Get your patient on Restasis Multidose - Cyclosporine emulsion (Cyclosporine)
Restasis Multidose - Cyclosporine emulsion prescribing information
1 INDICATIONS AND USAGE
RESTASIS MULTIDOSE ® ophthalmic emulsion is indicated to increase tear production in patients whose tear production is presumed to be suppressed due to ocular inflammation associated with keratoconjunctivitis sicca. Increased tear production was not seen in patients currently taking topical anti-inflammatory drugs or using punctal plugs.
2 DOSAGE AND ADMINISTRATION
Instill one drop of RESTASIS MULTIDOSE ophthalmic emulsion twice a day in each eye approximately 12 hours apart. RESTASIS MULTIDOSE can be used concomitantly with lubricant eye drops, allowing a 15-minute interval between products.
2.1 Preparation for First-Time Use
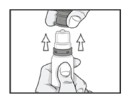
Step 1: Pull off the clear shipping cover by pulling straight up. Throw the shipping cover away. Do not use RESTASIS MULTIDOSE if shipping cover or pull tab are damaged or missing.

Step 2: Remove the pull tab on the olive green colored protective cap by pulling the end of the pull tab away from the bottle then winding it counterclockwise. Throw away the pull tab.

Step 3: Remove the olive green colored protective cap by pulling it straight up. Keep the colored protective cap.
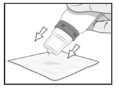
Step 4: Prime the bottle for first-time use by squeezing two drops onto a tissue. Do not let the bottle tip touch the tissue.
Step 5: The bottle is now ready for use. After use, recap the bottle with the olive green colored protective cap by pushing it straight down onto the bottle.

2.2 Preparation for Use
Step 6: Turn the bottle upside down a few times before giving your dose to make sure the medicine is mixed well.

Step 7: Instill one drop in the affected eye. Replace the olive green colored protective cap.
3 DOSAGE FORMS AND STRENGTHS
Ophthalmic emulsion containing cyclosporine 0.05% (0.5 mg/mL)
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary Clinical administration of cyclosporine ophthalmic emulsion 0.05% is not detected systemically following topical ocular administration [see Clinical Pharmacology (12.3) ] , and maternal use is not expected to result in fetal exposure to the drug. Oral administration of cyclosporine to pregnant rats or rabbits did not produce teratogenicity at clinically relevant doses [see Data] .
Data Animal Data At maternally toxic doses (30 mg/kg/day in rats and 100 mg/kg/day in rabbits), cyclosporine oral solution (USP) was teratogenic as indicated by increased pre- and postnatal mortality, reduced fetal weight and skeletal retardations. These doses (normalized to body surface area) are 5,000 and 32,000 times greater, respectively, than the daily recommended human dose of one drop (approximately 28 mcL) of cyclosporine ophthalmic emulsion 0.05% twice daily into each eye of a 60 kg person (0.001 mg/kg/day), assuming that the entire dose is absorbed. No evidence of embryofetal toxicity was observed in rats or rabbits receiving cyclosporine during organogenesis at oral doses up to 17 mg/kg/day or 30 mg/kg/day, respectively. These doses in rats and rabbits are approximately 3,000 and 10,000 times greater, respectively, than the daily recommended human dose.
An oral dose of 45 mg/kg/day cyclosporine administered to rats from Day 15 of pregnancy until Day 21 postpartum produced maternal toxicity and an increase in postnatal mortality in offspring. This dose is 7,000 times greater than the daily recommended human dose. No adverse effects in dams or offspring were observed at oral doses up to 15 mg/kg/day (2,000 times greater than the daily recommended human dose).
8.2 Lactation
Risk Summary Cyclosporine is known to appear in human milk following systemic administration, but its presence in human milk following topical treatment has not been investigated. Although blood concentrations are undetectable following topical administration of cyclosporine ophthalmic emulsion 0.05% [see Clinical Pharmacology (12.3) ] , caution should be exercised when RESTASIS MULTIDOSE is administered to a nursing woman. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for RESTASIS MULTIDOSE and any potential adverse effects on the breast-fed child from cyclosporine.
8.4 Pediatric Use
Safety and efficacy have not been established in pediatric patients below the age of 16.
8.5 Geriatric Use
No overall difference in safety or effectiveness has been observed between elderly and younger patients.
4 CONTRAINDICATIONS
RESTASIS MULTIDOSE is contraindicated in patients with known or suspected hypersensitivity to any of the ingredients in the formulation [ see Adverse Reactions (6.2) ] .
5 WARNINGS AND PRECAUTIONS
- To avoid the potential for eye injury and contamination, be careful not to touch the bottle tip to your eye or other surfaces. (5.1 )
5.000000000000000e+00 1 Potential for Eye Injury and Contamination
Be careful not to touch the bottle tip to your eye or other surfaces to avoid potential for eye injury and contamination.
5.2 Use with Contact Lenses
RESTASIS MULTIDOSE should not be administered while wearing contact lenses. Patients with decreased tear production typically should not wear contact lenses. If contact lenses are worn, they should be removed prior to the administration of the emulsion. Lenses may be reinserted 15 minutes following administration of RESTASIS MULTIDOSE ophthalmic emulsion.
6 ADVERSE REACTIONS
The following serious adverse reactions are described elsewhere in the labeling:
- Potential for Eye Injury and Contamination [ see Warnings and Precautions (5.1) ]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In clinical trials, the most common adverse reaction following the use of cyclosporine ophthalmic emulsion, 0.05% was ocular burning (17%).
Other reactions reported in 1% to 5% of patients included conjunctival hyperemia, discharge, epiphora, eye pain, foreign body sensation, pruritus, stinging, and visual disturbance (most often blurring).
6.2 Post-marketing Experience
The following adverse reactions have been identified during post approval use of cyclosporine ophthalmic emulsion, 0.05%. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Reported reactions have included: hypersensitivity (including eye swelling, urticaria, rare cases of severe angioedema, face swelling, tongue swelling, pharyngeal edema, and dyspnea); and superficial injury of the eye (from the bottle tip touching the eye during administration).
11 DESCRIPTION
RESTASIS MULTIDOSE (cyclosporine ophthalmic emulsion) 0.05% contains a calcineurin inhibitor immunosuppressant with anti-inflammatory effects. Cyclosporine’s chemical name is Cyclo[[( E )-(2 S ,3 R ,4 R )-3-hydroxy-4-methyl-2-(methylamino)-6-octenoyl]-L-2-aminobutyryl- N -methylglycyl- N -methyl-L-leucyl-L-valyl- N -methyl-L-leucyl-L-alanyl-D-alanyl- N -methyl-L-leucyl- N -methyl-L-leucyl- N -methyl-L-valyl] and it has the following structure:
Structural Formula
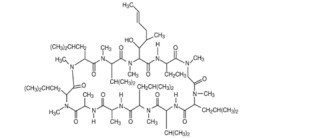
Formula: C 62 H 111 N 11 O 12 Mol. Wt.: 1202.6
Cyclosporine is a fine white powder. RESTASIS MULTIDOSE appears as a white opaque to slightly translucent homogeneous emulsion. It has an osmolality of 230 to 320 mOsmol/kg and a pH of 6.5-8.0. Each mL of RESTASIS MULTIDOSE ophthalmic emulsion contains: Active: cyclosporine 0.05%. Inactives: glycerin; castor oil; polysorbate 80; carbomer copolymer type A; purified water; and sodium hydroxide to adjust pH. RESTASIS MULTIDOSE contains no preservatives.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Cyclosporine is an immunosuppressive agent when administered systemically.
In patients whose tear production is presumed to be suppressed due to ocular inflammation associated with keratoconjunctivitis sicca, cyclosporine emulsion is thought to act as a partial immunomodulator. The exact mechanism of action is not known.
12.3 Pharmacokinetics
Blood cyclosporine A concentrations were measured using a specific high pressure liquid chromatography-mass spectrometry assay. Blood concentrations of cyclosporine, in all the samples collected, after topical administration of cyclosporine ophthalmic emulsion, 0.05%, twice daily, in humans for up to 12 months, were below the quantitation limit of 0.1 ng/mL. There was no detectable drug accumulation in blood during 12 months of treatment with cyclosporine ophthalmic emulsion, 0.05%.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis Systemic carcinogenicity studies were conducted in male and female mice and rats. In the 78-week oral (diet) mouse study, at doses of 1, 4, and 16 mg/kg/day, evidence of a statistically significant trend was found for lymphocytic lymphomas in females, and the incidence of hepatocellular carcinomas in mid-dose males significantly exceeded the control value.
In the 24-month oral (diet) rat study, conducted at 0.5, 2, and 8 mg/kg/day, pancreatic islet cell adenomas significantly exceeded the control rate in the low dose level. The hepatocellular carcinomas and pancreatic islet cell adenomas were not dose related. The low doses in mice and rats are approximately 80 times greater (normalized to body surface area) than the daily recommended human dose of one drop (approximately 28 mcL) of cyclosporine ophthalmic emulsion, 0.05% twice daily into each eye of a 60 kg person (0.001 mg/kg/day), assuming that the entire dose is absorbed.
Mutagenesis Cyclosporine has not been found to be mutagenic/genotoxic in the Ames Test, the V79-HGPRT Test, the micronucleus test in mice and Chinese hamsters, the chromosome-aberration tests in Chinese hamster bone-marrow, the mouse dominant lethal assay, and the DNA-repair test in sperm from treated mice. A study analyzing sister chromatid exchange (SCE) induction by cyclosporine using human lymphocytes in vitro gave indication of a positive effect (i.e., induction of SCE).
Impairment of Fertility No impairment in fertility was demonstrated in studies in male and female rats receiving oral doses of cyclosporine up to 15 mg/kg/day (approximately 2,000 times the human daily dose of 0.001 mg/kg/day normalized to body surface area) for 9 weeks (male) and 2 weeks (female) prior to mating.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In clinical trials, the most common adverse reaction following the use of cyclosporine ophthalmic emulsion, 0.05% was ocular burning (17%).
Other reactions reported in 1% to 5% of patients included conjunctival hyperemia, discharge, epiphora, eye pain, foreign body sensation, pruritus, stinging, and visual disturbance (most often blurring).
16 HOW SUPPLIED/STORAGE AND HANDLING
RESTASIS MULTIDOSE ophthalmic emulsion is packaged in a sterile, multi-dose bottle. Each bottle consists of a white opaque LDPE bottle, a white opaque polypropylene top with unidirectional valve and air filter, a protective olive green polypropylene cap, and a clear disposable shipping cover over the colored cap. RESTASIS MULTIDOSE contains no preservatives.
5.5 mL in 10-mL bottle - NDC 0023-5301-05
Storage: Store at 15°C to 25°C (59°F to 77°F). After opening, RESTASIS MULTIDOSE can be used until the expiration date on the bottle.
12.1 Mechanism of Action
Cyclosporine is an immunosuppressive agent when administered systemically.
In patients whose tear production is presumed to be suppressed due to ocular inflammation associated with keratoconjunctivitis sicca, cyclosporine emulsion is thought to act as a partial immunomodulator. The exact mechanism of action is not known.