |
Use in Patients with Hepatic Impairment
No dosage adjustment is needed in patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment.
No pharmacokinetic or safety data are available regarding the use of nirmatrelvir or ritonavir in subjects with severe (Child-Pugh Class C) hepatic impairment; therefore, PAXLOVID is not recommended for use in patients with severe hepatic impairment [see Use in Specific Populations (8.7) ] .
DOSAGE FORMS AND STRENGTHS
PAXLOVID is nirmatrelvir tablets co-packaged with ritonavir tablets [see How Supplied/Storage and Handling (16) ] .
- Nirmatrelvir is supplied as oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Each tablet contains 150 mg of nirmatrelvir.
- Ritonavir is supplied as white or white to off-white film-coated tablets uniquely identified by the color, shape, and debossing. Each tablet contains 100 mg of ritonavir.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
Available data on the use of nirmatrelvir during pregnancy are insufficient to evaluate for a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Published observational studies on ritonavir use in pregnant women have not identified an increase in the risk of major birth defects. Published studies with ritonavir are insufficient to identify a drug associated risk of miscarriage (see Data ). There are maternal and fetal risks associated with untreated COVID-19 in pregnancy (see Clinical Considerations ).
In an embryo-fetal development study with nirmatrelvir, reduced fetal body weights following oral administration of nirmatrelvir to pregnant rabbits were observed at systemic exposures (AUC) approximately 11 times higher than clinical exposure at the approved human dose of PAXLOVID. No other adverse developmental outcomes were observed in animal reproduction studies with nirmatrelvir at systemic exposures (AUC) greater than or equal to 3 times higher than clinical exposure at the approved human dose of PAXLOVID (see Data ) .
In embryo-fetal developmental studies with ritonavir, no evidence of adverse developmental outcomes was observed following oral administration of ritonavir to pregnant rats and rabbits at systemic exposures (AUC) 5 (rat) or 8 (rabbits) times higher than clinical exposure at the approved human dose of PAXLOVID (see Data ) .
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated Maternal and/or Embryo-fetal Risk
COVID-19 in pregnancy is associated with adverse maternal and fetal outcomes, including preeclampsia, eclampsia, preterm birth, premature rupture of membranes, venous thromboembolic disease, and fetal death.
Data
Human Data
Ritonavir
Based on prospective reports to the antiretroviral pregnancy registry of live births following exposure to ritonavir-containing regimens (including over 3,500 live births exposed in the first-trimester and over 3,500 live births exposed in the second and third trimesters), there was no difference in the rate of overall birth defects for ritonavir compared with the background birth defect rate of 2.7% in the U.S. reference population of the Metropolitan Atlanta Congenital Defects Program (MACDP). The prevalence of birth defects in live births was 2.4% [95% confidence interval (CI): 1.9%, 2.9%] following first-trimester exposure to ritonavir-containing regimens and 2.9% (95% CI: 2.4%, 3.5%) following second and third trimester exposure to ritonavir-containing regimens. While placental transfer of ritonavir and fetal ritonavir concentrations are generally low, detectable levels have been observed in cord blood samples and neonate hair.
Animal Data
Nirmatrelvir
Embryo-fetal developmental (EFD) toxicity studies were conducted in pregnant rats and rabbits administered oral nirmatrelvir doses of up to 1,000 mg/kg/day during organogenesis [on Gestation Days (GD) 6 through 17 in rats and GD 7 through 19 in rabbits]. No biologically significant developmental effects were observed in the rat EFD study. At the highest dose of 1,000 mg/kg/day, the systemic nirmatrelvir exposure (AUC 24 ) in rats was approximately 9 times higher than clinical exposures at the approved human dose of PAXLOVID. In the rabbit EFD study, lower fetal body weights (9% decrease) were observed at 1,000 mg/kg/day in the absence of significant maternal toxicity findings. At 1,000 mg/kg/day, the systemic exposure (AUC 24 ) in rabbits was approximately 11 times higher than clinical exposures at the approved human dose of PAXLOVID. No other significant developmental toxicities (malformations and embryo-fetal lethality) were observed up to the highest dose tested, 1,000 mg/kg/day. No developmental effects were observed in rabbits at 300 mg/kg/day resulting in systemic exposure (AUC 24 ) approximately 3 times higher than clinical exposures at the approved human dose of PAXLOVID. A pre- and postnatal developmental (PPND) study in pregnant rats administered oral nirmatrelvir doses of up to 1,000 mg/kg/day from GD 6 through Lactation Day (LD) 20 showed no adverse findings. Although no difference in body weight was noted at birth when comparing offspring born to nirmatrelvir-treated versus control animals, a decrease in the body weight of offspring was observed on Postnatal Day (PND) 17 (8% decrease) and PND 21 (up to 7% decrease) in the absence of maternal toxicity. No significant differences in offspring body weight were observed from PND 28 to PND 56. The maternal systemic exposure (AUC 24 ) at 1,000 mg/kg/day was approximately 9 times higher than clinical exposures at the approved human dose of PAXLOVID. No body weight changes in the offspring were noted at 300 mg/kg/day, where maternal systemic exposure (AUC 24 ) was approximately 6 times higher than clinical exposures at the approved human dose of PAXLOVID.
Ritonavir
Ritonavir was administered orally to pregnant rats (at 0, 15, 35, and 75 mg/kg/day) and rabbits (at 0, 25, 50, and 110 mg/kg/day) during organogenesis (on GD 6 through 17 in rats and GD 6 through 19 in rabbits). No evidence of teratogenicity due to ritonavir was observed in rats and rabbits at systemic exposures (AUC) 5 (rats) or 8 (rabbits) times higher than exposure at the approved human dose of PAXLOVID. Increased incidences of early resorptions, ossification delays, and developmental variations, as well as decreased fetal body weights were observed in rats in the presence of maternal toxicity, at systemic exposures (AUC) approximately 10 times higher than exposure at the approved human dose of PAXLOVID. In rabbits, resorptions, decreased litter size, and decreased fetal weights were observed at maternally toxic doses, at systemic exposures greater than 8 times higher than exposure at the approved human dose of PAXLOVID. In a PPND study in rats, administration of 0, 15, 35, and 60 mg/kg/day ritonavir from GD 6 through PND 20 resulted in no developmental toxicity, at ritonavir systemic exposures greater than 10 times the exposure at the approved human dose of PAXLOVID.
Lactation
Risk Summary
Nirmatrelvir and ritonavir are present in human breast milk in small amounts (less than 2%). In a clinical lactation study in 8 lactating women, nirmatrelvir and ritonavir were estimated to be present in human milk at a mean weight-normalized infant daily dose of 0.16 mg/kg/day (1.8% of maternal weight-adjusted daily dose) and 0.006 mg/kg/day (0.2% of maternal weight-adjusted daily dose), respectively (see Data ) .
There are no available data on the effects of nirmatrelvir or ritonavir on the breastfed infant or on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for PAXLOVID and any potential adverse effects on the breastfed infant from PAXLOVID or from the underlying maternal condition. Breastfeeding individuals with COVID-19 should follow practices according to clinical guidelines to avoid exposing the infant to COVID-19.
Data
In a clinical pharmacokinetics study, 8 healthy lactating women who were at least 12 weeks postpartum were administered 3 oral doses every 12 hours (steady state dosing) of 300 mg/100 mg nirmatrelvir/ritonavir. The mean daily amount of nirmatrelvir and ritonavir recovered in breast milk was 0.752 mg and 0.027 mg, respectively, representing 0.13% and 0.014% of the corresponding administered daily maternal doses (unadjusted for weight). The estimated daily infant dose (assuming average milk consumption of 150 mL/kg/day), was 0.16 mg/kg/day and 0.006 mg/kg/day, 1.8% and 0.2% of the maternal dose, respectively, for nirmatrelvir and ritonavir.
Females and Males of Reproductive Potential
Contraception
Use of ritonavir may reduce the efficacy of combined hormonal contraceptives. Advise patients using combined hormonal contraceptives to use an effective alternative contraceptive method or an additional barrier method of contraception [see Drug Interactions (7.3) ] .
Pediatric Use
The optimal dose of PAXLOVID has not been established in pediatric patients.
Geriatric Use
Clinical studies of PAXLOVID include subjects 65 years of age and older and their data contributes to the overall assessment of safety and efficacy [see Adverse Reactions (6.1) and Clinical Studies (14.1) ] . Of the total number of subjects in the integrated dataset consisting of EPIC-HR and EPIC-SR who were randomized to and received PAXLOVID (N=1,578), 165 (10%) were 65 years of age and older and 39 (2%) were 75 years of age and older. No overall differences in safety were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in safety between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Renal Impairment
Renal impairment increases nirmatrelvir exposure, which may increase the risk of PAXLOVID adverse reactions. No dosage adjustment is recommended in patients with mild renal impairment (eGFR ≥60 to <90 mL/min). Reduce the PAXLOVID dosage in patients with moderate renal impairment (eGFR ≥30 to <60 mL/min). Reduce the PAXLOVID dose and dose frequency in patients with severe renal impairment (eGFR <30 mL/min), including those requiring hemodialysis. On days when patients undergo hemodialysis, the PAXLOVID dose should be administered after hemodialysis [see Dosage and Administration (2.3) , Adverse Reactions (6.1) , and Clinical Pharmacology (12.3) ]. Prescriptions should specify the numeric dose of each active ingredient within PAXLOVID. Providers should counsel patients about renal dosing instructions [see Patient Counseling Information (17) ] .
Hepatic Impairment
No dosage adjustment of PAXLOVID is recommended for patients with mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment. No pharmacokinetic or safety data are available regarding the use of nirmatrelvir or ritonavir in subjects with severe (Child-Pugh Class C) hepatic impairment, therefore, PAXLOVID is not recommended for use in patients with severe (Child-Pugh Class C) hepatic impairment [see Warnings and Precautions (5.3) and Clinical Pharmacology (12.3) ].
CONTRAINDICATIONS
PAXLOVID is contraindicated in patients with a history of clinically significant hypersensitivity reactions [e.g., toxic epidermal necrolysis (TEN) or Stevens-Johnson syndrome] to its active ingredients (nirmatrelvir or ritonavir) or any other components of the product.
PAXLOVID is contraindicated with drugs that are primarily metabolized by CYP3A and for which elevated concentrations are associated with serious and/or life-threatening reactions and drugs that are strong CYP3A inducers where significantly reduced nirmatrelvir or ritonavir plasma concentrations may be associated with the potential for loss of virologic response and possible resistance. There are certain other drugs for which concomitant use with PAXLOVID should be avoided and/or dose adjustment, interruption, or therapeutic monitoring is recommended. Drugs listed in this section are a guide and not considered a comprehensive list of all drugs that may be contraindicated with PAXLOVID. The healthcare provider should consult other appropriate resources such as the prescribing information for the interacting drug for comprehensive information on dosing or monitoring with concomitant use of a strong CYP3A inhibitor like PAXLOVID [see Drug Interactions (7.3) ] :
- Drugs that are primarily metabolized by CYP3A for which elevated concentrations are associated with serious and/or life-threatening reactions [see Drug Interactions (7.3) ] :
- Alpha 1-adrenoreceptor antagonist: alfuzosin
- Antianginal: ranolazine
- Antiarrhythmic: amiodarone, dronedarone, flecainide, propafenone, quinidine
- Anti-gout: colchicine (in patients with renal and/or hepatic impairment [see Table 2 , Drug Interactions (7.3)] )
- Antipsychotics: lurasidone, pimozide
- Benign prostatic hyperplasia agents: silodosin
- Cardiovascular agents: eplerenone, ivabradine
- Ergot derivatives: dihydroergotamine, ergotamine, methylergonovine
- HMG-CoA reductase inhibitors: lovastatin, simvastatin (these drugs can be temporarily discontinued to allow PAXLOVID use [see Table 2 , Drug Interactions (7.3) ] )
- Immunosuppressants: voclosporin
- Microsomal triglyceride transfer protein inhibitor: lomitapide
- Migraine medications: eletriptan, ubrogepant
- Mineralocorticoid receptor antagonists: finerenone
- Non-opioid analgesic (selective blocker of Na v 1.8 sodium channels): suzetrigine
- Opioid antagonists: naloxegol
- PDE5 inhibitor: sildenafil (Revatio ® ) when used for pulmonary arterial hypertension (PAH)
- Sedative/hypnotics: triazolam, oral midazolam
- Serotonin receptor 1A agonist/serotonin receptor 2A antagonist: flibanserin
- Vasopressin receptor antagonists: tolvaptan
- Drugs that are strong CYP3A inducers where significantly reduced nirmatrelvir or ritonavir plasma concentrations may be associated with the potential for loss of virologic response and possible resistance. PAXLOVID cannot be started immediately after discontinuation of any of the following medications due to the delayed offset of the recently discontinued CYP3A inducer [see Drug Interactions (7.3) ] :
- Anticancer drugs: apalutamide, enzalutamide
- Anticonvulsant: carbamazepine, phenobarbital, primidone, phenytoin
- Antimycobacterials: rifampin, rifapentine
- Cystic fibrosis transmembrane conductance regulator potentiators: lumacaftor/ivacaftor
- Herbal products: St. John's Wort ( hypericum perforatum )
WARNINGS AND PRECAUTIONS
- The concomitant use of PAXLOVID and certain other drugs may result in potentially significant drug interactions. Consult the Full Prescribing Information prior to and during treatment for potential drug interactions. (5.1 , 7 )
- Hypersensitivity Reactions: Anaphylaxis, serious skin reactions (including toxic epidermal necrolysis and Stevens-Johnson syndrome), and other hypersensitivity reactions have been reported with PAXLOVID. If signs and symptoms of a clinically significant hypersensitivity reaction or anaphylaxis occur, immediately discontinue PAXLOVID and initiate appropriate medications and/or supportive care. (5.2 )
- Hepatotoxicity: Hepatic transaminase elevations, clinical hepatitis, and jaundice have occurred in patients receiving ritonavir. (5.3 )
- HIV-1 Drug Resistance: PAXLOVID use may lead to a risk of HIV-1 developing resistance to HIV protease inhibitors in individuals with uncontrolled or undiagnosed HIV-1 infection. (5.4 )
Risk of Serious Adverse Reactions Due to Drug Interactions
Initiation of PAXLOVID, which contains ritonavir, a strong CYP3A inhibitor, in patients receiving medications metabolized by CYP3A or initiation of medications metabolized by CYP3A in patients already receiving PAXLOVID, may increase plasma concentrations of medications metabolized by CYP3A. Medications that induce CYP3A may decrease concentrations of PAXLOVID. These interactions may lead to:
- Clinically significant adverse reactions, potentially leading to severe, life-threatening, or fatal events from greater exposures of concomitant medications.
- Loss of therapeutic effect of PAXLOVID and possible development of viral resistance.
Severe, life-threatening, and/or fatal adverse reactions due to drug interactions have been reported in patients treated with PAXLOVID. The most commonly reported concomitant medications resulting in serious adverse reactions were calcineurin inhibitors (e.g., tacrolimus, cyclosporine), followed by calcium channel blockers.
Prior to prescribing PAXLOVID, review all medications taken by the patient to assess potential drug-drug interactions and determine if concomitant medications require a dose adjustment, interruption, and/or additional monitoring (e.g., calcineurin inhibitors) [see Contraindications (4) and Drug Interactions (7) ] . See Table 2 for clinically significant drug interactions, including contraindicated drugs. Drugs listed in Table 2 are a guide and not considered a comprehensive list of all possible drugs that may interact with PAXLOVID.
Consider the benefit of PAXLOVID treatment in reducing hospitalization and death, and whether the risk of potential drug-drug interactions for an individual patient can be appropriately managed [see Drug Interactions (7) and Clinical Studies (14) ] .
Hypersensitivity Reactions
Anaphylaxis, serious skin reactions (including toxic epidermal necrolysis and Stevens-Johnson syndrome), and other hypersensitivity reactions have been reported with PAXLOVID [see Adverse Reactions (6.1) ]. If signs and symptoms of a clinically significant hypersensitivity reaction or anaphylaxis occur, immediately discontinue PAXLOVID and initiate appropriate medications and/or supportive care.
Hepatotoxicity
Hepatic transaminase elevations, clinical hepatitis, and jaundice have occurred in patients receiving ritonavir. Therefore, caution should be exercised when administering PAXLOVID to patients with pre-existing liver diseases, liver enzyme abnormalities, or hepatitis.
Risk of HIV-1 Resistance Development
Because nirmatrelvir is co-administered with ritonavir, there may be a risk of HIV-1 developing resistance to HIV protease inhibitors in individuals with uncontrolled or undiagnosed HIV-1 infection [see Contraindications (4) and Drug Interactions (7) ] .
ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hypersensitivity reactions [see Warnings and Precautions (5.2) ]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of PAXLOVID is based on two Phase 2/3 randomized, placebo-controlled trials in symptomatic adult subjects 18 years of age and older with a laboratory confirmed diagnosis of SARS-CoV-2 infection. Subjects in both studies received PAXLOVID (nirmatrelvir/ritonavir 300 mg/100 mg) or placebo every 12 hours for 5 days for the treatment of mild-to-moderate COVID-19 within 5 days of symptom onset [see Clinical Studies (14) ] :
- Trial C4671005 (EPIC-HR) enrolled subjects who were at high risk for progression to severe disease.
- Trial C4671002 (EPIC-SR) enrolled subjects who were at standard risk for progression to severe disease (previously unvaccinated subjects at standard risk or fully vaccinated subjects with at least 1 risk factor for progression to severe disease).
Adverse reactions were those reported while subjects were on study medication and through 28 days after the last dose of study treatment.
In Trial C4671005 (EPIC-HR), 1,038 subjects received PAXLOVID and 1,053 subjects received placebo. The most common adverse reactions (≥1% incidence in the PAXLOVID group and occurring at a greater frequency than in the placebo group) were dysgeusia (5% and <1%, respectively) and diarrhea (3% and 2%, respectively).
Among vaccinated or unvaccinated subjects at standard risk or fully vaccinated subjects with at least 1 risk factor for progression to severe disease in Trial C4671002 (EPIC-SR), 540 subjects received PAXLOVID and 528 subjects received placebo. The adverse reactions observed were consistent with those observed in EPIC-HR.
Trial C4671028 (EPIC-SRI) was a Phase 1, open-label trial that evaluated the effects of severe renal impairment on the pharmacokinetics, safety, and tolerability of PAXLOVID in non-hospitalized adult participants with COVID-19 and severe renal impairment. A total of 15 subjects with severe renal impairment were enrolled in this trial, with 12 subjects receiving intermittent hemodialysis and 3 subjects not on hemodialysis. Subjects received nirmatrelvir/ritonavir 300 mg/100 mg once on Day 1 followed by nirmatrelvir/ritonavir 150 mg/100 mg once daily from Days 2-5. The safety profile of PAXLOVID in subjects with severe renal impairment, including those requiring hemodialysis, was consistent with the safety profile observed in the Phase 2/3 randomized, placebo-controlled trials.
Emergency Use Authorization Experience in Subjects with COVID-19
The following adverse reactions have been identified during use of PAXLOVID under Emergency Use Authorization.
Immune System Disorders: Anaphylaxis, hypersensitivity reactions [see Warnings and Precautions (5.2) ]
Skin and Subcutaneous Tissue Disorders: Toxic epidermal necrolysis, Stevens-Johnson syndrome [see Warnings and Precautions (5.2) ]
Nervous System Disorders: Headache
Vascular Disorders: Hypertension
Gastrointestinal Disorders: Abdominal pain, nausea, vomiting
General Disorders and Administration Site Conditions: Malaise
DRUG INTERACTIONS
Co-administration of PAXLOVID can alter the plasma concentrations of other drugs and other drugs may alter the plasma concentrations of PAXLOVID. Consider the potential for drug interactions prior to and during PAXLOVID therapy and review concomitant medications during PAXLOVID therapy. (4 , 5.1 , 7 , 12.3 )
Potential for PAXLOVID to Affect Other Drugs
PAXLOVID (nirmatrelvir co-packaged with ritonavir) is a strong inhibitor of CYP3A, and an inhibitor of CYP2D6, P-gp and OATP1B1. Co-administration of PAXLOVID with drugs that are primarily metabolized by CYP3A and CYP2D6 or are transported by P-gp or OATP1B1 may result in increased plasma concentrations of such drugs and increase the risk of adverse events. Co-administration of PAXLOVID with drugs highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening events is contraindicated [see Contraindications (4) and Drug Interactions (7.3) Table 2 ] . Co-administration with other CYP3A substrates may require a dose adjustment or additional monitoring as shown in Table 2.
Potential for Other Drugs to Affect PAXLOVID
Nirmatrelvir and ritonavir are CYP3A substrates; therefore, drugs that induce CYP3A may decrease nirmatrelvir and ritonavir plasma concentrations and reduce PAXLOVID therapeutic effect [see Contraindications (4) and Drug Interactions (7.3) Table 2 ] .
Established and Other Potentially Significant Drug Interactions
Table 2 provides a listing of clinically significant drug interactions, including contraindicated drugs [see Contraindications (4) and Warnings and Precautions (5.1) ] . Drugs listed in Table 2 are a guide and not considered a comprehensive list of all possible drugs that may interact with PAXLOVID. The healthcare provider should consult other appropriate resources such as the prescribing information for the interacting drug for comprehensive information on dosing or monitoring with concomitant use of a strong CYP3A inhibitor such as ritonavir.
| Drug Class | Drugs within Class | Effect on Concentration | Clinical Comments |
|---|---|---|---|
Alpha 1- adrenoreceptor antagonist | alfuzosin | ↑ alfuzosin | Co-administration contraindicated due to potential hypotension [see Contraindications (4) ] . |
Alpha 1- adrenoreceptor antagonist | tamsulosin | ↑ tamsulosin | Avoid concomitant use with PAXLOVID. |
Antianginal | ranolazine | ↑ ranolazine | Co-administration contraindicated due to potential for serious and/or life-threatening reactions [see Contraindications (4) ] . |
Antiarrhythmics | amiodarone, dronedarone, flecainide, propafenone, quinidine | ↑ antiarrhythmic | Co-administration contraindicated due to potential for cardiac arrhythmias [see Contraindications (4) ] . |
Antiarrhythmics | lidocaine (systemic), disopyramide | ↑ antiarrhythmic | Caution is warranted and therapeutic concentration monitoring is recommended for antiarrhythmics if available. |
Anticancer drugs | apalutamide, enzalutamide | ↓ nirmatrelvir/ritonavir | Co-administration contraindicated due to potential loss of virologic response and possible resistance [see Contraindications (4) ]. |
Anticancer drugs | abemaciclib, ceritinib, dasatinib, encorafenib, ibrutinib, ivosidenib, neratinib, nilotinib, venetoclax, vinblastine, vincristine | ↑ anticancer drugs | Avoid co-administration of encorafenib or ivosidenib due to potential risk of serious adverse events such as QT interval prolongation. Avoid use of neratinib, venetoclax or ibrutinib. Co-administration of vincristine and vinblastine may lead to significant hematologic or gastrointestinal side effects. For further information, refer to the individual product prescribing information for anticancer drug. |
Anticoagulants | warfarin | ↑↓ warfarin | Closely monitor international normalized ratio (INR) if co-administration with warfarin is necessary. |
rivaroxaban | ↑ rivaroxaban | Increased bleeding risk with rivaroxaban. Avoid concomitant use. | |
dabigatran See Pharmacokinetics, Clinical Drug Interaction Studies (12.3) . | ↑ dabigatran | Increased bleeding risk with dabigatran. Depending on dabigatran indication and renal function, reduce dose of dabigatran or avoid concomitant use. Refer to the dabigatran prescribing information for further information. | |
apixaban | ↑ apixaban | Combined P-gp and strong CYP3A inhibitors increase blood levels of apixaban and increase the risk of bleeding. Dosing recommendations for co-administration of apixaban with PAXLOVID depend on the apixaban dose. Refer to the apixaban prescribing information for more information. | |
Anticonvulsants | carbamazepine, phenobarbital, primidone, phenytoin | ↓ nirmatrelvir/ritonavir | Co-administration contraindicated due to potential loss of virologic response and possible resistance [see Contraindications (4) ] . |
Anticonvulsants | clonazepam | ↑ anticonvulsant | A dose decrease may be needed for clonazepam when co-administered with PAXLOVID and clinical monitoring is recommended. |
Antidepressants | bupropion | ↓ bupropion and active metabolite hydroxy-bupropion | Monitor for an adequate clinical response to bupropion. |
trazodone | ↑ trazodone | Adverse reactions of nausea, dizziness, hypotension, and syncope have been observed following co-administration of trazodone and ritonavir. A lower dose of trazodone should be considered. Refer to the trazadone prescribing information for further information. | |
Antifungals | voriconazole | ↓ voriconazole | Avoid concomitant use of voriconazole. |
ketoconazole, isavuconazonium sulfate, itraconazole | ↑ ketoconazole ↑ isavuconazonium sulfate ↑ itraconazole | Refer to the ketoconazole, isavuconazonium sulfate, and itraconazole prescribing information for further information. | |
↑ nirmatrelvir/ritonavir | A nirmatrelvir/ritonavir dose reduction is not needed. | ||
Anti-gout | colchicine | ↑ colchicine | Co-administration contraindicated due to potential for serious and/or life-threatening reactions in patients with renal and/or hepatic impairment [see Contraindications (4) ] . |
Anti-HIV protease inhibitors | atazanavir, darunavir, tipranavir | ↑ protease inhibitor | For further information, refer to the respective protease inhibitors' prescribing information. Patients on ritonavir- or cobicistat-containing HIV regimens should continue their treatment as indicated. Monitor for increased PAXLOVID or protease inhibitor adverse events . |
Anti-HIV | efavirenz, maraviroc, nevirapine, zidovudine, bictegravir/ emtricitabine/ tenofovir | ↑ efavirenz ↑ maraviroc ↑ nevirapine ↓ zidovudine ↑ bictegravir ↔ emtricitabine ↑ tenofovir | For further information, refer to the respective anti-HIV drugs prescribing information. |
Anti-infective | clarithromycin, erythromycin | ↑ clarithromycin ↑ erythromycin | Refer to the respective prescribing information for anti-infective dose adjustment. |
Antimycobacterial | rifampin, rifapentine | ↓ nirmatrelvir/ritonavir | Co-administration contraindicated due to potential loss of virologic response and possible resistance. Alternate antimycobacterial drugs such as rifabutin should be considered [see Contraindications (4) ] . |
Antimycobacterial | bedaquiline | ↑ bedaquiline | Refer to the bedaquiline prescribing information for further information. |
rifabutin | ↑ rifabutin | Refer to the rifabutin prescribing information for further information on rifabutin dose reduction. | |
Antipsychotics | lurasidone, pimozide | ↑ lurasidone ↑ pimozide | Co-administration contraindicated due to serious and/or life-threatening reactions such as cardiac arrhythmias [see Contraindications (4) ] . |
Antipsychotics | quetiapine | ↑ quetiapine | If co-administration is necessary, reduce quetiapine dose and monitor for quetiapine-associated adverse reactions. Refer to the quetiapine prescribing information for recommendations. |
clozapine | ↑ clozapine | If co-administration is necessary, consider reducing the clozapine dose and monitor for adverse reactions. | |
Benign prostatic hyperplasia agents | silodosin | ↑ silodosin | Co-administration contraindicated due to potential for postural hypotension [see Contraindications (4) ] . |
Calcium channel blockers | amlodipine, diltiazem, felodipine, nicardipine, nifedipine, verapamil | ↑ calcium channel blocker | Caution is warranted and clinical monitoring of patients is recommended. A dose decrease may be needed for these drugs when co-administered with PAXLOVID. If co-administered, refer to the individual product prescribing information for calcium channel blocker for further information. |
Cardiac glycosides | digoxin | ↑ digoxin | Caution should be exercised when co-administering PAXLOVID with digoxin, with appropriate monitoring of serum digoxin levels. Refer to the digoxin prescribing information for further information. |
Cardiovascular agents | eplerenone | ↑ eplerenone | Co-administration with eplerenone is contraindicated due to potential for hyperkalemia [see Contraindications (4) ] . |
ivabradine | ↑ ivabradine | Co-administration with ivabradine is contraindicated due to potential for bradycardia or conduction disturbances [see Contraindications (4) ] . | |
Cardiovascular agents | aliskiren, ticagrelor, vorapaxar clopidogrel | ↑ aliskiren ↑ ticagrelor ↑ vorapaxar ↓ clopidogrel active metabolite | Avoid concomitant use with PAXLOVID. |
cilostazol | ↑ cilostazol | Dosage adjustment of cilostazol is recommended. Refer to the cilostazol prescribing information for more information. | |
mavacamten | ↑ mavacamten | Co-administration with mavacamten may increase mavacamten plasma concentration and increase the risk of heart failure. Discontinue mavacamten for the duration of PAXLOVID treatment. Resumption of mavacamten within 5 days of completing PAXLOVID may result in higher exposure of mavacamten. Refer to the mavacamten prescribing information for more information. | |
Corticosteroids primarily metabolized by CYP3A | betamethasone, budesonide, ciclesonide, dexamethasone, fluticasone, methylprednisolone, mometasone, triamcinolone | ↑ corticosteroid | Co-administration with corticosteroids (all routes of administration) of which exposures are significantly increased by strong CYP3A inhibitors can increase the risk for Cushing’s syndrome and adrenal suppression. However, the risk of Cushing’s syndrome and adrenal suppression associated with short-term use of a strong CYP3A inhibitor is low. Alternative corticosteroids including beclomethasone, prednisone, and prednisolone should be considered. |
Cystic fibrosis transmembrane conductance regulator potentiators | lumacaftor/ivacaftor | ↓ nirmatrelvir/ritonavir | Co-administration contraindicated due to potential loss of virologic response and possible resistance [see Contraindications (4) ] . |
Cystic fibrosis transmembrane conductance regulator potentiators | ivacaftor elexacaftor/tezacaftor/ ivacaftor tezacaftor/ivacaftor | ↑ ivacaftor ↑ elexacaftor/tezacaftor/ ivacaftor ↑ tezacaftor/ivacaftor | Reduce dosage when co-administered with PAXLOVID. Refer to the individual product prescribing information for more information. |
Dipeptidyl peptidase 4 (DPP4) inhibitors | saxagliptin | ↑ saxagliptin | Dosage adjustment of saxagliptin is recommended. Refer to the saxagliptin prescribing information for more information. |
Endothelin receptor antagonists | bosentan | ↑ bosentan ↓ nirmatrelvir/ritonavir | Discontinue use of bosentan at least 36 hours prior to initiation of PAXLOVID. Refer to the bosentan prescribing information for further information. |
Ergot derivatives | dihydroergotamine, ergotamine, methylergonovine | ↑ dihydroergotamine ↑ ergotamine ↑ methylergonovine | Co-administration contraindicated due to potential for acute ergot toxicity characterized by vasospasm and ischemia of the extremities and other tissues including the central nervous system [see Contraindications (4) ] . |
Hepatitis C direct acting antivirals | elbasvir/grazoprevir | ↑ antiviral | Increased grazoprevir concentrations can result in alanine transaminase (ALT) elevations. |
glecaprevir/pibrentasvir | Avoid concomitant use of glecaprevir/pibrentasvir with PAXLOVID. | ||
ombitasvir/paritaprevir/ritonavir and dasabuvir | Refer to the ombitasvir/paritaprevir/ritonavir and dasabuvir label for further information. | ||
sofosbuvir/velpatasvir/voxilaprevir | Refer to the sofosbuvir/velpatasvir/voxilaprevir prescribing information for further information. Patients on ritonavir-containing HCV regimens should continue their treatment as indicated. Monitor for increased PAXLOVID or HCV drug adverse events with concomitant use . | ||
Herbal products | St. John's Wort ( hypericum perforatum ) | ↓ nirmatrelvir/ritonavir | Co-administration contraindicated due to potential loss of virologic response and possible resistance [see Contraindications (4) ] . |
HMG-CoA reductase inhibitors | lovastatin, simvastatin | ↑ lovastatin ↑ simvastatin | Co-administration contraindicated due to potential for myopathy including rhabdomyolysis [see Contraindications (4) ] . If treatment with PAXLOVID is considered medically necessary, discontinue use of lovastatin and simvastatin at least 12 hours prior to initiation of PAXLOVID, during the 5 days of PAXLOVID treatment, and for 5 days after completing PAXLOVID. |
HMG-CoA reductase inhibitors | atorvastatin | ↑ atorvastatin | Consider temporary discontinuation of atorvastatin during treatment with PAXLOVID. Atorvastatin does not need to be withheld prior to or after completing PAXLOVID. |
Hormonal contraceptive | ethinyl estradiol | ↓ ethinyl estradiol | An additional, non-hormonal method of contraception should be considered during the 5 days of PAXLOVID treatment and until one menstrual cycle after stopping PAXLOVID. |
Immunosuppressants | voclosporin | ↑ voclosporin | Co-administration contraindicated due to potential for acute and/or chronic nephrotoxicity [see Contraindications (4) ] . |
Immunosuppressants | calcineurin inhibitors: cyclosporine, tacrolimus | ↑ cyclosporine ↑ tacrolimus | Avoid concomitant use of calcineurin inhibitors with PAXLOVID when close monitoring of immunosuppressant concentrations is not feasible. If co-administered, dose adjustment of the immunosuppressant and close and regular monitoring for immunosuppressant concentrations and adverse reactions are recommended during and after treatment with PAXLOVID. Obtain expert consultation to appropriately manage the complexity of this co-administration [see Warnings and Precautions (5.1) ] . |
mTOR inhibitors: everolimus, sirolimus | ↑ everolimus ↑ sirolimus | Avoid concomitant use of everolimus and sirolimus and PAXLOVID. Refer to the individual immunosuppressant prescribing information and latest guidelines for further information. | |
Janus kinase (JAK) inhibitors | tofacitinib | ↑ tofacitinib | Dosage adjustment of tofacitinib is recommended. Refer to the tofacitinib prescribing information for more information. |
upadacitinib | ↑ upadacitinib | Dosing recommendations for co-administration of upadacitinib with PAXLOVID depends on the upadacitinib indication. Refer to the upadacitinib prescribing information for more information. | |
Long-acting beta-adrenoceptor agonist | salmeterol | ↑ salmeterol | Avoid concomitant use with PAXLOVID. The combination may result in increased risk of cardiovascular adverse events associated with salmeterol, including QT prolongation, palpitations, and sinus tachycardia. |
Microsomal triglyceride transfer protein (MTTP) inhibitor | lomitapide | ↑ lomitapide | Co-administration contraindicated due to potential for hepatotoxicity and gastrointestinal adverse reactions [see Contraindications (4) ] . |
Migraine medications | eletriptan | ↑ eletriptan | Co-administration of eletriptan within at least 72 hours of PAXLOVID is contraindicated due to potential for serious adverse reactions including cardiovascular and cerebrovascular events [see Contraindications (4) ] . |
ubrogepant | ↑ ubrogepant | Co-administration of ubrogepant with PAXLOVID is contraindicated due to potential for serious adverse reactions [see Contraindications (4) ] . | |
Migraine medications | rimegepant | ↑ rimegepant | Avoid concomitant use with PAXLOVID. |
Mineralocorticoid receptor antagonists | finerenone | ↑ finerenone | Co-administration contraindicated due to potential for serious adverse reactions including hyperkalemia, hypotension, and hyponatremia [see Contraindications (4) ] . |
Muscarinic receptor antagonists | darifenacin | ↑ darifenacin | The darifenacin daily-dose should not exceed 7.5 mg when co-administered with PAXLOVID. Refer to the darifenacin prescribing information for more information. |
Narcotic analgesics | fentanyl, hydrocodone, oxycodone, meperidine | ↑ fentanyl ↑ hydrocodone ↑ oxycodone ↑ meperidine | Careful monitoring of therapeutic and adverse effects (including potentially fatal respiratory depression) is recommended when fentanyl, hydrocodone, oxycodone, or meperidine is concomitantly administered with PAXLOVID. If concomitant use with PAXLOVID is necessary, consider a dosage reduction of the narcotic analgesic and monitor patients closely at frequent intervals. Refer to the individual product prescribing information for more information. |
methadone | ↓ methadone | Monitor methadone-maintained patients closely for evidence of withdrawal effects and adjust the methadone dose accordingly. | |
Neuropsychiatric agents | suvorexant | ↑ suvorexant | Avoid concomitant use of suvorexant with PAXLOVID. |
aripiprazole, brexpiprazole, cariprazine, iloperidone, lumateperone, pimavanserin | ↑ aripiprazole ↑ brexpiprazole ↑ cariprazine ↑ iloperidone ↑ lumateperone ↑ pimavanserin | Dosage adjustment of aripiprazole, brexpiprazole, cariprazine, iloperidone, lumateperone, and pimavanserin is recommended. Refer to the individual product prescribing information for more information. | |
Non-opioid analgesic (selective blocker of Na v 1.8 sodium channels) | suzetrigine | ↑ suzetrigine and active metabolite M6‑SUZ | Co-administration contraindicated due to potential for serious and/or life-threatening suzetrigine adverse reactions [see Contraindications (4) ] . |
Opioid antagonists | naloxegol | ↑ naloxegol | Co-administration contraindicated due to the potential for opioid withdrawal symptoms [see Contraindications (4) ] . |
Pulmonary hypertension agents (PDE5 inhibitors) | sildenafil (Revatio ® ) | ↑ sildenafil | Co-administration of sildenafil with PAXLOVID is contraindicated for use in pulmonary hypertension due to the potential for sildenafil associated adverse events, including visual abnormalities hypotension, prolonged erection, and syncope [see Contraindications (4) ] . |
Pulmonary hypertension agents (PDE5 inhibitors) | tadalafil (Adcirca ® ) | ↑ tadalafil | Avoid concomitant use of tadalafil with PAXLOVID for pulmonary hypertension. |
Pulmonary hypertension agents (sGC stimulators) | riociguat | ↑ riociguat | Dosage adjustment is recommended for riociguat when used for pulmonary hypertension. Refer to the riociguat prescribing information for more information. |
Erectile dysfunction agents (PDE5 inhibitors) | avanafil | ↑ avanafil | Do not use PAXLOVID with avanafil because a safe and effective avanafil dosage regimen has not been established. |
sildenafil, tadalafil, vardenafil | ↑ sildenafil ↑ tadalafil ↑ vardenafil | Dosage adjustment is recommended for use of sildenafil, tadalafil or vardenafil with PAXLOVID when used for erectile dysfunction. Refer to the individual product prescribing information for more information. | |
Sedative/hypnotics | triazolam, oral midazolam | ↑ triazolam ↑ midazolam | Co-administration contraindicated due to potential for extreme sedation and respiratory depression [see Contraindications (4) ] . |
Sedative/hypnotics | buspirone, clorazepate, diazepam, estazolam, flurazepam, zolpidem | ↑ sedative/hypnotic | A dose decrease may be needed for these drugs when co-administered with PAXLOVID and monitoring for adverse events. |
midazolam (administered parenterally) | ↑ midazolam | Co-administration of midazolam (parenteral) should be done in a setting which ensures close clinical monitoring and appropriate medical management in case of respiratory depression and/or prolonged sedation. Dosage reduction for midazolam should be considered, especially if more than a single dose of midazolam is administered. Refer to the midazolam prescribing information for further information. | |
Serotonin receptor 1A agonist/ serotonin receptor 2A antagonist | flibanserin | ↑ flibanserin | Co-administration contraindicated due to potential for hypotension, syncope, and CNS depression [see Contraindications (4) ] . |
Vasopressin receptor antagonists | tolvaptan | ↑ tolvaptan | Co-administration contraindicated due to potential for dehydration, hypovolemia and hyperkalemia [see Contraindications (4) ] . |
DESCRIPTION
PAXLOVID is nirmatrelvir tablets co-packaged with ritonavir tablets. Nirmatrelvir is a SARS-CoV-2 main protease (M pro ) inhibitor, and ritonavir is an HIV-1 protease inhibitor and CYP3A inhibitor.
Nirmatrelvir
The chemical name of active ingredient of nirmatrelvir is (1 R ,2 S ,5 S )- N -((1 S )-1-Cyano-2-((3 S )-2-oxopyrrolidin-3-yl)ethyl)-3-((2 S )-3,3-dimethyl-2-(2,2,2-trifluoroacetamido)butanoyl)-6,6-dimethyl-3-azabicyclo[3.1.0]hexane-2-carboxamide]. It has a molecular formula of C 23 H 32 F 3 N 5 O 4 and a molecular weight of 499.54. Nirmatrelvir has the following structural formula:

Nirmatrelvir is available as immediate-release, film-coated tablets. Each tablet contains 150 mg nirmatrelvir with the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, lactose monohydrate, microcrystalline cellulose, and sodium stearyl fumarate. The following are the ingredients in the film coating: hydroxy propyl methylcellulose, iron oxide red, polyethylene glycol, and titanium dioxide.
Ritonavir
Ritonavir is chemically designated as 10-Hydroxy-2-methyl-5-(1-methylethyl)-1- [2-(1 methylethyl)-4-thiazolyl]-3,6-dioxo-8,11-bis(phenylmethyl)-2,4,7,12- tetraazatridecan-13-oic acid, 5-thiazolylmethyl ester, [5S-(5R•,8R•,10R•,11R•)]. Its molecular formula is C 37 H 48 N 6 O 5 S 2 , and its molecular weight is 720.95. Ritonavir has the following structural formula:

Ritonavir is available as film-coated tablets. Each tablet contains 100 mg ritonavir with the following inactive ingredients: anhydrous dibasic calcium phosphate, colloidal silicon dioxide, copovidone, sodium stearyl fumarate, and sorbitan monolaurate. The film coating may include the following ingredients: colloidal anhydrous silica, colloidal silicon dioxide, hydroxypropyl cellulose, hypromellose, polyethylene glycol, polysorbate 80, talc, and titanium dioxide.
CLINICAL PHARMACOLOGY
Mechanism of Action
Nirmatrelvir is a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antiviral drug [see Microbiology (12.4) ].
Ritonavir is an HIV-1 protease inhibitor but is not active against SARS-CoV-2 M pro . Ritonavir inhibits the CYP3A-mediated metabolism of nirmatrelvir, resulting in increased plasma concentrations of nirmatrelvir.
Pharmacodynamics
Cardiac Electrophysiology
At 3 times the steady state peak plasma concentration (C max ) at the recommended dose, nirmatrelvir does not prolong the QTc interval to any clinically relevant extent.
Pharmacokinetics
The pharmacokinetics of nirmatrelvir/ritonavir were similar in healthy subjects and in subjects with mild-to-moderate COVID-19.
Nirmatrelvir AUC increased in a less than dose proportional manner over a single dose range from 250 mg to 750 mg (0.83 to 2.5 times the approved recommended dose) and multiple dose range from 75 mg to 500 mg (0.25 to 1.67 times the approved recommended dose), when administered in combination with 100 mg ritonavir. Nirmatrelvir steady state was achieved on Day 2 following administration of the approved recommended dosage and the mean accumulation ratio was approximately 2-fold.
The pharmacokinetic properties of nirmatrelvir/ritonavir are displayed in Table 3.
| Nirmatrelvir (When Given With Ritonavir) | Ritonavir | |
|---|---|---|
| Abbreviations: CL/F=apparent clearance; hr=hour; L/hr=liters per hour; T ½ =terminal elimination half-life; T max =the time to reach C max ; V z /F=apparent volume of distribution. | ||
Absorption | ||
T max (hr), median | 3.00 Represents data after a single dose of 300 mg nirmatrelvir (2 × 150 mg tablet formulation) administered together with 100 mg ritonavir tablet in healthy subjects. | 3.98 |
Food effect | Test/reference (fed/fasted) ratios of adjusted geometric means (90% CI) AUC inf and C max for nirmatrelvir were 119.67 (108.75, 131.68) and 161.01 (139.05, 186.44), respectively. Following a single oral dose of nirmatrelvir 300 mg boosted ritonavir 100 mg at -12 hours, 0 hours and 12 hours, administered under fed (high fat and high calorie meal) or fasted conditions. | |
Distribution | ||
% bound to human plasma proteins | 69% | 98–99% |
Blood-to-plasma ratio | 0.60 | 0.14 Red blood cell to plasma ratio. |
V z /F (L), mean | 104.7 300 mg nirmatrelvir (oral suspension formulation) co-administered with 100 mg ritonavir (tablet formulation) twice daily for 3 days. | 112.4 |
Elimination | ||
Major route of elimination | Renal elimination | Hepatic metabolism |
Half-life (T ½ ) (hr), mean | 6.05 | 6.15 |
Oral clearance (CL/F) (L/hr), mean | 8.99 | 13.92 |
Metabolism | ||
Metabolic pathways | Nirmatrelvir is a CYP3A substrate but when dosed with ritonavir, metabolic clearance is minimal. | Major CYP3A, Minor CYP2D6 |
Excretion | ||
% drug-related material in feces | 35.3% Determined by 19 F-NMR analysis following 300 mg nirmatrelvir oral suspension administered at 0 hr enhanced with 100 mg ritonavir at -12 hours, 0 hours, 12 hours, and 24 hours. | 86.4% Determined by 14 C analysis following 600 mg 14 C-ritonavir oral solution (6 times the approved ritonavir dose). |
% of dose excreted as total (unchanged drug) in feces | 27.5% | 33.8% |
% drug-related material in urine | 49.6% | 11.3% |
% of dose excreted as total (unchanged drug) in urine | 55.0% | 3.5% |
The predicted Day 5 nirmatrelvir exposure parameters in adult subjects with mild-to-moderate COVID-19 who were treated with PAXLOVID in EPIC-HR are presented in Table 4.
| Pharmacokinetic Parameter (units) Data presented as geometric mean (10 th and 90 th percentile). | Nirmatrelvir Based on 1,017 subjects with their post hoc PK parameters. |
|---|---|
| Abbreviations: C max =predicted maximal concentration; C min =predicted minimal concentration (C trough ). | |
C max (µg/mL) | 3.29 (1.93, 5.40) |
AUC tau (µg•hr/mL) AUC tau =predicted area under the plasma concentration-time profile from time 0 to 12 hours for twice-daily dosing. | 28.3 (12.5, 52.5) |
C min (µg/mL) | 1.40 (0.48, 3.45) |
Effect of Food
No clinically significant differences in the pharmacokinetics of nirmatrelvir were observed following administration of a high fat meal (800-1,000 calories; 50% fat) to healthy subjects.
Specific Populations
There were no clinically significant differences in the pharmacokinetics of nirmatrelvir based on age (18 to 86 years), sex, or race/ethnicity.
Pediatric Patients
The pharmacokinetics of nirmatrelvir/ritonavir in patients less than 18 years of age have not been established.
Patients with Renal Impairment
The pharmacokinetics of nirmatrelvir in subjects with renal impairment following administration of a single oral dose of nirmatrelvir 100 mg (0.33 times the approved recommended dose) co-administered with ritonavir 100 mg were determined. Compared to healthy controls with no renal impairment, the C max and AUC of nirmatrelvir in subjects with mild renal impairment was 30% and 24% higher, in subjects with moderate renal impairment was 38% and 87% higher, and in subjects with severe renal impairment was 48% and 204% higher, respectively.
The pharmacokinetics of nirmatrelvir in subjects with mild-to-moderate COVID-19 and severe renal impairment (eGFR<30 mL/min) either requiring intermittent hemodialysis (n=12) or not requiring hemodialysis (n=2) were evaluated after administration of 300 mg/100 mg nirmatrelvir/ritonavir once on Day 1 followed by 150 mg/100 mg nirmatrelvir/ritonavir once daily on Days 2-5 for a total of 5 doses.
The administration of 300 mg/100 mg nirmatrelvir/ritonavir once on Day 1 followed by 150 mg/100 mg nirmatrelvir/ritonavir once daily on Days 2-5 in subjects with severe renal impairment, either requiring intermittent hemodialysis or not requiring hemodialysis resulted in comparable exposures on Day 1 and at steady-state (AUC 0-24 and C max ) compared to those observed in subjects with normal renal function receiving 300 mg/100 mg nirmatrelvir/ritonavir twice daily for 5 days. During a 4-hour hemodialysis session, approximately 6.9% of nirmatrelvir dose was cleared through dialysis. Hemodialysis clearance was 1.83 L/h.
Patients with Hepatic Impairment
The pharmacokinetics of nirmatrelvir were similar in patients with moderate (Child-Pugh Class B) hepatic impairment compared to healthy subjects following administration of a single oral dose of nirmatrelvir 100 mg (0.33 times the approved recommended dose) co-administered with ritonavir 100 mg. The impact of severe hepatic impairment (Child-Pugh Class C) on the pharmacokinetics of nirmatrelvir or ritonavir has not been studied.
Clinical Drug Interaction Studies
Table 5 describes the effect of other drugs on the C max and AUC of nirmatrelvir.
| Co-administered Drug | Dose (Schedule) | N | Percent Ratio (in combination with co-administered drug/alone) of Nirmatrelvir Pharmacokinetic Parameters (90% CI); No Effect=100 | ||
|---|---|---|---|---|---|
| Co-administered Drug | Nirmatrelvir/ Ritonavir | C max | AUC For carbamazepine, AUC=AUC inf ; for itraconazole, AUC=AUC tau . | ||
| Abbreviations: AUC=area under the plasma concentration-time curve; AUC inf =area under the plasma concentration-time profile from time zero extrapolated to infinite time; AUC tau =area under the plasma concentration-time profile from time zero to time tau (τ), the dosing interval. CI=confidence interval; C max =observed maximum plasma concentrations. | |||||
Carbamazepine Carbamazepine titrated up to 300 mg twice daily on Day 8 through Day 15 (e.g., 100 mg twice daily on Day 1 through Day 3 and 200 mg twice daily on Day 4 through Day 7). | 300 mg twice daily (16 doses) | 300 mg/100 mg once daily (2 doses) | 10 | 56.82 (47.04, 68.62) | 44.50 (33.77, 58.65) |
Itraconazole | 200 mg once daily (8 doses) | 300 mg/100 mg twice daily (5 doses) | 11 | 118.57 (112.50, 124.97) | 138.82 (129.25, 149.11) |
Table 6 describes the effect of nirmatrelvir/ritonavir on the C max and AUC inf of other drugs.
| Co-administered Drug | Dose (Schedule) | N | Percent Ratio of Test/Reference of Geometric Means (90% CI); No Effect=100 | ||
|---|---|---|---|---|---|
| Co-administered Drug | Nirmatrelvir/ Ritonavir | C max | AUC inf | ||
| Abbreviations: AUC inf =area under the plasma concentration-time curve from time zero extrapolated to infinite time; CI=confidence interval; C max =observed maximum plasma concentrations; CYP3A4=cytochrome P450 3A4; OATP1B1=organic anion transporter polypeptide 1B1; P-gp=p-glycoprotein. | |||||
Midazolam For midazolam, Test=nirmatrelvir/ritonavir plus midazolam, Reference=Midazolam. Midazolam is an index substrate for CYP3A4. For dabigatran, Test=nirmatrelvir/ritonavir plus dabigatran, Reference=Dabigatran. Dabigatran is an index substrate for P-gp. For rosuvastatin, Test=nirmatrelvir/ritonavir plus rosuvastatin, Reference=Rosuvastatin. Rosuvastatin is an index substrate for OATP1B1. | 2 mg (1 dose) | 300 mg/100 mg twice daily (9 doses) | 10 | 368.33 (318.91, 425.41) | 1430.02 (1204.54, 1697.71) |
Dabigatran | 75 mg (1 dose) | 300 mg/100 mg twice daily (4 doses) | 24 | 233.06 (172.14, 315.54) | 194.47 (155.29, 243.55) |
Rosuvastatin | 10 mg (1 dose) | 300 mg/100 mg twice daily (3 doses) | 12 | 212.44 (174.31, 258.90) | 131.18 (115.89, 148.48) |
In Vitro Studies
Cytochrome P450 (CYP) Enzymes:
- Nirmatrelvir is a reversible and time-dependent inhibitor of CYP3A, but not an inhibitor CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. Nirmatrelvir is an inducer of CYP2B6, 2C8, 2C9, and 3A4, but there is minimal risk for pharmacokinetic interactions arising from induction of these CYP enzymes at the proposed therapeutic dose.
- Ritonavir is a substrate of CYP2D6 and CYP3A. Ritonavir is an inducer of CYP1A2, CYP2C9, CYP2C19, CYP2B6, and CYP3A.
Transporter Systems: Nirmatrelvir is an inhibitor of P-gp and OATP1B1. Nirmatrelvir is a substrate for P-gp, but not BCRP, MATE1, MATE2K, NTCP, OAT1, OAT2, OAT3, OCT1, OCT2, PEPT1, OATP1B1, OATP1B3, OATP2B1, or OATP4C1.
Microbiology
Mechanism of Action
Nirmatrelvir is a peptidomimetic inhibitor of the SARS-CoV-2 main protease (M pro ), also referred to as 3C-like protease (3CL pro ) or nonstructural protein 5 (nsp5) protease. Inhibition of SARS-CoV-2 M pro renders it incapable of processing the viral polyproteins pp1a and pp1ab, preventing viral replication. Nirmatrelvir inhibited the activity of recombinant SARS-CoV-2 M pro in a biochemical assay with a K i value of 3.1 nM and an IC 50 value of 19.2 nM. Nirmatrelvir was found to bind directly to the SARS-CoV-2 M pro active site by X-ray crystallography.
Antiviral Activity
Cell Culture Antiviral Activity
Nirmatrelvir exhibited antiviral activity against SARS-CoV-2 (USA-WA1/2020 isolate) infection of differentiated normal human bronchial epithelial (dNHBE) cells with EC 50 and EC 90 values of 62 nM (31 ng/mL) and 181 nM (90 ng/mL), respectively, after 3 days of drug exposure.
The antiviral activity of nirmatrelvir against the Omicron sub-variants BA.2, BA.2.12.1, BA.4, BA.4.6, BA.5, BF.7, BQ.1, BQ.1.11, XBB.1.5, EG.5, and JN.1 was assessed in Vero E6-TMPRSS2 cells in the presence of a P-gp inhibitor. Nirmatrelvir had a median EC 50 value of 88 nM (range: 39-146 nM) against the Omicron sub-variants, reflecting EC 50 value fold changes ≤1.8 relative to the USA-WA1/2020 isolate.
In addition, the antiviral activity of nirmatrelvir against the SARS-CoV-2 Alpha, Beta, Gamma, Delta, Lambda, Mu, and Omicron BA.1 variants was assessed in Vero E6 P-gp knockout cells. Nirmatrelvir had a median EC 50 value of 25 nM (range: 16-141 nM). The Beta variant was the least susceptible variant tested, with an EC 50 value fold change of 3.7 relative to USA-WA1/2020. The other variants had EC 50 value fold changes ≤1.1 relative to USA-WA1/2020.
Clinical Antiviral Activity
In clinical trial EPIC-HR, which enrolled subjects who were primarily infected with the SARS-CoV-2 Delta variant, PAXLOVID treatment was associated with a 0.83 log 10 copies/mL greater median decline in viral RNA shedding levels in nasopharyngeal samples through Day 5 (mITT1 analysis set, all treated subjects with onset of symptoms ≤5 days who at baseline did not receive nor were expected to receive COVID-19 therapeutic mAb treatment); similar results were observed in the mITT2 analysis set (all treated subjects with onset of symptoms ≤5 days). In the EPIC-SR trial, which included subjects who were infected with SARS-CoV-2 Delta (79%) or Omicron (19%) variants, PAXLOVID treatment was associated with a 1.05 log 10 copies/mL greater median decline in viral RNA shedding levels in nasopharyngeal samples through Day 5, with similar declines observed in subjects infected with Delta or Omicron variants. The degree of reduction in viral RNA levels relative to placebo following 5 days of PAXLOVID treatment was similar between unvaccinated high-risk subjects in EPIC-HR and vaccinated high-risk subjects in EPIC-SR.
Antiviral Resistance
In Cell Culture and Biochemical Assays
SARS-CoV-2 M pro residues potentially associated with nirmatrelvir resistance have been identified using a variety of methods, including SARS-CoV-2 resistance selection, testing of recombinant SARS-CoV-2 viruses with M pro substitutions, and biochemical assays with recombinant SARS-CoV-2 M pro containing amino acid substitutions. Table 7 indicates M pro substitutions and combinations of M pro substitutions that have been observed in SARS-CoV-2 under nirmatrelvir selective pressure in cell culture. Individual M pro substitutions are listed regardless of whether they occurred alone or in combination with other M pro substitutions. Note that the M pro S301P and T304I substitutions overlap the P6 and P3 positions of the nsp5/nsp6 cleavage site located at the C-terminus of M pro . Substitutions at other M pro cleavage sites have not been associated with nirmatrelvir resistance in cell culture. The clinical significance of these substitutions is unknown.
| Abbreviation: ND=no data. | |
Table 7: SARS-CoV-2 M pro Amino Acid Substitutions Selected by Nirmatrelvir in Cell Culture EC 50 value fold change ranges are shown in instances where multiple data points have been reported. | |
Single Substitutions (EC 50 value fold change in cell culture) | T21I (1.1-4.8), S46F (ND), L50F (1.2-4.2), P108S (ND), T135I (ND), F140L (4.1), S144A (2.2-5.3), C160F (2.1), E166A (3.3), E166V (25‑288), L167F (1.9-2.5), T169I (ND), H172Y (15), A173V (0.9-2.3), V186A (ND), R188G (ND), A191V (0.7-1.5), A193P (ND), P252L (5.9), S301P (ND), and T304I (1.4-5.5). |
≥2 Substitutions (EC 50 value fold change in cell culture) | T21I+S144A (9.4), T21I+E166V (83-250), T21I+A173V (3.1-8.9), T21I+T304I (3.0-7.9), L50F+E166V (34-175), L50F+T304I (5.9), T135I+T304I (3.8), F140L+A173V (10-17), H172Y+P252L (ND), A173V+T304I (5.8-20), T21I+L50F+A193P+S301P (29), T21I+S144A+T304I (11-28), T21I+C160F+A173V+V186A+T304I (28-29), T21I+A173V+T304I (15-16), and L50F+F140L+L167F+T304I (43-55). |
Table 8 indicates M pro substitutions and combinations of M pro substitutions that have been found to reduce nirmatrelvir activity ≥3-fold (based on IC 50 or K i values) in biochemical assays using recombinant SARS-CoV-2 M pro . Note that these M pro substitutions were laboratory engineered and most were not observed in PAXLOVID-treated subjects in clinical trials. In addition, according to public sequence databases, most of these substitutions have not been observed in clinical isolates or have been observed but with global cumulative frequencies ≤0.002%. Thus, the clinical relevance of these substitutions is unclear. The following M pro substitutions and combinations of M pro substitutions emerged in cell culture in the presence of nirmatrelvir but conferred <3-fold reduced nirmatrelvir activity in biochemical assays: T21I, S46F, L50F, P108S, T135I, C160F, T169I, V186A, A191V, A193P, P252L, S301P, T304I, T21I+T304I, and L50F+T304I.
Table 8: SARS-CoV-2 M pro Amino Acid Substitutions That Reduce Nirmatrelvir Activity ≥3-Fold in Biochemical Assays
Single Substitutions (IC 50 /K i value fold change in biochemical assay) | Y54A/C (3.0-25), F140A/L/S (1.2-230), G143S (3.6-148), S144A/F/G/M/W/Y (1.2-76), S144D/E/H/Q/T/V (81-480), S144K/L/P/R (1,165->5,319), H164N (1.9-6.7), M165D/F/G/T (5.7-51), M165H/K/P/R/W (>384), M165Y (3,838), E166A/G/K/L/Q (4.5-77), E166D/H/I/N/V/Y (143-708), E166R/V (>1,538-7,700), L167F (1.4-4.5), P168del (4.5-9.3), H172D/F/G/K/Q/Y (10-91), H172A/C/E/M/N/R/V/Y (114-858), H172I/L/S/T (1,172-6,740), A173S/V (4.1-52), R188G (38), Q189E/K (1.6-16), Q192A/C/D/E/F/G/H/I/K/L/P/R/S/T/V/W (5.0-61), Q192Y (>384), A260V (0.6-3.3), and V297A (3.0). |
≥2 Substitutions (IC 50 /K i value fold change in biochemical assay) | T21I+S144A (20), T21I+E166V (120-11,000), T21I+A173V (15), L50F+E166V (100-4,500), T135I+T304I (5.1), F140L+A173V (95), S144A+T304I (28), E166V+L232R (5,700), P168del+A173V (170-536), H172Y+P252L (180), A173V+T304I (28), T21I+S144A+T304I (51), T21I+A173V+T304I (55), L50F+E166A+L167F (52-180), T21I+L50F+A193P+S301P (7.3), L50F+F140L+L167F+T304I (190), and T21I+C160F+A173V+V186A+T304I (28). |
In Clinical Trials
Treatment-emergent substitutions were evaluated among subjects in clinical trials EPIC-HR/SR with sequence data available at both baseline and post-baseline visits (n=907 PAXLOVID-treated subjects, n=946 placebo-treated subjects). SARS-CoV-2 M pro amino acid changes were classified as PAXLOVID treatment-emergent substitutions if they occurred at the same amino acid position in 3 or more PAXLOVID-treated subjects and were ≥2.5-fold more common in PAXLOVID-treated subjects than placebo-treated subjects. The following PAXLOVID treatment-emergent M pro substitutions were observed: T98I/R/del(n=4), E166V (n=3), and W207L/R/del (n=4). In biochemical assays, the T98I and W207L/R substitutions did not affect nirmatrelvir activity (K i value fold changes were 0.3 and 0.7/0.3, respectively), whereas the E166V substitution (which occurs at a M pro -nirmatrelvir contact residue) reduced nirmatrelvir activity 187-7,700-fold. Within the M pro cleavage sites, the following PAXLOVID treatment-emergent substitutions were observed: A5328S/V(n=7) and S6799A/P/Y (n=4). These cleavage site substitutions were not associated with the co-occurrence of any specific M pro substitutions. In a cell culture replicon assay, the A5328S/V and S6799A substitutions did not affect nirmatrelvir activity (EC 50 value fold changes were 0.3/0.2 and 0.7, respectively).
None of the treatment-emergent substitutions listed above in M pro or M pro cleavage sites occurred in PAXLOVID-treated subjects who experienced hospitalization. Thus, the clinical significance of these substitutions is unknown.
Viral RNA Rebound and Treatment-Emergent Substitutions
EPIC-HR and EPIC-SR were not designed to evaluate COVID-19 rebound; exploratory analyses were conducted to assess the relationship between PAXLOVID use and rebound in viral RNA shedding levels.
Post-treatment increases in SARS-CoV-2 RNA shedding levels in nasopharyngeal samples were observed on Day 10 and/or Day 14 in a subset of PAXLOVID and placebo recipients in EPIC-HR and EPIC-SR, irrespective of COVID-19 symptoms. The frequency of detection of post-treatment viral RNA rebound varied according to analysis parameters, but was generally similar among PAXLOVID and placebo recipients. A similar or smaller percentage of placebo recipients compared to PAXLOVID recipients had nasopharyngeal viral RNA results < lower limit of quantitation (LLOQ) at all study timepoints in both the treatment and post-treatment periods.
In EPIC-HR, of 59 PAXLOVID-treated subjects identified with post-treatment viral RNA rebound and with available viral sequence data, treatment-emergent substitutions in M pro potentially reducing nirmatrelvir activity were detected in 2 (3%) subjects, including E166V in 1 subject and T304I in 1 subject. Both subjects had viral RNA shedding levels
Post-treatment viral RNA rebound was not associated with the primary clinical outcome of COVID-19 related hospitalization or death from any cause through Day 28 following the single 5-day course of PAXLOVID treatment. The clinical relevance of post-treatment increases in viral RNA following PAXLOVID or placebo treatment is unknown.
Cross-Resistance
Cross-resistance is not expected between nirmatrelvir and remdesivir or any other anti-SARS-CoV-2 agents with different mechanisms of action (i.e., agents that are not M pro inhibitors).
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Nirmatrelvir
Carcinogenicity studies have not been conducted with nirmatrelvir.
Nirmatrelvir was negative for mutagenic or clastogenic activity in a battery of in vitro and in vivo assays including the Ames bacterial reverse mutation assay using S. typhimurium and E. coli , the in vitro micronucleus assay using human lymphoblastoid TK6 cells, and the in vivo rat micronucleus assays.
In a fertility and early embryonic development study, nirmatrelvir was administered orally to male and female rats at doses of 60, 200, or 1,000 mg/kg/day once daily beginning 14 days prior to mating, throughout the mating phase, and continued through GD 6 for females and for a total of 32 doses for males. There were no effects on fertility, reproductive performance, or early embryonic development at doses up to 1,000 mg/kg/day, resulting in systemic exposure (AUC 24 ) approximately 5 times higher than exposure at the approved human dose of PAXLOVID.
Ritonavir
Carcinogenicity studies in mice and rats have been conducted on ritonavir. In male mice, at levels of 50, 100, or 200 mg/kg/day, there was a dose dependent increase in the incidence of both adenomas and combined adenomas and carcinomas in the liver. Based on AUC measurements, the exposure at the high dose was approximately 25 times higher than the exposure in humans at the approved human dose of PAXLOVID. No carcinogenic effects were observed in females at up to the highest dose tested, resulting in systemic exposure (AUC 24 ) approximately 25 times higher than the exposure in humans at the approved human dose of PAXLOVID. In rats dosed at levels of 7, 15, or 30 mg/kg/day, there were no carcinogenic effects. In this study, the exposure at the high dose was approximately 5 times higher than the exposure in humans at the approved human dose of PAXLOVID.
Ritonavir was found to be negative for mutagenic or clastogenic activity in a battery of in vitro and in vivo assays including the Ames bacterial reverse mutation assay using S. typhimurium and E. coli , the mouse lymphoma assay, the mouse micronucleus test and chromosomal aberration assays in human lymphocytes.
Ritonavir produced no effects on fertility in rats at drug exposures approximately 18 (male) and 27 (female) times higher than the exposure in humans at the approved human dose of PAXLOVID.
CLINICAL STUDIES
Efficacy in Subjects at High Risk of Progression to Severe COVID-19 (EPIC-HR)
EPIC-HR (NCT04960202) was a Phase 2/3, randomized, double-blind, placebo-controlled trial in non-hospitalized symptomatic adult subjects with a laboratory confirmed diagnosis of SARS-CoV-2 infection. Eligible subjects were 18 years of age and older with at least 1 of the following risk factors for progression to severe disease: diabetes, overweight (BMI >25), chronic lung disease (including asthma), chronic kidney disease, current smoker, immunosuppressive disease or immunosuppressive treatment, cardiovascular disease, hypertension, sickle cell disease, neurodevelopmental disorders, active cancer, medically-related technological dependence, or were 60 years of age and older regardless of comorbidities. Subjects with COVID-19 symptom onset of ≤5 days were included in the study. Subjects were randomized (1:1) to receive PAXLOVID (nirmatrelvir/ritonavir 300 mg/100 mg) or placebo orally every 12 hours for 5 days. The trial excluded individuals with a history of prior COVID-19 infection or vaccination and excluded individuals taking any medications with clinically significant drug interactions with PAXLOVID. The primary efficacy endpoint was the proportion of subjects with COVID-19 related hospitalization or death from any cause through Day 28. The analysis was conducted in the modified intent-to-treat (mITT) analysis set [all treated subjects with onset of symptoms ≤3 days who at baseline did not receive nor were expected to receive COVID-19 therapeutic monoclonal antibody (mAb) treatment], the mITT1 analysis set (all treated subjects with onset of symptoms ≤5 days who at baseline did not receive nor were expected to receive COVID-19 therapeutic mAb treatment), and the mITT2 analysis set (all treated subjects with onset of symptoms ≤5 days).
A total of 2,113 subjects were randomized to receive either PAXLOVID or placebo. At baseline, mean age was 45 years; 51% were male; 71% were White, 15% were Asian, 9% were American Indian or Alaska Native, 4% were Black or African American, and 1% was missing or unknown; 41% were Hispanic or Latino; 67% of subjects had onset of symptoms ≤3 days before initiation of study treatment; 49% of subjects were serological negative at baseline; the mean (SD) baseline viral RNA in nasopharyngeal samples was 4.71 log 10 copies/mL (2.89); 27% of subjects had a baseline viral RNA of ≥10^7 (log 10 copies/mL); 6% of subjects either received or were expected to receive COVID-19 therapeutic monoclonal antibody treatment at the time of randomization and were excluded from the mITT and mITT1 analyses.
The baseline demographic and disease characteristics were balanced between the PAXLOVID and placebo groups.
The proportions of subjects who discontinued treatment due to an adverse event were 2.0% in the PAXLOVID group and 4.2% in the placebo group.
Table 9 provides results of the primary endpoint in mITT1 analysis population. For the primary endpoint, the relative risk reduction in the mITT1 analysis population for PAXLOVID compared to placebo was 86% (95% CI: 72%, 93%).
| PAXLOVID (N=977) | Placebo (N=989) | |
|---|---|---|
| Abbreviations: CI=confidence interval; COVID-19=coronavirus disease 2019; mAb=monoclonal antibody; mITT1=modified intent-to-treat 1 (all treated subjects with onset of symptoms ≤5 days who at baseline did not receive nor were expected to receive COVID-19 therapeutic mAb treatment). The determination of primary efficacy was based on a planned interim analysis of 754 subjects in mITT population. The estimated risk reduction was -6.5% with a 95% CI of (-9.3%, -3.7%) and 2-sided p-value <0.0001. | ||
COVID-19 Related Hospitalization or Death from Any Cause Through Day 28 | ||
n (%) | 9 (0.9%) | 64 (6.5%) |
Reduction Relative to Placebo The estimated cumulative proportion of subjects hospitalized or death by Day 28 was calculated for each treatment group using the Kaplan-Meier method, where subjects without hospitalization and death status through Day 28 were censored at the time of study discontinuation. (95% CI), % | -5.6 (-7.3, -4.0) | |
COVID-19 Related Hospitalization Through Day 28, % | 9 (0.9%) | 63 (6.4%) |
All-cause Mortality Through Day 28 For the secondary endpoint of all-cause mortality through Week 24, there were 0 and 15 (1%) events in the PAXLOVID arm and placebo arm, respectively. , % | 0 | 12 (1.2%) |
Consistent results were observed in the mITT and mITT2 analysis populations.
Similar trends have been observed across subgroups of subjects (see Figure 1 ) .
Figure 1: Subgroup Analysis of Adults with COVID-19 Dosed within 5 Days of Symptom Onset with COVID-19 Related Hospitalization or Death from Any Cause Through Day 28: EPIC-HR
| Abbreviations: BMI=body mass index; COVID-19=coronavirus disease 2019; mAb=monoclonal antibody; mITT=modified intent-to-treat; SARS-CoV-2=severe acute respiratory syndrome coronavirus 2. N=number of subjects in the category of the analysis set. All categories are based on mITT1 population except for COVID-19 mAb treatment which is based on mITT2 population. Seropositivity was defined if results were positive in either Elecsys anti-SARS-CoV-2 S or Elecsys anti-SARS-CoV-2 (N) assay. The difference of the proportions in the 2 treatment groups and its 95% confidence interval based on normal approximation of the data are presented. |
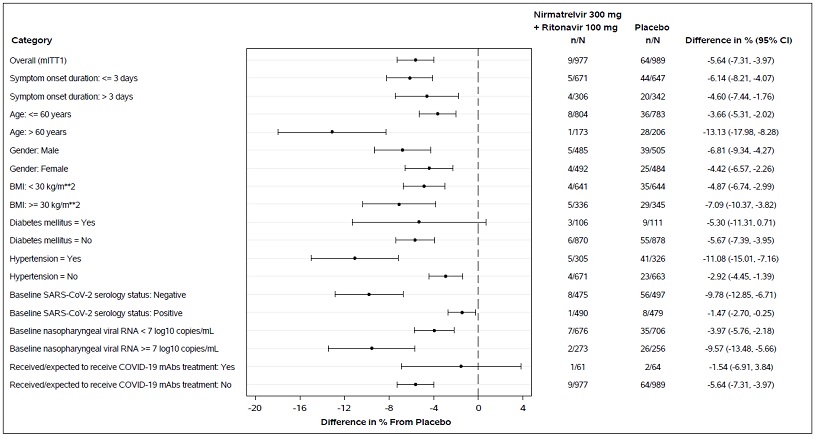 |
Among subjects who were SARS-CoV-2 seropositive at baseline, 1/490 (0.2%) PAXLOVID recipients versus 8/479 (1.7%) placebo recipients met the primary endpoint of COVID-19 related hospitalization or death from any cause through Day 28 [reduction relative to placebo -1.47% (-2.70%, -0.25%)].
Trial in Unvaccinated Subjects Without a Risk Factor for Progression to Severe COVID-19 or Subjects Fully Vaccinated Against COVID-19 With at Least One Factor for Progression to Severe COVID-19 (EPIC-SR)
PAXLOVID is not indicated for the treatment of COVID-19 in patients without a risk factor for progression to severe COVID-19.
EPIC-SR (NCT05011513) was a Phase 2/3, randomized, double-blind, placebo-controlled trial in non-hospitalized symptomatic adult subjects with a laboratory confirmed diagnosis of SARS-CoV-2 infection. Eligible subjects were 18 years of age or older with COVID-19 symptom onset of ≤5 days who were at standard risk for progression to severe disease. The trial included previously unvaccinated subjects with no risk factors for progression to severe disease or subjects fully vaccinated against COVID-19 (i.e., completed a primary vaccination series) with at least 1 of the risk factors for progression to severe disease as defined in EPIC-HR. Through the December 19, 2021, data cutoff, a total of 1,075 subjects were randomized (1:1) to receive PAXLOVID or placebo orally every 12 hours for 5 days; of these, 59% were fully vaccinated high-risk subjects.
The primary endpoint in this trial, the difference in time to sustained alleviation of all targeted COVID-19 signs and symptoms through Day 28 among PAXLOVID versus placebo recipients, was not met.
In an exploratory analysis of the subgroup of fully vaccinated subjects with at least 1 risk factor for progression to severe disease, a non-statistically significant numerical reduction relative to placebo for the secondary endpoint of COVID-19 related hospitalization or death from any cause through Day 28 was observed.
Post-Exposure Prophylaxis Trial
PAXLOVID is not indicated for the post-exposure prophylaxis of COVID-19.
In a double-blind, double-dummy, placebo-controlled trial, the efficacy of PAXLOVID when administered for 5 or 10 days as post-exposure prophylaxis of COVID-19 was evaluated. Eligible subjects were asymptomatic adults 18 years of age and older who were SARS-CoV-2 negative at baseline and who lived in the same household with symptomatic individuals with a recent diagnosis of SARS-CoV-2. A total of 2,736 subjects were randomized (1:1:1) to receive PAXLOVID orally every 12 hours for 5 days, PAXLOVID orally every 12 hours for 10 days, or placebo.
The primary endpoint for this trial was not met. The primary endpoint was the risk reduction between the 5-day and 10-day PAXLOVID regimens versus placebo in the proportion of subjects who developed RT-PCR or RAT-confirmed symptomatic SARS-CoV-2 infection through Day 14 who had a negative SARS-CoV-2 RT-PCR result at baseline. The proportion of subjects who had events through Day 14 was 2.6% for the 5-day PAXLOVID regimen, 2.4% for the 10-day PAXLOVID regimen, and 3.9% for placebo. There was not a statistically significant risk reduction versus placebo for either the 5-day or 10-day PAXLOVID regimen.
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
PAXLOVID is nirmatrelvir tablets co-packaged with ritonavir tablets. It is supplied in three different Dose Packs.
Nirmatrelvir tablets and ritonavir tablets are supplied in separate blister cavities within the same child-resistant blister card.
Dose Pack | Content | NDC | Description |
300 mg nirmatrelvir; 100 mg ritonavir | Each Carton Contains: 30 tablets divided in 10 blister cards | 0069-5045-30 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White to off-white, capsule-shaped, film-coated tablets debossed with "H" on one side and “R9” on the other side. |
Or | |||
0069-5321-30 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White film-coated ovaloid tablets debossed with "NK" on one side. | ||
Each Blister Card Contains: 2 nirmatrelvir tablets (150 mg each) and 1 ritonavir tablet (100 mg) | 0069-5045-06 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White to off-white, capsule-shaped, film-coated tablets debossed with "H" on one side and “R9” on the other side. | |
Or | |||
0069-5321-03 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White film-coated ovaloid tablets debossed with "NK" on one side. | ||
150 mg nirmatrelvir; 100 mg ritonavir | Each Carton Contains: 20 tablets divided in 10 blister cards | 0069-5317-20 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White film-coated ovaloid tablets debossed with “NK” on one side. |
Or | |||
0069-5434-20 | Nirmatrelvir tablets: Oval, pink immediate‑release, film‑coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White to off-white, capsule‑shaped, film‑coated tablets debossed with “H” on one side and “R9” on the other side. | ||
Each Blister Card Contains: 1 nirmatrelvir tablet (150 mg) and 1 ritonavir tablet (100 mg) | 0069-5317-02 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White film-coated ovaloid tablets debossed with “NK” on one side. | |
Or | |||
0069-5434-02 | Nirmatrelvir tablets: Oval, pink immediate‑release, film‑coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White to off-white, capsule‑shaped, film‑coated tablets debossed with “H” on one side and “R9” on the other side. | ||
300 mg nirmatrelvir; 100 mg ritonavir (Day 1) 150 mg nirmatrelvir; 100 mg ritonavir (Days 2-5) | Each Carton Contains: 11 tablets in 1 blister card | 0069-0521-11 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White film-coated ovaloid tablets debossed with “NK” on one side. |
Or | |||
0069-5450-11 | Nirmatrelvir tablets: Oval, pink immediate‑release, film‑coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White to off-white, capsule‑shaped, film‑coated tablets debossed with “H” on one side and “R9” on the other side. | ||
Each Blister Card Contains: 6 nirmatrelvir tablets (150 mg) and 5 ritonavir tablets (100 mg) | 0069-0521-11 | Nirmatrelvir tablets: Oval, pink immediate-release, film-coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White film-coated ovaloid tablets debossed with “NK” on one side. | |
Or | |||
0069-5450-11 | Nirmatrelvir tablets: Oval, pink immediate‑release, film‑coated tablets debossed with "PFE" on one side and "3CL" on the other side. Ritonavir tablets: White to off-white, capsule‑shaped, film‑coated tablets debossed with “H” on one side and “R9” on the other side. | ||
Storage and Handling
Store at USP controlled room temperature 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F).
Mechanism of Action
Nirmatrelvir is a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antiviral drug [see Microbiology (12.4) ].
Ritonavir is an HIV-1 protease inhibitor but is not active against SARS-CoV-2 M pro . Ritonavir inhibits the CYP3A-mediated metabolism of nirmatrelvir, resulting in increased plasma concentrations of nirmatrelvir.