Get your patient on Symdeko (Tezacaftor And Ivacaftor)
Dosage & administration

Symdeko prescribing information
INDICATIONS AND USAGE
SYMDEKO is indicated for the treatment of cystic fibrosis (CF) in patients aged 6 years and older who are homozygous for the F508del mutation or who have at least one mutation in the cystic fibrosis transmembrane conductance regulator ( CFTR ) gene that is responsive to tezacaftor/ivacaftor based on in vitro data and/or clinical evidence [see Clinical Pharmacology (12.1) and Clinical Studies (14) ] .
If the patient's genotype is unknown, an FDA-cleared CF mutation test should be used to detect the presence of a CFTR mutation followed by verification with bi-directional sequencing when recommended by the mutation test instructions for use.
DOSAGE AND ADMINISTRATION
- Pediatric patients aged 6 to less than 12 years weighing less than 30 kg: one tablet (containing tezacaftor 50 mg/ivacaftor 75 mg) in the morning and one tablet (containing ivacaftor 75 mg) in the evening, approximately 12 hours apart. SYMDEKO should be taken with fat-containing food. (2.1 , 2.2 , 12.3 )
- Adults and pediatric patients aged 12 years and older or pediatric patients aged 6 to less than 12 years weighing 30 kg or more: one tablet (containing tezacaftor 100 mg/ivacaftor 150 mg) in the morning and one tablet (containing ivacaftor 150 mg) in the evening, approximately 12 hours apart. SYMDEKO should be taken with fat-containing food. (2.1 , 2.2 , 12.3 )
- Reduce dosage in patients with moderate and severe hepatic impairment. (2.3 , 8.6 , 12.3 )
- See full prescribing information for dosage modifications due to drug interactions with SYMDEKO. (2.4 , 7.2 , 12.3 )
General Dosage Information
Swallow the tablets whole.
SYMDEKO should be taken with fat-containing food, such as food recommended in standard nutritional guidelines. Examples of meals or snacks that contain fat are those prepared with butter or oils or those containing eggs, cheeses, nuts, whole milk, or meats, etc. [see Clinical Pharmacology (12.3) ] .
Recommended Dosage in Adults, Adolescents, and Children Aged 6 Years and Older
Adults, adolescents, and children aged 6 years and older should be dosed according to Table 1. The morning and the evening doses should be taken approximately 12 hours apart.
| Age | Morning (one tablet) | Evening (one tablet) |
|---|---|---|
| 6 to <12 years weighing <30 kg | tezacaftor 50 mg/ivacaftor 75 mg | ivacaftor 75 mg |
| 6 to <12 years weighing ≥30 kg | tezacaftor 100 mg/ivacaftor 150 mg | ivacaftor 150 mg |
| ≥12 years | tezacaftor 100 mg/ivacaftor 150 mg | ivacaftor 150 mg |
Information for Missed Doses:
If 6 hours or less have passed since the missed morning or evening dose, the patient should take the missed dose as soon as possible and continue on the original schedule. If more than 6 hours have passed since the missed morning or evening dose, the patient should not take the missed dose. The next scheduled dose can be taken at the usual time. More than one dose should not be taken at the same time.
Recommended Dosage for Patients with Hepatic Impairment
For dosage adjustment for patients with hepatic impairment, refer to Table 2.
Studies have not been conducted in patients with severe hepatic impairment (Child-Pugh Class C), but exposure of tezacaftor and ivacaftor is expected to be higher than in patients with moderate hepatic impairment. Therefore, SYMDEKO should be used with caution at an adjusted dosage after weighing the risks and benefits of treatment in these patients [see Use in Specific Populations (8.6) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ].
| Hepatic Impairment | Morning | Evening | |
|---|---|---|---|
| Patients Aged 6 to <12 Years Weighing <30 kg | Patients Aged 6 to <12 Years Weighing ≥30 kg and Patients Age ≥12 Years | All Patients | |
| Mild (Child-Pugh Class A) | No dose adjustment | No dose adjustment | No dose adjustment |
| Moderate (Child-Pugh Class B) | One tablet of tezacaftor 50 mg/ivacaftor 75 mg once daily | One tablet of tezacaftor 100 mg/ivacaftor 150 mg once daily | No ivacaftor dose |
| Severe (Child-Pugh Class C) | One tablet of tezacaftor 50 mg/ivacaftor 75 mg once daily (or less frequently) | One tablet of tezacaftor 100 mg/ivacaftor 150 mg once daily (or less frequently) | |
Dosage Adjustment for Patients Taking Drugs that are CYP3A Inhibitors
The dosing regimen of SYMDEKO should be adjusted when co-administered with moderate and strong CYP3A inhibitors.
Moderate CYP3A inhibitors:
When co-administered with moderate CYP3A inhibitors (e.g., fluconazole, erythromycin), the dosing regimen should be adjusted as in Table 3 [see Drug Interactions (7.2) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
| Day 1 | Day 2 | Day 3 | Day 4 Continue dosing with tezacaftor/ivacaftor or ivacaftor tablets on alternate days. | |
|---|---|---|---|---|
| Patients Aged 6 to <12 Years Weighing <30 kg | ||||
| Morning | ||||
| Tezacaftor 50 mg/ivacaftor 75 mg tablet | ✓ | - | ✓ | - |
| Ivacaftor 75 mg tablet | - | ✓ | - | ✓ |
| Evening | ||||
| Ivacaftor 75 mg tablet | - | - | - | - |
| Patients Aged 6 to <12 Years Weighing ≥30 kg and Patients Age ≥12 Years | ||||
| Morning | ||||
| Tezacaftor 100 mg/ivacaftor 150 mg tablet | ✓ | - | ✓ | - |
| Ivacaftor 150 mg tablet | - | ✓ | - | ✓ |
| Evening | ||||
| Ivacaftor 150 mg tablet | - | - | - | - |
Strong CYP3A inhibitors:
When co-administered with strong CYP3A inhibitors (e.g., ketoconazole, itraconazole, posaconazole, voriconazole, telithromycin, and clarithromycin), the dosing regimen should be adjusted as in Table 4 [see Drug Interactions (7.2) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
| Day 1 | Day 2 and Day 3 | Day 4 Continue dosing with tezacaftor/ivacaftor tablets twice a week, taken approximately 3 to 4 days apart. | |
|---|---|---|---|
| Patients Aged 6 to <12 Years Weighing <30 kg | |||
| Morning | |||
| Tezacaftor 50 mg/ivacaftor 75 mg tablet | ✓ | - | ✓ |
| Evening The evening dose of ivacaftor should not be taken on any day. | |||
| Ivacaftor 75 mg tablet | - | - | - |
| Patients Aged 6 to <12 Years Weighing ≥30 kg and Patients Age ≥12 Years | |||
| Morning | |||
| Tezacaftor 100 mg/ivacaftor 150 mg tablet | ✓ | - | ✓ |
| Evening | |||
| Ivacaftor 150 mg tablet | - | - | - |
Food or drink containing grapefruit should be avoided during treatment with SYMDEKO [see Drug Interactions (7.2) and Patient Counseling Information (17) ] .
DOSAGE FORMS AND STRENGTHS
Tablets: Tezacaftor 50 mg/ivacaftor 75 mg fixed-dose combination tablets co-packaged with ivacaftor 75 mg tablets
- Tezacaftor 50 mg/ivacaftor 75 mg tablets are white, oblong-shaped, and debossed with "V50" on one side and plain on the other.
- Ivacaftor 75 mg tablets are light blue, oblong-shaped, and printed with "V 75" in black ink on one side and plain on the other.
Tablets: Tezacaftor 100 mg/ivacaftor 150 mg fixed-dose combination tablets co-packaged with ivacaftor 150 mg tablets
- Tezacaftor 100 mg/ivacaftor 150 mg tablets are yellow, oblong-shaped, and debossed with "V100" on one side and plain on the other.
- Ivacaftor 150 mg tablets are light blue, oblong-shaped, and printed with "V 150" in black ink on one side and plain on the other.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are limited and incomplete human data from clinical trials and postmarketing reports on the use of SYMDEKO or its individual components, tezacaftor and ivacaftor, in pregnant women to inform a drug-associated risk. Although there are no animal reproduction studies with the concomitant administration of tezacaftor and ivacaftor, separate reproductive and developmental studies were conducted with tezacaftor and ivacaftor in pregnant rats and rabbits. In animal reproduction studies, oral administration of tezacaftor to pregnant rats and rabbits during organogenesis demonstrated no teratogenicity or adverse developmental effects at doses that produced maternal exposures up to approximately 3 times the exposure at the maximum recommended human dose (MRHD) in rats and 0.2 times the MRHD in rabbits (based on summed AUCs for tezacaftor and M1 metabolite). Oral administration of ivacaftor to pregnant rats and rabbits during organogenesis demonstrated no teratogenicity or adverse developmental effects at doses that produced maternal exposures up to approximately 6 and 16 times the exposure at the MRHD, respectively. No adverse developmental effects were observed after oral administration of either tezacaftor or ivacaftor to pregnant rats from the period of organogenesis through lactation at doses that produced maternal exposures approximately 1 and 4 times the exposures at the MRHD, respectively ( see Data ).
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
Tezacaftor
In an embryo-fetal development study in pregnant rats dosed during the period of organogenesis from gestation Days 6-17, tezacaftor was not teratogenic and did not affect fetal development or survival at exposures up to 3 times the MRHD (based on summed AUCs for tezacaftor and M1 metabolite at maternal oral doses up to 100 mg/kg/day). In an embryo-fetal development study in pregnant rabbits dosed during the period of organogenesis from gestation Days 7-20, tezacaftor was not teratogenic and did not affect fetal development or survival at exposures up to 0.2 times the MRHD (based on summed AUCs for tezacaftor and M1 metabolite at maternal oral doses up to 25 mg/kg/day). Lower fetal body weights were observed in rabbits at a maternally toxic dose that produced exposures approximately 1 times the MRHD (at a maternal dose of 50 mg/kg/day). In a pre- and postnatal development (PPND) study in pregnant rats dosed from gestation Day 6 through lactation Day 18, tezacaftor had no adverse developmental effects on pups at an exposure of approximately 1 times the MRHD (based on summed AUCs for tezacaftor and M1 metabolite at a maternal dose of 25 mg/kg/day). Decreased fetal body weights and early developmental delays in pinna detachment, eye opening, and righting reflex occurred at a maternally toxic dose (based on maternal weight loss) that produced exposures approximately 2 times the exposure at the MRHD (based on summed AUCs for tezacaftor and M1 metabolite at a maternal oral dose of 50 mg/kg/day). Placental transfer of tezacaftor was observed in pregnant rats.
Ivacaftor
In an embryo-fetal development study in pregnant rats dosed during the period of organogenesis from gestation Days 7-17, ivacaftor was not teratogenic and did not affect fetal survival at exposures up to 6 times the MRHD (based on summed AUCs for ivacaftor and its metabolites at a maternal oral dose of 200 mg/kg/day). In an embryo-fetal development study in pregnant rabbits dosed during the period of organogenesis from gestation Days 7-19, ivacaftor was not teratogenic and did not affect fetal development or survival at exposures up to 16 times the MRHD (on an ivacaftor AUC basis at maternal oral doses up to 100 mg/kg/day). In a PPND study in pregnant rats dosed from gestation Day 7 through lactation Day 20, ivacaftor had no effects on delivery or growth and development of offspring at exposures up to 4 times the MRHD (based on summed AUCs for ivacaftor and its metabolites at maternal oral doses up to 100 mg/kg/day). Decreased fetal body weights were observed at a maternally toxic dose that produced exposures 6 times the MRHD. Placental transfer of ivacaftor was observed in pregnant rats and rabbits.
Lactation
Risk Summary
There is no information regarding the presence of tezacaftor or ivacaftor in human milk, the effects on the breastfed infant, or the effects on milk production. Both tezacaftor and ivacaftor are excreted into the milk of lactating rats ( see Data ). The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for SYMDEKO and any potential adverse effects on the breastfed child from SYMDEKO or from the underlying maternal condition.
Data
Tezacaftor
Lacteal excretion of tezacaftor in rats was demonstrated following a single oral dose (30 mg/kg) of 14 C-tezacaftor administered 6 to 10 days postpartum to lactating dams. Exposure of 14 C-tezacaftor in milk was approximately 3 times higher than in plasma (based on AUC 0-72h ).
Ivacaftor
Lacteal excretion of ivacaftor in rats was demonstrated following a single oral dose (100 mg/kg) of 14 C-ivacaftor administered 9 to 10 days postpartum to lactating dams. Exposure of 14 C-ivacaftor in milk was approximately 1.5 times higher than in plasma (based on AUC 0-24h ).
Pediatric Use
The safety and effectiveness of SYMDEKO for the treatment of CF have been established in pediatric patients aged 6 to less than 18 years who are homozygous for the F508del mutation or who have at least one mutation in the CFTR gene that is responsive to tezacaftor/ivacaftor based on in vitro data and/or clinical evidence [see Clinical Pharmacology (12.1) and Clinical Studies (14) ].
Clinical trials included the following patients with CF:
- 12 to less than 18 years of age who are homozygous for the F508del mutation [see Adverse Reactions (6) and Clinical Studies (14) ] .
- 12 to less than 18 years of age who are heterozygous for the F508del mutation and a second mutation predicted to be responsive to tezacaftor/ivacaftor [see Adverse Reactions (6) and Clinical Studies (14) ] .
- 6 to less than 12 years of age who are either homozygous for the F508del mutation or heterozygous for the F508del mutation and a second mutation predicted to be responsive to tezacaftor/ivacaftor [see Adverse Reactions (6) and Clinical Pharmacology (12) ].
The effectiveness of SYMDEKO in patients aged 6 to less than 12 years was extrapolated from patients aged 12 years and older with support from population pharmacokinetic analyses showing similar tezacaftor and ivacaftor exposure levels in patients aged 6 to less than 12 years and in patients aged 12 years and older [see Clinical Pharmacology (12.3) ] . Safety of SYMDEKO in this population was derived from a 24-week, open-label, clinical trial in 70 patients aged 6 to less than 12 years (mean age at screening 8.1 years) administered either tezacaftor 50 mg/ivacaftor 75 mg and ivacaftor 75 mg or tezacaftor 100 mg/ivacaftor 150 mg and ivacaftor 150 mg, 12 hours apart (Trial 4). The safety profile for patients in this trial was similar to that observed in Trials 1 and 3 [see Adverse Reactions (6.1) ].
The safety and effectiveness of SYMDEKO in patients with CF younger than 6 years of age have not been studied.
Juvenile Animal Toxicity Data
Findings of cataracts were observed in juvenile rats dosed from postnatal Day 7 through 35 with ivacaftor dose levels of 10 mg/kg/day and higher (0.25 times the MRHD based on systemic exposure of ivacaftor and its metabolites). This finding has not been observed in older animals.
Geriatric Use
Clinical trials of SYMDEKO did not include sufficient numbers of patients 65 years of age and over to determine whether they respond differently from younger patients.
Hepatic Impairment
No dosage adjustment is necessary for patients with mild hepatic impairment (Child-Pugh Class A). A reduced dosage of SYMDEKO is recommended in patients with moderate hepatic impairment (Child-Pugh Class B). There is no experience in patients with severe hepatic impairment (Child-Pugh Class C), but tezacaftor/ivacaftor exposure is expected to be higher than in patients with moderate hepatic impairment. Therefore, use with caution at a reduced dosage in patients with severe hepatic impairment after weighing the risks and benefits of treatment [see Dosage and Administration (2.3) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
Renal Impairment
SYMDEKO has not been studied in patients with moderate or severe renal impairment or in patients with end-stage renal disease. No dosage adjustment is recommended for mild and moderate renal impairment. Caution is recommended in patients with severe renal impairment or end-stage renal disease [Clinical Pharmacology (12.3)] .
Patients with Severe Lung Dysfunction
Trial 1 and Trial 2 included a total of 39 SYMDEKO-treated patients with ppFEV 1 <40 at baseline (range: 30-40); 23 patients in Trial 1 and 16 patients in Trial 2. There were 24 placebo-treated patients in Trial 1, and 15 placebo- and 13 ivacaftor-treated patients in Trial 2, with ppFEV 1 <40 at baseline. The safety and efficacy in this subgroup were comparable to the overall results observed in both Trials 1 and 2.
CONTRAINDICATIONS
None.
WARNINGS AND PRECAUTIONS
- Elevated transaminases (ALT or AST): Transaminases (ALT and AST) should be assessed prior to initiating SYMDEKO, every 3 months during the first year of treatment, and annually thereafter. In patients with a history of transaminase elevations, more frequent monitoring should be considered. Dosing should be interrupted in patients with significant elevations of transaminases, e.g., patients with ALT or AST >5 × upper limit of normal (ULN), or ALT or AST >3 × ULN with bilirubin >2 × ULN. Following resolution of transaminase elevations, consider the benefits and risks of resuming treatment. (5.1 , 6 )
- Hypersensitivity reactions: Anaphylaxis has been reported with SYMDEKO in the postmarketing setting. Initiate appropriate therapy in the event of a hypersensitivity reaction. (5.2 )
- Intracranial hypertension : Intracranial hypertension (IH) has been reported in the postmarketing setting with the use of drugs containing the same or similar active ingredients as SYMDEKO. If an unusual headache or visual disturbances occur during treatment, and IH is suspected, interrupt SYMDEKO and refer for prompt medical evaluation. (5.3 )
- Neuropsychiatric events, including suicidal thoughts and behaviors : Serious neuropsychiatric events, including symptoms of anxiety, depression, suicidal ideation and behavior, and sleep disturbances, have been reported in the postmarketing setting for SYMDEKO or drugs containing the same or similar active ingredients. Monitor patients closely for new or worsening symptoms. Consider the risks and benefits for the individual patient to determine if therapy with SYMDEKO should be interrupted at the occurrence of neuropsychiatric symptoms. (5.4 )
- Use with CYP3A inducers: Concomitant use with strong CYP3A inducers (e.g., rifampin, St. John's wort) substantially decrease exposure of ivacaftor and may decrease the exposure of tezacaftor, which may reduce therapeutic effectiveness. Therefore, co-administration is not recommended. (5.5 , 7.1 , 12.3 )
- Cataracts: Non-congenital lens opacities/cataracts have been reported in pediatric patients treated with SYMDEKO. Baseline and follow-up examinations are recommended in pediatric patients initiating SYMDEKO treatment. (5.6 , 8.4 )
Transaminase (AST/ALT) Elevations
Elevated transaminases have been observed in patients with CF treated with SYMDEKO, as well as with ivacaftor monotherapy. Assessments of transaminases (ALT and AST) are recommended for all patients prior to initiating SYMDEKO, every 3 months during the first year of treatment, and annually thereafter. For patients with a history of transaminase elevations more frequent monitoring should be considered. In the event of significant elevations of transaminases, e.g., patients with ALT or AST >5 × upper limit of normal (ULN), or ALT or AST >3 × ULN with bilirubin >2 × ULN, dosing should be interrupted and laboratory tests closely followed until the abnormalities resolve. Following the resolution of transaminase elevations consider the benefits and risks of resuming treatment [see Adverse Reactions (6) ] .
Hypersensitivity Reactions, Including Anaphylaxis
Hypersensitivity reactions, including cases of anaphylaxis, have been reported in the postmarketing setting [see Adverse Reactions (6.2) ] . If signs or symptoms of serious hypersensitivity reactions develop during treatment, discontinue SYMDEKO and institute appropriate therapy. Consider the benefits and risks for the individual patient to determine whether to resume treatment with SYMDEKO.
Intracranial Hypertension
Cases of intracranial hypertension (IH) have been reported in the postmarketing setting with the use of drugs containing the same or similar active ingredients as SYMDEKO [see Adverse Reactions (6.2) ] . Clinical manifestations of IH include headache, blurred vision, diplopia, and potential vision loss; papilledema can be found on fundoscopy. If an unusual headache or visual disturbances occur during treatment, and IH is suspected, interrupt SYMDEKO and refer for prompt medical evaluation. Consider the benefits and risks for the individual patient to determine whether to resume treatment with SYMDEKO. Patients should be monitored until IH resolution and for recurrence. Patients with elevated vitamin A levels may be at increased risk.
Neuropsychiatric Events, Including Suicidal Thoughts and Behaviors
Serious neuropsychiatric events, including symptoms of anxiety, depression, suicidal ideation and behavior, and sleep disturbances, have been reported in the postmarketing setting in patients taking SYMDEKO or drugs containing the same or similar active ingredients [see Adverse Reactions (6.2) ] . The events were reported in adult and pediatric patients with and without a previous history of neuropsychiatric symptoms. Symptoms may occur within the first three months of treatment initiation.
Assess patients for baseline neuropsychiatric symptoms and monitor for new or worsening symptoms of anxiety, depression, suicidal ideation or behavior, or sleep disturbances. Consider the benefits and risks for the individual patient to determine if therapy with SYMDEKO should be interrupted at the occurrence of neuropsychiatric symptoms and whether to resume therapy with symptom improvement.
Concomitant Use with CYP3A Inducers
Exposure to ivacaftor is significantly decreased and exposure to tezacaftor may be reduced by the concomitant use of CYP3A inducers, which may reduce the therapeutic effectiveness of SYMDEKO. Therefore, co-administration with strong CYP3A inducers is not recommended [see Drug Interactions (7.1) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
Cataracts
Cases of non-congenital lens opacities have been reported in pediatric patients treated with SYMDEKO, as well as with ivacaftor monotherapy. Although other risk factors were present in some cases (such as corticosteroid use, exposure to radiation), a possible risk attributable to treatment with SYMDEKO cannot be excluded. Baseline and follow-up ophthalmological examinations are recommended in pediatric patients initiating treatment with SYMDEKO [see Use in Specific Populations (8.4) and Patient Counseling Information (17) ] .
ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the label:
- Transaminase Elevations [see Warnings and Precautions (5.1) ]
- Hypersensitivity Reactions, Including Anaphylaxis [see Warnings and Precautions (5.2) ]
- Intracranial Hypertension [see Warnings and Precautions (5.3) ]
- Neuropsychiatric Events, Including Suicidal Thoughts and Behaviors [see Warnings and Precautions (5.4) ]
- Cataracts [see Warnings and Precautions (5.6) ]
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The overall safety profile of SYMDEKO is based on data from 1001 patients in three double-blind, placebo-controlled, clinical trials: two parallel-group trials of 12 and 24-week duration and one cross-over design trial of 8 weeks duration. Eligible patients were also able to participate in an open-label extension safety study (up to 96 weeks of SYMDEKO). In the three placebo-controlled trials (Trials 1, 2, and 3), a total of 496 patients with CF aged 12 years and older received at least one dose of SYMDEKO. The proportion of patients who discontinued study drug prematurely due to adverse reactions was 1.6% for SYMDEKO-treated patients and 2.0% for placebo-treated patients. Serious adverse reactions, whether considered drug-related or not by the investigators, that occurred more frequently in SYMDEKO-treated patients compared to placebo included distal intestinal obstruction syndrome, 3 (0.6%) SYMDEKO-treated patients vs. 0 placebo. There were no deaths in the placebo-controlled trials, and one death in the open-label extension study due to respiratory failure and influenza infection in a patient who had discontinued SYMDEKO seven weeks prior.
The safety profile of SYMDEKO was generally similar across all subgroups of patients, including analysis by age, sex, baseline percent predicted FEV 1 (ppFEV 1 ), and geographic regions.
Table 5 shows adverse reactions occurring in ≥3% of SYMDEKO-treated patients that also occurred at a higher rate than in the placebo-treated patients in the 12- and 24-week placebo-controlled, parallel-group trials (Trials 1 and 3).
| Adverse Reactions (Preferred Term) | SYMDEKO N=334 n (%) | Placebo N=343 n (%) |
|---|---|---|
| Headache | 49 (15) | 44 (13) |
| Nausea | 29 (9) | 24 (7) |
| Sinus congestion | 13 (4) | 6 (2) |
| Dizziness | 12 (4) | 8 (2) |
The safety data from the following trials are similar to that observed in Trials 1 and 3:
- an 8-week randomized, double-blind, placebo-controlled crossover study in 244 patients with CF aged 12 years and older who were heterozygous for the F508del mutation and a second mutation predicted to be responsive to tezacaftor/ivacaftor (Trial 2).
- a 24-week open-label study in 70 patients with CF aged 6 to less than 12 years who were either homozygous for the F508del mutation or heterozygous for the F508del mutation and a second mutation predicted to be responsive to tezacaftor/ivacaftor (Trial 4).
Laboratory Abnormalities
Transaminase elevations
During the placebo-controlled trials in patients aged 12 years and older, the incidence of maximum transaminase (ALT or AST) >8, >5, and >3 × the upper limit of normal (ULN) was similar between SYMDEKO-treated patients and placebo-treated patients; 0.2%, 1.0%, and 3.4% in SYMDEKO-treated patients, and 0.4%, 1.0%, and 3.4% in placebo-treated patients. One patient (0.2%) on SYMDEKO and 2 patients (0.4%) on placebo permanently discontinued treatment for elevated transaminases. No SYMDEKO-treated patients experienced a transaminase elevation >3 × ULN associated with elevated total bilirubin >2 × ULN.
During the 24-week, open-label study in patients aged 6 to less than 12 years (Trial 4), the incidence of maximum transaminase (ALT or AST) >8, >5, and >3 × ULN were 1.4%, 4.3%, and 10.0%, respectively. No SYMDEKO-treated patients experienced a transaminase elevation >3 × ULN associated with elevated total bilirubin >2 × ULN or discontinued SYMDEKO treatment due to transaminase elevations.
Postmarketing Experience
The following adverse reactions have been identified during postapproval use of SYMDEKO or drugs containing the same or similar active ingredients as SYMDEKO. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune System Disorders : anaphylaxis
Skin : rash
Nervous System Disorders : intracranial hypertension
Psychiatric Disorders : anxiety, depression, suicidal ideation and behavior, insomnia
DRUG INTERACTIONS
Potential for other drugs to affect tezacaftor/ivacaftor
Inducers of CYP3A
Tezacaftor and ivacaftor are substrates of CYP3A (ivacaftor is a sensitive substrate of CYP3A). Concomitant use of CYP3A inducers may result in reduced exposures and thus reduced SYMDEKO efficacy. Co-administration of ivacaftor with rifampin, a strong CYP3A inducer, significantly decreased ivacaftor exposure (area under the curve [AUC]) by 89%. Tezacaftor exposures can also be expected to decrease significantly during co-administration with strong CYP3A inducers. Therefore, co-administration of SYMDEKO with strong CYP3A inducers is not recommended [see Warnings and Precautions (5.5) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
Examples of strong CYP3A inducers include:
- rifampin, rifabutin, phenobarbital, carbamazepine, phenytoin, and St. John's wort (Hypericum perforatum)
Inhibitors of CYP3A
Co-administration with itraconazole, a strong CYP3A inhibitor, increased tezacaftor exposure (AUC) by 4.0-fold and ivacaftor by 15.6-fold. When co-administered with strong CYP3A inhibitors, the dosing regimen of SYMDEKO should be adjusted [see Dosage and Administration (2.4) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
Examples of strong CYP3A inhibitors include:
- ketoconazole, itraconazole, posaconazole, and voriconazole
- telithromycin and clarithromycin
Co-administration of fluconazole increased ivacaftor exposure (AUC) by 3.0-fold. Simulation suggested co-administration with fluconazole, a moderate CYP3A inhibitor, may increase tezacaftor exposure (AUC) by approximately 2.0-fold. When co-administered with moderate CYP3A inhibitors, the dosing regimen of SYMDEKO should be adjusted [see Dosage and Administration (2.4) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
Examples of moderate CYP3A inhibitors include:
- fluconazole
- erythromycin
Co-administration of SYMDEKO with grapefruit juice, which contains one or more components that moderately inhibit CYP3A, may increase exposure of tezacaftor and ivacaftor; therefore, food or drink containing grapefruit should be avoided during treatment with SYMDEKO [see Dosage and Administration (2.4) , Clinical Pharmacology (12.3) , and Patient Counseling Information (17) ] .
Ciprofloxacin
Co-administration of SYMDEKO with ciprofloxacin had no significant effect on the exposure of tezacaftor or ivacaftor. Therefore, no dosage adjustment is necessary during concomitant administration of SYMDEKO with ciprofloxacin [see Clinical Pharmacology (12.3) ] .
Potential for tezacaftor/ivacaftor to affect other drugs
CYP3A Substrates
Co-administration of SYMDEKO with midazolam (oral), a sensitive CYP3A substrate, did not affect midazolam exposure. No dosage adjustment of CYP3A substrates is required when co-administered with SYMDEKO [see Clinical Pharmacology (12.3) ] .
CYP2C9 Substrates
Ivacaftor may inhibit CYP2C9; therefore, monitoring of the international normalized ratio (INR) during co-administration of SYMDEKO with warfarin is recommended. Other medicinal products for which exposure may be increased by SYMDEKO include glimepiride and glipizide; these medicinal products should be used with caution [see Clinical Pharmacology (12.3) ] .
Digoxin and Other P-gp Substrates
Co-administration of SYMDEKO with digoxin, a sensitive P-gp substrate, increased digoxin exposure by 1.3-fold consistent with weak inhibition of P-gp by ivacaftor. Administration of SYMDEKO may increase systemic exposure of medicinal products that are sensitive substrates of P-gp, which may increase or prolong their therapeutic effect and adverse reactions. When used concomitantly with digoxin or other substrates of P-gp with a narrow therapeutic index such as cyclosporine, everolimus, sirolimus, and tacrolimus, caution and appropriate monitoring should be used [see Clinical Pharmacology (12.3) ] .
Hormonal Contraceptives
SYMDEKO has been studied with an ethinyl estradiol/norethindrone oral contraceptive and was found to have no significant effect on the exposures of the hormonal contraceptive. SYMDEKO is not expected to modify the efficacy of hormonal contraceptives [see Clinical Pharmacology (12.3) ] .
DESCRIPTION
SYMDEKO is co-packaged as a tezacaftor/ivacaftor fixed-dose combination tablet and an ivacaftor tablet. Both tablets are for oral administration.
Tezacaftor 50 mg/ivacaftor 75 mg fixed-dose combination tablets and ivacaftor 75 mg tablets :
The tezacaftor/ivacaftor fixed-dose combination tablet is available as a white, oblong-shaped, film-coated tablet containing 50 mg of tezacaftor, 75 mg of ivacaftor, and the following inactive ingredients: croscarmellose sodium, hypromellose, hypromellose acetate succinate, magnesium stearate, microcrystalline cellulose and sodium lauryl sulfate. The tablet film coat contains HPMC/hypromellose 2910, hydroxypropyl cellulose, talc and titanium dioxide.
The ivacaftor tablet is available as a light blue, oblong-shaped, film-coated tablet containing 75 mg of ivacaftor and the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose acetate succinate, lactose monohydrate, magnesium stearate, microcrystalline cellulose, and sodium lauryl sulfate. The tablet film coat contains carnauba wax, FD&C Blue #2, PEG 3350, polyvinyl alcohol, talc, and titanium dioxide. The printing ink contains ammonium hydroxide, iron oxide black, propylene glycol, and shellac.
Tezacaftor 100 mg/ivacaftor 150 mg fixed-dose combination tablets and ivacaftor 150 mg tablets :
The tezacaftor/ivacaftor fixed-dose combination tablet is available as a yellow, oblong-shaped, film-coated tablet containing 100 mg of tezacaftor, 150 mg of ivacaftor, and the following inactive ingredients: croscarmellose sodium, hypromellose, hypromellose acetate succinate, magnesium stearate, microcrystalline cellulose and sodium lauryl sulfate. The tablet film coat contains HPMC/hypromellose 2910, hydroxypropyl cellulose, iron oxide yellow, talc and titanium dioxide.
The ivacaftor tablet is available as a light blue, oblong-shaped, film-coated tablet containing 150 mg of ivacaftor and the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, hypromellose acetate succinate, lactose monohydrate, magnesium stearate, microcrystalline cellulose, and sodium lauryl sulfate. The tablet film coat contains carnauba wax, FD&C Blue #2, PEG 3350, polyvinyl alcohol, talc, and titanium dioxide. The printing ink contains ammonium hydroxide, iron oxide black, propylene glycol, and shellac.
The active ingredients of SYMDEKO are described below.
Tezacaftor
Tezacaftor is a white to off-white powder that is practically insoluble in water (<5 microgram/mL). Its chemical name of tezacaftor is 1-(2,2-difluoro-2H-1,3-benzodioxol-5-yl)-N-{1-[(2R)-2,3-dihydroxypropyl]-6-fluoro-2-(1-hydroxy-2-methylpropan-2-yl)-1Hindol-5-yl}cyclopropane-1-carboxamide. Its molecular formula is C 26 H 27 N 2 F 3 O 6 and its molecular weight is 520.50. Tezacaftor has the following structural formula:
Ivacaftor
Ivacaftor is a white to off-white powder that is practically insoluble in water (<0.05 microgram/mL). Pharmacologically it is a CFTR potentiator. Its chemical name is N -(2,4-di-tert-butyl-5-hydroxyphenyl)-1,4-dihydro-4-oxoquinoline-3-carboxamide. Its molecular formula is C 24 H 28 N 2 O 3 and its molecular weight is 392.49. Ivacaftor has the following structural formula:
CLINICAL PHARMACOLOGY
Mechanism of Action
Tezacaftor facilitates the cellular processing and trafficking of select mutant forms of CFTR (including F508del-CFTR) to increase the amount of mature CFTR protein delivered to the cell surface. Ivacaftor is a CFTR potentiator that facilitates increased chloride transport by potentiating the channel-open probability (or gating) of the CFTR protein at the cell surface. For ivacaftor to function CFTR protein must be present at the cell surface. Ivacaftor can potentiate the CFTR protein delivered to the cell surface by tezacaftor, leading to a further enhancement of chloride transport than either agent alone. The combined effect of tezacaftor and ivacaftor is increased quantity and function of CFTR at the cell surface, resulting in increases in chloride transport.
CFTR Chloride Transport Assay in Fischer Rat Thyroid (FRT) cells expressing mutant CFTR
The chloride transport response of mutant CFTR protein to tezacaftor/ivacaftor was determined in Ussing chamber electrophysiology studies using a panel of FRT cell lines transfected with individual CFTR mutations. Tezacaftor/ivacaftor increased chloride transport in FRT cells expressing CFTR mutations that result in CFTR protein being delivered to the cell surface.
The in vitro chloride transport response threshold was designated as a net increase of at least 10% of normal over baseline because it is predictive or reasonably expected to predict clinical benefit. For individual mutations, the magnitude of the net change over baseline in CFTR-mediated chloride transport in vitro is not correlated with the magnitude of clinical response.
Note that splice site mutations cannot be studied in the FRT assay.
Table 6 lists responsive CFTR mutations based on (1) a clinical FEV 1 response and/or (2) in vitro data in FRT cells, indicating that tezacaftor/ivacaftor increases chloride transport to at least 10% of normal over baseline. CFTR gene mutations that are not responsive to ivacaftor alone are not expected to respond to SYMDEKO except for F508del homozygotes.
| 546insCTA | E92K | G576A | L346P | R117G | S589N |
| 711+3A→G Clinical data for these mutations in Clinical Studies [see Clinical Studies (14.1 and 14.2) ] . | E116K | G576A;R668C Complex/compound mutations where a single allele of the CFTR gene has multiple mutations; these exist independent of the presence of mutations on the other allele. | L967S | R117H | S737F |
| 2789+5G→A | E193K | G622D | L997F | R117L | S912L |
| 3272-26A→G | E403D | G970D | L1324P | R117P | S945L |
| 3849+10kbC→T | E588V | G1069R | L1335P | R170H | S977F |
| A120T | E822K | G1244E | L1480P | R258G | S1159F |
| A234D | E831X | G1249R | M152V | R334L | S1159P |
| A349V | F191V | G1349D | M265R | R334Q | S1251N |
| A455E | F311del | H939R | M952I | R347H | S1255P |
| A554E | F311L | H1054D | M952T | R347L | T338I |
| A1006E | F508C | H1375P | P5L | R347P | T1036N |
| A1067T | F508C;S1251N | I148T | P67L | R352Q | T1053I |
| D110E | F508del A patient must have two copies of the F508del mutation or at least one copy of a responsive mutation presented in Table 6 to be indicated. | I175V | P205S | R352W | V201M |
| D110H | F575Y | I336K | Q98R | R553Q | V232D |
| D192G | F1016S | I601F | Q237E | R668C | V562I |
| D443Y | F1052V | I618T | Q237H | R751L | V754M |
| D443Y;G576A;R668C | F1074L | I807M | Q359R | R792G | V1153E |
| D579G | F1099L | I980K | Q1291R | R933G | V1240G |
| D614G | G126D | I1027T | R31L | R1066H | V1293G |
| D836Y | G178E | I1139V | R74Q | R1070Q | W1282R |
| D924N | G178R | I1269N | R74W | R1070W | Y109N |
| D979V | G194R | I1366N | R74W;D1270N | R1162L | Y161S |
| D1152H | G194V | K1060T | R74W;V201M | R1283M | Y1014C |
| D1270N | G314E | L15P | R74W;V201M;D1270N | R1283S | Y1032C |
| E56K | G551D | L206W | R75Q | S549N | |
| E60K | G551S | L320V | R117C | S549R |
Pharmacodynamics
Effects on Sweat Chloride
In Trial 1 (patients aged 12 years and older who were homozygous for the F508del mutation), the treatment difference between SYMDEKO and placebo in mean absolute change from baseline in sweat chloride through Week 24 was -10.1 mmol/L (95% CI: -11.4, -8.8).
In Trial 2 (patients aged 12 years and older who were heterozygous for the F508del mutation and a second mutation predicted to be responsive to tezacaftor/ivacaftor), the treatment difference in mean absolute change from baseline in sweat chloride through Week 8 was -9.5 mmol/L (95% CI: -11.7, -7.3) between SYMDEKO and placebo, and -4.5 mmol/L (95% CI: -6.7, -2.3) between ivacaftor and placebo.
In Trial 4 (patients aged 6 to less than 12 years) a reduction in sweat chloride was observed from baseline through Week 4 and sustained throughout the 24-week treatment period. Mean absolute change in sweat chloride from baseline through Week 24 was -14.5 mmol/L (95% CI: -17.4, -11.6).
Cardiac Electrophysiology
At a dose 3 times the maximum approved recommended dose, tezacaftor does not prolong the QT interval to any clinically relevant extent.
In a separate study of ivacaftor evaluating doses up to 3 times the maximum approved recommended dose, ivacaftor does not prolong the QT interval to any clinically relevant extent.
Pharmacokinetics
The pharmacokinetics of tezacaftor and ivacaftor are similar between healthy adult volunteers and patients with CF. Following once-daily dosing of tezacaftor and twice-daily dosing of ivacaftor in patients with CF, plasma concentrations of tezacaftor and ivacaftor reach steady-state within 8 days and within 3 to 5 days, respectively, after starting treatment. At steady-state, the accumulation ratio is approximately 1.5 for tezacaftor and 2.2 for ivacaftor. Exposures of tezacaftor (administered alone or in combination with ivacaftor) increase in an approximately dose-proportional manner with increasing doses from 10 mg to 300 mg once daily.
Key pharmacokinetic parameters for tezacaftor and ivacaftor at steady state are shown in Table 7.
| Drug | C max (mcg/mL) | Effective t ½ (h) | AUC 0-24h or AUC 0-12h (mcg∙h/mL) AUC 0-24h for tezacaftor and AUC 0-12h for ivacaftor | |
|---|---|---|---|---|
| Tezacaftor 100 mg once daily/ivacaftor 150 mg every 12 hours | Tezacaftor | 5.95 (1.50) | 15.0 (3.44) | 84.5 (27.8) |
| Ivacaftor | 1.17 (0.424) | 13.7 (6.06) | 11.3 (4.60) |
Absorption
After a single dose in healthy subjects in the fed state, tezacaftor was absorbed with a median (range) time to maximum concentration (t max ) of approximately 4 hours (2 to 6 hours). The median (range) t max of ivacaftor was approximately 6 hours (3 to 10 hours) in the fed state.
When a single dose of tezacaftor/ivacaftor was administered with fat-containing foods, tezacaftor exposure was similar and ivacaftor exposure was approximately 3 times higher than when taken in a fasting state.
Distribution
Tezacaftor is approximately 99% bound to plasma proteins, primarily to albumin. Ivacaftor is approximately 99% bound to plasma proteins, primarily to alpha 1-acid glycoprotein and albumin. After oral administration of tezacaftor 100 mg once daily/ivacaftor 150 mg every 12 hours in patients with CF in the fed state, the mean (±SD) for apparent volume of distribution of tezacaftor and ivacaftor was 271 (157) L and 206 (82.9) L, respectively. Neither tezacaftor nor ivacaftor partition preferentially into human red blood cells.
Elimination
After oral administration of tezacaftor 100 mg once daily/ivacaftor 150 mg every 12 hours in patients with CF in the fed state, the mean (±SD) for apparent clearance values of tezacaftor and ivacaftor were 1.31 (0.41) and 15.7 (6.38) L/h, respectively. After steady-state dosing of tezacaftor in combination with ivacaftor in patients with CF, the effective half-lives of tezacaftor and ivacaftor were approximately 15 (3.44) and 13.7 (6.06) hours, respectively.
Metabolism
Tezacaftor is metabolized extensively in humans. In vitro data suggested that tezacaftor is metabolized mainly by CYP3A4 and CYP3A5. Following oral administration of a single dose of 100 mg 14 C-tezacaftor to healthy male subjects, M1, M2, and M5 were the three major circulating metabolites of tezacaftor in humans. M1 has the similar potency to that of tezacaftor and is considered pharmacologically active. M2 is much less pharmacologically active than tezacaftor or M1, and M5 is not considered pharmacologically active. Another minor circulating metabolite, M3, is formed by direct glucuronidation of tezacaftor.
Ivacaftor is also metabolized extensively in humans. In vitro and in vivo data indicate that ivacaftor is metabolized primarily by CYP3A4 and CYP3A5. M1 and M6 are the two major metabolites of ivacaftor in humans. M1 has approximately one-sixth the potency of ivacaftor and is considered pharmacologically active. M6 is not considered pharmacologically active.
Excretion
Following oral administration of 14 C-tezacaftor, the majority of the dose (72%) was excreted in the feces (unchanged or as the M2 metabolite) and about 14% was recovered in urine (mostly as M2 metabolite), resulting in a mean overall recovery of 86% up to 21 days after the dose. Less than 1% of the administrated dose was excreted in urine as unchanged tezacaftor, showing that renal excretion is not the major pathway of tezacaftor elimination in humans.
Following oral administration of ivacaftor alone, the majority of ivacaftor (87.8%) is eliminated in the feces after metabolic conversion. There was minimal elimination of ivacaftor and its metabolites in urine (only 6.6% of total radioactivity was recovered in the urine), and there was negligible urinary excretion of ivacaftor as unchanged drug.
Specific Populations
Based on population PK analyses, the PK exposure parameters of tezacaftor/ivacaftor in children and adolescents (ages 6 to <18 years) are similar to the AUCss range observed in adults when given in combination.
Pediatric patients aged 6 to less than 12 years
| Age Group | Dose | Tezacaftor AUCss mcg∙h/mL AUC 0-24h for tezacaftor and AUC 0-12h for ivacaftor | Ivacaftor AUCss mcg∙h/mL |
|---|---|---|---|
| 6 to <12 years Exposures in ≥ 30 kg weight range are predictions derived from the population PK model | 71.3 (28.3) | 8.5 (3.34) | |
| 6 to <12 years (<30 kg) | tezacaftor 50 mg/ivacaftor 75 mg | 56.7 (22.3) | 6.92 (2.07) |
| 6 to <12 years (≥30 kg) | tezacaftor 100 mg/ivacaftor 150 mg | 92.7 (21.9) | 10.8 (3.52) |
Pediatric patients aged 12 to less than 18 years
Following oral administration of SYMDEKO tablets, tezacaftor 100 mg once daily/ivacaftor 150 mg every 12 hours, the mean (±SD) AUCss for tezacaftor and ivacaftor was 97.1 (35.8) mcg∙h/mL and 11.4 (5.50) mcg∙h/mL, respectively, similar to the mean AUCss in adult patients administered SYMDEKO tablets, tezacaftor 100 mg once daily/ivacaftor 150 mg every 12 hours.
Patients with Hepatic Impairment
Following multiple doses of tezacaftor and ivacaftor for 10 days, patients with moderately impaired hepatic function (Child-Pugh Class B, score 7-9) had an approximately 36% increase in AUC and a 10% increase in C max for tezacaftor, and a 1.5-fold increase in ivacaftor AUC compared with healthy subjects matched for demographics. In a separate study, patients with moderately impaired hepatic function (Child-Pugh Class B, score 7-9) had similar ivacaftor C max , but an approximately 2.0-fold increase in ivacaftor AUC 0-∞ compared with healthy subjects matched for demographics.
Pharmacokinetic studies have not been conducted in patients with mild (Child-Pugh Class A, score 5-6) or severe hepatic impairment (Child-Pugh Class C, score 10-15) receiving SYMDEKO. The magnitude of increase in exposure in patients with severe hepatic impairment is unknown but is expected to be higher than that observed in patients with moderate hepatic impairment [see Dosage and Administration (2.3) , Use in Specific Populations (8.6) , and Patient Counseling Information (17) ] .
Patients with Renal Impairment
SYMDEKO has not been studied in patients with moderate or severe renal impairment (creatinine clearance ≤30 mL/min) or in patients with end-stage renal disease. In a human pharmacokinetic study with tezacaftor alone, there was minimal elimination of tezacaftor and its metabolites in urine (only 13.7% of total radioactivity was recovered in the urine with 0.79% as unchanged drug).
In a human pharmacokinetic study with ivacaftor alone, there was minimal elimination of ivacaftor and its metabolites in urine (only 6.6% of total radioactivity was recovered in the urine).
In population pharmacokinetic analysis, data from 665 patients on tezacaftor or tezacaftor in combination with ivacaftor in clinical trials indicated that mild renal impairment (N=147; eGFR 60 to less than 90 mL/min/1.73 m 2 ) and moderate renal impairment (N=7; eGFR 30 to less than 60 mL/min/1.73 m 2 ) did not affect the clearance of tezacaftor significantly [see Use in Specific Populations (8.7) ] .
Male and Female Patients
The pharmacokinetic parameters of tezacaftor and ivacaftor are similar in males and females.
Drug Interactions Studies
Drug interaction studies were performed with SYMDEKO and other drugs likely to be co-administered or drugs commonly used as probes for pharmacokinetic interaction studies [see Drug Interactions (7) ] .
Potential for Tezacaftor/Ivacaftor to Affect Other Drugs
Clinical studies (with rosiglitazone and desipramine – see Table 9 ) showed that ivacaftor is not an inhibitor of CYP2C8 or CYP2D6. Based on in vitro results, ivacaftor has the potential to inhibit CYP3A and P-gp, and may also inhibit CYP2C9. In vitro , ivacaftor was not an inducer of CYP isozymes. Ivacaftor is not an inhibitor of transporters OATP1B1, OATP1B3, OCT1, OCT2, OAT1, or OAT3.
Based on in vitro results, tezacaftor has a low potential to inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and CYP3A4. Tezacaftor has a low potential to induce CYP3A, but it is not an inducer of CYP1A2 and CYP2B6. Tezacaftor has a low potential to inhibit transporters P-gp, BCRP, OATP1B3, OCT2, OAT1, or OAT3.
Clinical studies with midazolam showed that SYMDEKO is not an inhibitor of CYP3A. Co-administration of SYMDEKO with digoxin, a sensitive P-gp substrate, increased digoxin exposure by 1.3-fold. Co-administration of SYMDEKO with an ethinyl estradiol/ norethindrone oral contraceptive had no significant effect on the exposures of the hormonal contraceptives. Co-administration of SYMDEKO with pitavastatin, an OATP1B1 substrate, had no clinically relevant effect on the exposure of pitavastatin.
The effects of tezacaftor and ivacaftor (or ivacaftor alone) on the exposure of co-administered drugs are shown in Table 9 [see Drug Interactions (7) ] .
Potential for Other Drugs to Affect Tezacaftor/Ivacaftor
In vitro studies showed that ivacaftor and tezacaftor were substrates of CYP3A enzymes ( i.e. , CYP3A4 and CYP3A5). Exposure to ivacaftor and tezacaftor will be reduced by concomitant CYP3A inducers and increased by concomitant CYP3A inhibitors.
In vitro studies showed that tezacaftor is a substrate for the uptake transporter OATP1B1, and efflux transporters P-gp and BCRP. Tezacaftor is not a substrate for OATP1B3. In vitro studies showed that ivacaftor is not a substrate for OATP1B1, OATP1B3, or P-gp.
The effects of co-administered drugs on the exposure of tezacaftor and ivacaftor (or ivacaftor alone) are shown in Table 10 [see Dosage and Administration (2.4) and Drug Interactions (7) ] .
| Dose and Schedule | Mean Ratio (90% CI) of Other Drugs No Effect=1.0 | ||||
|---|---|---|---|---|---|
| Drug | Dose | TEZ/IVA or IVA | Effect on Drug PK | AUC | C max |
| ↑ = increase, ↓ = decrease, ↔ = no change. CI = Confidence interval; TEZ = tezacaftor; IVA = ivacaftor; PK = Pharmacokinetics | |||||
| Midazolam | 2 mg single oral dose | TEZ 100 mg/IVA 150 mg every morning + IVA 150 mg every evening | ↔ Midazolam | 1.12 (1.01, 1.25) | 1.13 (1.01, 1.25) |
| Digoxin | 0.5 mg single dose | TEZ 100 mg/IVA 150 mg every morning + IVA 150 mg every evening | ↑ Digoxin | 1.30 (1.17, 1.45) | 1.32 (1.07, 1.64) |
| Oral Contraceptive | Ethinyl estradiol/ Norethindrone 0.035 mg/1.0 mg once daily | TEZ 100 mg/IVA 150 mg every morning + IVA 150 mg every evening | ↔ Ethinyl estradiol | 1.12 (1.03, 1.22) | 1.15 (0.99, 1.33) |
| ↔ Norethindrone | 1.05 (0.98, 1.12) | 1.01 (0.87, 1.19) | |||
| Pitavastatin | 2 mg single dose | TEZ 100 mg/IVA 150 mg every morning + IVA 150 mg every evening | ↑ Pitavastatin Effect is not clinically significant – no dosage adjustment is necessary | 1.24 (1.17, 1.31) | 0.977 (0.841, 1.14) |
| Rosiglitazone | 4 mg single oral dose | IVA 150 mg twice daily | ↔ Rosiglitazone | 0.975 (0.897, 1.06) | 0.928 (0.858, 1.00) |
| Desipramine | 50 mg single dose | IVA 150 mg twice daily | ↔ Desipramine | 1.04 (0.985, 1.10) | 1.00 (0.939, 1.07) |
| Dose and Schedule | Mean Ratio (90% CI) of Tezacaftor and Ivacaftor No Effect = 1.0 | ||||
|---|---|---|---|---|---|
| Drug | Dose | TEZ/IVA or IVA | Effect on TEZ/IVA PK | AUC | C max |
| ↑ = increase, ↓ = decrease, ↔ = no change. CI = Confidence interval; TEZ = tezacaftor; IVA = ivacaftor; PK = Pharmacokinetics | |||||
| Itraconazole | 200 mg twice a day on Day 1, followed by 200 mg once daily | TEZ 25 mg + IVA 50 mg once daily | ↑ Tezacaftor | 4.02 (3.71, 4.63) | 2.83 (2.62, 3.07) |
| ↑ Ivacaftor | 15.6 (13.4, 18.1) | 8.60 (7.41, 9.98) | |||
| Ciprofloxacin | 750 mg twice daily | TEZ 50 mg + IVA 150 mg twice daily | ↔ Tezacaftor | 1.08 (1.03, 1.13) | 1.05 (0.99, 1.11) |
| ↑ Ivacaftor Effect is not clinically significant – no dosage adjustment is necessary | 1.17 (1.06, 1.30) | 1.18 (1.06, 1.31) | |||
| Oral Contraceptive | Norethindrone/ethinyl estradiol 1.0 mg/0.035 mg once daily | TEZ 100 mg/IVA 150 mg every morning + IVA 150 mg every evening | ↔ Tezacaftor | 1.01 (0.963, 1.05) | 1.01 (0.933, 1.09) |
| ↔ Ivacaftor | 1.03 (0.960, 1.11) | 1.03 (0.941, 1.14) | |||
| Rifampin | 600 mg once daily | IVA 150 mg single dose | ↓ Ivacaftor | 0.114 (0.097, 0.136) | 0.200 (0.168, 0.239) |
| Fluconazole | 400 mg single dose on Day 1, followed by 200 mg once daily | IVA 150 mg twice daily | ↑ Ivacaftor | 2.95 (2.27, 3.82) | 2.47 (1.93, 3.17) |
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies of carcinogenicity, mutagenicity, or impairment of fertility were conducted with the combination of tezacaftor and ivacaftor, however, separate studies of tezacaftor and ivacaftor are described below.
Tezacaftor
A 2-year study in Sprague-Dawley rats and a 6-month study in Tg.rasH2 transgenic mice were conducted to assess the carcinogenic potential of tezacaftor. No evidence of tumorigenicity from tezacaftor was observed in male and female rats at oral doses up to 50 and 75 mg/kg/day (approximately 2 and 3 times the MRHD based on summed AUCs of tezacaftor and its metabolites in males and females, respectively). No evidence of tumorigenicity was observed in male and female Tg.rasH2 transgenic mice at tezacaftor doses up to 500 mg/kg/day.
Tezacaftor was negative for genotoxicity in the following assays: Ames test for bacterial gene mutation, in vitro chromosomal aberration assay in Chinese hamster ovary cells, and in vivo mouse micronucleus test.
There were no effects on male or female fertility and early embryonic development in rats at oral tezacaftor doses up to 100 mg/kg/day (approximately 3 times the MRHD based on summed AUC of tezacaftor and M1 metabolite).
Ivacaftor
Two-year studies were conducted in CD-1 mice and Sprague-Dawley rats to assess the carcinogenic potential of ivacaftor. No evidence of tumorigenicity from ivacaftor was observed in mice or rats at oral doses up to 200 mg/kg/day and 50 mg/kg/day, respectively (approximately equivalent to 2 and 9 times the MRHD, respectively, based on summed AUCs of ivacaftor and its metabolites).
Ivacaftor was negative for genotoxicity in the following assays: Ames test for bacterial gene mutation, in vitro chromosomal aberration assay in Chinese hamster ovary cells, and in vivo mouse micronucleus test.
Ivacaftor impaired fertility and reproductive performance indices in male and female rats at 200 mg/kg/day (approximately 9 and 6 times, respectively, the MRHD based on summed AUCs of ivacaftor and its metabolites). Increases in prolonged diestrus were observed in females at 200 mg/kg/day. Ivacaftor also increased the number of females with all nonviable embryos and decreased corpora lutea, implantations, and viable embryos in rats at 200 mg/kg/day (approximately 6 times the MRHD based on summed AUCs of ivacaftor and its metabolites) when dams were dosed prior to and during early pregnancy. These impairments of fertility and reproductive performance in male and female rats at 200 mg/kg/day were attributed to severe toxicity. No effects on male or female fertility and reproductive performance indices were observed at ≤100 mg/kg/day (approximately 6 and 4 times, respectively, the MRHD based on summed AUCs of ivacaftor and its metabolites).
CLINICAL STUDIES
Dose Ranging :
Dose selection for the clinical program primarily consisted of one double-blind, placebo-controlled, multiple-cohort trial which included 176 patients with CF (homozygous for the F508del mutation) 18 years of age and older with a screening ppFEV1≥40. In the study, 34 and 106 patients, respectively, received tezacaftor at once-daily doses of 10 mg, 30 mg, 100 mg, or 150 mg alone or in combination with ivacaftor 150 mg q12h, and 33 patients received placebo. During the 28-day treatment period, dose-dependent increases in mean ppFEV 1 change from baseline were observed with tezacaftor in combination with ivacaftor. Tezacaftor/ivacaftor in general had a greater mean treatment effect than tezacaftor alone. No additional benefit was observed at tezacaftor doses greater than 100 mg daily.
Efficacy :
The efficacy of SYMDEKO in patients with CF aged 12 years and older was evaluated in three double-blind, placebo-controlled trials (Trials1, 2, and 3).
Trial 1 was a 24-week randomized, double-blind, placebo-controlled, two-arm study in patients with CF who were homozygous for the F508del mutation in the CFTR gene.
Trial 2 was a randomized, double-blind, placebo-controlled, 2-period, 3-treatment, 8-week crossover study in patients with CF who were heterozygous for the F508del mutation and a second mutation predicted to be responsive to tezacaftor/ivacaftor. Mutations predicted to be responsive were selected for the study based on the clinical phenotype (pancreatic sufficiency), biomarker data (sweat chloride), and in vitro responsiveness to tezacaftor/ivacaftor [see Clinical Studies (14.2) ] . Patients were randomized to and received sequences of treatment that included SYMDEKO, ivacaftor, and placebo.
Trial 3 was a 12-week randomized, double-blind, placebo-controlled, two-arm study in patients with CF who were heterozygous for the F508del mutation and a second CFTR mutation predicted to be unresponsive to tezacaftor/ivacaftor. Mutations predicted to be non-responsive were selected for the study based on biologic plausibility (mutation class), clinical phenotype (pancreatic insufficiency), biomarker data (sweat chloride), and in vitro testing to tezacaftor and/or ivacaftor.
Patients in all trials continued on their standard-of-care CF therapies (e.g . , bronchodilators, inhaled antibiotics, dornase alfa, and hypertonic saline) and were eligible to roll over into a 96-week open-label extension. Patients had a ppFEV 1 at screening between 40-90%. Patients with a history of colonization with organisms associated with a more rapid decline in pulmonary status such as Burkholderia cenocepacia , Burkholderia dolosa , or Mycobacterium abscessus , or who had 2 or more abnormal liver function tests at screening (ALT, AST, AP, GGT ≥3 × ULN or total bilirubin ≥2 × ULN) or AST or ALT ≥5 × ULN, were excluded from the trials.
Trial in Patients with CF Who Were Homozygous for the F508del Mutation in the CFTR Gene (Trial 1)
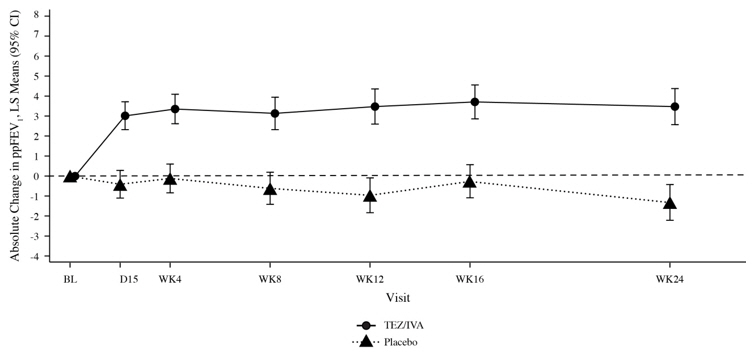
Trial 1 evaluated 504 patients (248 SYMDEKO, 256 placebo) with CF aged 12 years and older (mean age 26.3 years). The mean ppFEV 1 at baseline was 60.0% (range: 27.8% to 96.2%). The primary efficacy endpoint was change in lung function as determined by absolute change from baseline in ppFEV 1 through Week 24. Treatment with SYMDEKO resulted in a statistically significant improvement in ppFEV 1 . The treatment difference between SYMDEKO and placebo for the mean absolute change in ppFEV 1 from baseline through Week 24 was 4.0 percentage points (95% CI: 3.1, 4.8; P< 0.0001). These changes persisted throughout the 24-week treatment period (Figure 1). Improvements in ppFEV 1 were observed regardless of age, sex, baseline ppFEV 1 , colonization with Pseudomonas , concomitant use of standard-of-care medications for CF, and geographic region.
Key secondary efficacy variables included relative change from baseline in ppFEV 1 through Week 24; number of pulmonary exacerbations from baseline through Week 24; absolute change in BMI from baseline at Week 24, and absolute change in CFQ-R Respiratory Domain Score (a measure of respiratory symptoms relevant to patients with CF, such as cough, sputum production, and difficulty breathing) from baseline through Week 24. For the purposes of this trial, a pulmonary exacerbation was defined as a change in antibiotic therapy (IV, inhaled, or oral) as a result of 4 or more of 12 pre-specified sino-pulmonary signs/symptoms. See Table 11 for a summary of key secondary outcomes in Trial 1.
| Placebo N=256 | SYMDEKO N=248 | ||
|---|---|---|---|
| BMI: body mass index; CI: confidence interval; CFQ-R: Cystic Fibrosis Questionnaire-Revised; IVA: ivacaftor; NA: not applicable; ppFEV 1 : percent predicted forced expiratory volume in 1 second; | |||
| Relative change in ppFEV 1 from baseline through Week 24 (%) | Treatment difference (95% CI) | - | 6.8 (5.3, 8.3) |
| P value | NA | P< 0.0001 Indicates statistical significance confirmed in the hierarchical testing procedure. Other efficacy measures considered not statistically significant. | |
| Number of pulmonary exacerbations from baseline through Week 24 | Number of events (event rate per year Estimated event rate per year calculated using 48 weeks per year. ) Rate ratio (95% CI) | 122 (0.99) | 78 (0.64) 0.65 (0.48, 0.88) |
| P value | NA | P =0.0054 | |
| Absolute change in BMI from baseline at Week 24 (kg/m 2 ) | Treatment difference (95% CI) | - | 0.06 (-0.08, 0.19) |
| Absolute change in CFQ-R Respiratory Domain Score from baseline through Week 24 (points) | Treatment difference (95% CI) | - | 5.1 (3.2, 7.0) |
Figure 1: Absolute Change From Baseline in Percent Predicted FEV 1 at Each Visit in Trial 1
Trial in Patients with CF Who Were Heterozygous for the F508del Mutation and a Second Mutation Predicted to be Responsive to Tezacaftor/Ivacaftor (Trial 2)
Trial 2 evaluated 244 patients with CF aged 12 years and older (mean age 34.8 years). The mean ppFEV 1 at baseline was 62.3% (range: 34.6 to 93.5). Of the 244 patients included in the efficacy analysis, 146 patients had a splice mutation and 98 patients had a missense mutation as the second allele. 161 patients received SYMDEKO, 156 patients received ivacaftor, and 161 patients received placebo. The primary efficacy endpoint was the mean absolute change from study baseline in percent predicted FEV 1 averaged at Weeks 4 and 8 of treatment. The key secondary efficacy endpoint was absolute change in CFQ-R Respiratory Domain Score from study baseline averaged at Weeks 4 and 8 of treatment. For the overall population, treatment with SYMDEKO compared to placebo resulted in significant improvement in ppFEV 1 (6.8 percentage points [95% CI: 5.7, 7.8]; P <0.0001) and CFQ-R Respiratory Domain Score (11.1 points (95% CI: 8.7, 13.6); P <0.0001). Treatment difference for ppFEV 1 between ivacaftor- and placebo-treated patients was 4.7 percentage points (95% CI: 3.7, 5.8; P <0.0001) and 2.1 percentage points (95% CI: 1.2, 2.9; P <0.0001) between SYMDEKO- and ivacaftor-treated patients, which were statistically significant. Improvements in ppFEV 1 were observed regardless of age, baseline ppFEV 1 , sex, mutation class, colonization with Pseudomonas , concomitant use of standard-of-care medications for CF, and geographic region. Statistically significant improvements compared to placebo were also observed in the subgroup of patients with splice mutations and missense mutations (Table 12).
| Mutation (n) | Absolute Change in percent predicted FEV 1 Average of Week 4 and 8 values. Absolute change in ppFEV 1 by individual mutations is an ad hoc analysis. | Absolute Change in CFQ-R Respiratory Domain Score (Points) Absolute change in CFQ-R Respiratory Domain Score and absolute change in sweat chloride by mutation subgroups and by individual mutations are ad hoc analyses. | Absolute Change in Sweat Chloride (mmol/L) |
|---|---|---|---|
| (n=) patient numbers analysed. | |||
| Splice mutations (n= 93 for TEZ/IVA, n=97 for PBO) Results shown as difference in mean (95% CI) change from study baseline for SYMDEKO vs. placebo-treated patients: | |||
| 7.4 (6.0, 8.7) | 9.5 (6.3, 12.7) | -5.4 (-8.0, -2.7) | |
| By individual splice mutation (n). Results shown as mean (minimum, maximum) for change from study baseline for SYMDEKO-treated patients | |||
| 2789+5G→A (25) | 8.6 (-1.5, 23.4) | 12.0 (-8.3, 38.9) | -3.2 (-16.5, 9.0) |
| 3272-26A→G (23) | 5.7 (-2.1, 25.9) | 5.7 (-22.2, 44.4) | -3.8 (-22.3, 16.5) |
| 3849+10kbC→T (43) | 5.8 (-7.2, 22.3) | 8.2 (-25.0, 47.2) | -5.6 (-27.0, 8.5) |
| 711+3A→G (2) | 4.3 (2.0, 6.7) | -4.2 (-5.6, -2.8) | -15.4 (-21.0, -9.8) |
| E831X Patients enrolled did not receive tezacaftor/ivacaftor treatment. (0) | NA | NA | NA |
| Missense mutations (n=66 for TEZ/IVA, n=63 for PBO) Results shown as difference in mean (95% CI) change from study baseline for SYMDEKO vs. placebo-treated patients: | |||
| 5.9 (4.2, 7.5) | 13.4 (9.6, 17.3) | -16.3 (-19.7, -12.9) | |
| By individual missense mutation (n). Results shown as mean (minimum, maximum) for change from study baseline for SYMDEKO-treated patients | |||
| D579G (2) | 8.1 (-0.2, 16.4) | 11.1 (5.6, 16.7) | -23.1 (-24.8, -21.5) |
| D110H (1) | -1.0 (-1.0, -1.0) | -11.1 (-11.1, -11.1) | -22.5 (-22.5, -22.5) |
| D1152H (21) | 3.8 (-2.5, 12.5) | 15.2 (-8.3, 55.6) | -4.1 (-15.0, 11.5) |
| A455E (11) | 8.5 (2.6, 16.1) | 11.6 (-11.1, 44.4) | -0.3 (-8.8, 14.0) |
| L206W (4) | 3.0 (-4.5, 10.2) | 12.5 (-2.8, 38.9) | -36.1 (-44.5, -27.5) |
| P67L (11) | 9.4 (0.0, 31.9) | 11.7 (-12.5, 72.2) | -29.3 (-50.0, 0.8) |
| R1070W (2) | 6.1 (2.0, 10.1) | 29.2 (16.7, 41.7) | -13.8 (-26.8, -0.8) |
| R117C (1) | 2.9 (2.9, 2.9) | 16.7 (16.7, 16.7) | -38.8 (-38.8, -38.8) |
| R347H (2) | -0.5 (-2.8, 1.7) | 5.6 (-5.6, 16.7) | -13.8 (-19.0, -8.5) |
| R352Q (2) | 4.9 (2.6, 7.1) | 8.3 (8.3, 8.3) | -43.3 (-49.8, -36.8) |
| S945L (7) | 9.6 (0.7, 19.5) | 11.3 (-4.2, 25.0) | -29.0 (-42.5, -8.0) |
| S977F (2) | 10.1 (5.5, 14.7) | -1.4 (-8.3, 5.6) | -13.9 (-22.3, -5.5) |
In an analysis of BMI at Week 8, an exploratory endpoint, patients treated with SYMDEKO had a mean improvement of 0.2 kg/m 2 (95% CI [0.0, 0.3]), 0.1 kg/m 2 (95% CI [-0.1, 0.3]), and 0.3 kg/m 2 (95% CI [0.1, 0.5]) versus placebo for the overall, splice, and missense mutation populations of patients, respectively.
Trial in Patients with CF Who Were Heterozygous for the F508del Mutation and a Second Mutation Not Predicted to be Responsive to Tezacaftor/Ivacaftor (Trial 3)
Trial 3 evaluated 168 patients with CF (83 SYMDEKO and 85 placebo) aged 12 years and older (mean age 26.1 years) who were heterozygous for the F508del mutation and had a second CFTR mutation predicted to be unresponsive to tezacaftor/ivacaftor. CF patients with the F508del mutation and one of the following mutations in the CFTR gene were enrolled in the study (listed in decreasing frequency): W1282X, G542X, N1303K, 621+1G>T, 1717-1G>A, 1898+1G>A, CFTRdele2,3 , 2183delAA>G , 2184insA , R1162X , R553X, 3659delC, 3905insT, G970R, I507del, R1066C, R347P, 1154insTC, 1811+1.6kbA>G, 2184delA, 405+1G>A, E60X, G85E, L1077P, Q39X, S466X, Y1092X, 1078delT, 1248+1G>A, 1677delTA, 1812-1G>A, 2869INSG, 3120+1G>A, 394delTT, 457TAT>G, 711+1G>T, 711+5G>A, 712-1G>T, G673x, L1065P, Q220X, Q493X, R709X, V520F. The mean ppFEV 1 at baseline was 57.5% [range: 31.0 to 96.7]. The primary efficacy endpoint was changed from baseline in absolute ppFEV 1 through Week 12. The overall treatment difference between SYMDEKO and placebo for the mean absolute change in ppFEV 1 from baseline through Week 12 was 1.2 percentage points (95% CI: -0.3, 2.6). This study was terminated following the planned interim analysis because the pre-specified futility criteria were met.
HOW SUPPLIED/STORAGE AND HANDLING
SYMDEKO (tezacaftor 50 mg/ivacaftor 75 mg fixed-dose combination tablets co-packaged with ivacaftor 75 mg tablet):
- Tezacaftor 50 mg/ivacaftor 75 mg fixed-dose combination tablets are supplied as white, oblong-shaped tablets containing 50 mg of tezacaftor and 75 mg of ivacaftor. Each tablet is debossed with "V50" on one side and plain on the other.
- Ivacaftor 75 mg tablets are supplied as light blue, film-coated, oblong-shaped tablets containing 75 mg of ivacaftor. Each tablet is printed with the characters "V 75" on one side and plain on the other.
- 56-count tablet carton containing a 4-week supply (4 weekly wallets, each with 14 tablets) NDC 51167-113-01
SYMDEKO (tezacaftor 100 mg/ivacaftor 150 mg fixed-dose combination tablets co-packaged with ivacaftor 150 mg tablet):
- Tezacaftor 100 mg/ivacaftor 150 mg fixed-dose combination tablets are supplied as yellow, oblong-shaped tablets containing 100 mg of tezacaftor and 150 mg of ivacaftor. Each tablet is debossed with "V100" on one side and plain on the other.
- Ivacaftor 150 mg tablets are supplied as light blue, film-coated, oblong-shaped tablets containing 150 mg of ivacaftor. Each tablet is printed with the characters "V 150" on one side and plain on the other.
- 56-count tablet carton containing a 4-week supply (4 weekly wallets, each with 14 tablets) NDC 51167-661-01
Store at 68°F to 77°F (20°C to 25°C); excursions permitted to 59°F to 86°F (15°C to 30°C) [see USP Controlled Room Temperature].
Mechanism of Action
Tezacaftor facilitates the cellular processing and trafficking of select mutant forms of CFTR (including F508del-CFTR) to increase the amount of mature CFTR protein delivered to the cell surface. Ivacaftor is a CFTR potentiator that facilitates increased chloride transport by potentiating the channel-open probability (or gating) of the CFTR protein at the cell surface. For ivacaftor to function CFTR protein must be present at the cell surface. Ivacaftor can potentiate the CFTR protein delivered to the cell surface by tezacaftor, leading to a further enhancement of chloride transport than either agent alone. The combined effect of tezacaftor and ivacaftor is increased quantity and function of CFTR at the cell surface, resulting in increases in chloride transport.
CFTR Chloride Transport Assay in Fischer Rat Thyroid (FRT) cells expressing mutant CFTR
The chloride transport response of mutant CFTR protein to tezacaftor/ivacaftor was determined in Ussing chamber electrophysiology studies using a panel of FRT cell lines transfected with individual CFTR mutations. Tezacaftor/ivacaftor increased chloride transport in FRT cells expressing CFTR mutations that result in CFTR protein being delivered to the cell surface.
The in vitro chloride transport response threshold was designated as a net increase of at least 10% of normal over baseline because it is predictive or reasonably expected to predict clinical benefit. For individual mutations, the magnitude of the net change over baseline in CFTR-mediated chloride transport in vitro is not correlated with the magnitude of clinical response.
Note that splice site mutations cannot be studied in the FRT assay.
Table 6 lists responsive CFTR mutations based on (1) a clinical FEV 1 response and/or (2) in vitro data in FRT cells, indicating that tezacaftor/ivacaftor increases chloride transport to at least 10% of normal over baseline. CFTR gene mutations that are not responsive to ivacaftor alone are not expected to respond to SYMDEKO except for F508del homozygotes.
| 546insCTA | E92K | G576A | L346P | R117G | S589N |
| 711+3A→G Clinical data for these mutations in Clinical Studies [see Clinical Studies (14.1 and 14.2) ] . | E116K | G576A;R668C Complex/compound mutations where a single allele of the CFTR gene has multiple mutations; these exist independent of the presence of mutations on the other allele. | L967S | R117H | S737F |
| 2789+5G→A | E193K | G622D | L997F | R117L | S912L |
| 3272-26A→G | E403D | G970D | L1324P | R117P | S945L |
| 3849+10kbC→T | E588V | G1069R | L1335P | R170H | S977F |
| A120T | E822K | G1244E | L1480P | R258G | S1159F |
| A234D | E831X | G1249R | M152V | R334L | S1159P |
| A349V | F191V | G1349D | M265R | R334Q | S1251N |
| A455E | F311del | H939R | M952I | R347H | S1255P |
| A554E | F311L | H1054D | M952T | R347L | T338I |
| A1006E | F508C | H1375P | P5L | R347P | T1036N |
| A1067T | F508C;S1251N | I148T | P67L | R352Q | T1053I |
| D110E | F508del A patient must have two copies of the F508del mutation or at least one copy of a responsive mutation presented in Table 6 to be indicated. | I175V | P205S | R352W | V201M |
| D110H | F575Y | I336K | Q98R | R553Q | V232D |
| D192G | F1016S | I601F | Q237E | R668C | V562I |
| D443Y | F1052V | I618T | Q237H | R751L | V754M |
| D443Y;G576A;R668C | F1074L | I807M | Q359R | R792G | V1153E |
| D579G | F1099L | I980K | Q1291R | R933G | V1240G |
| D614G | G126D | I1027T | R31L | R1066H | V1293G |
| D836Y | G178E | I1139V | R74Q | R1070Q | W1282R |
| D924N | G178R | I1269N | R74W | R1070W | Y109N |
| D979V | G194R | I1366N | R74W;D1270N | R1162L | Y161S |
| D1152H | G194V | K1060T | R74W;V201M | R1283M | Y1014C |
| D1270N | G314E | L15P | R74W;V201M;D1270N | R1283S | Y1032C |
| E56K | G551D | L206W | R75Q | S549N | |
| E60K | G551S | L320V | R117C | S549R |