Get your patient on Atropine - Atropine Sulfate solution/ Drops (Atropine Sulfate)
Atropine - Atropine Sulfate solution/ Drops prescribing information
INDICATIONS AND USAGE
Atropine sulfate ophthalmic solution, 1% is indicated in adults and pediatric patients aged three (3) months and older for:
Cycloplegia
Mydriasis
Penalization of the Healthy Eye in the Treatment of Amblyopia
DOSAGE AND ADMINISTRATION
- Apply 1 drop topically to the cul-de-sac of the conjunctiva, forty minutes prior to the intended maximal dilation time.
- In adults and pediatric patients aged 3 years and older, doses may be repeated up to twice daily as needed.
DOSAGE FORMS AND STRENGTHS
Ophthalmic Solution: 1% atropine sulfate, USP.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
There are no adequate and well-controlled studies of atropine sulfate administration in pregnant women to inform a drug-associated risk. Adequate animal development and reproduction studies have not been conducted with atropine sulfate. In humans, 1% atropine sulfate is systemically bioavailable following topical ocular administration [see Clinical Pharmacology (12.3)] .
Atropine sulfate ophthalmic solution, 1% should only be used during pregnancy if the potential benefit justifies the potential risk to the fetus.
Lactation
Risk Summary
There is no information to inform risk regarding the presence of atropine in human milk following ocular administration of atropine sulfate to the mother. The effects on breastfed infants and the effects on milk production are also unknown. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for atropine sulfate and any potential adverse effects on the breastfed child from atropine sulfate.
Pediatric Use
The safety and effectiveness of atropine sulfate ophthalmic solution, 1% have been established in pediatric patients aged 3 months and older. Use of atropine sulfate ophthalmic solution, 1% is supported by evidence from adequate and well-controlled trials with additional safety data from published literature.
Due to the potential for systemic absorption, the use of atropine sulfate ophthalmic solution, 1% in pediatric patients aged 3 months to 3 years should be limited to no more than one drop per eye per day.
Use in pediatric patients younger than 3 months of age is not recommended.
Geriatric Use
No overall differences in safety and effectiveness have been observed between elderly and younger adult patients.
CONTRAINDICATIONS
Hypersensitivity
Atropine sulfate ophthalmic solution, 1% is contraindicated in patients who have demonstrated a previous hypersensitivity or known allergic reaction to any ingredient of the formulation.
WARNINGS AND PRECAUTIONS
Photophobia and Blurred Vision
Photophobia and blurred vision due to pupil unresponsiveness and cycloplegia may last up to 2 weeks.
Elevation of Blood Pressure
Elevations in blood pressure from systemic absorption has been reported following conjunctival instillation of recommended doses of atropine sulfate ophthalmic solution, 1%.
Risk of Contamination
Do not touch the dropper tip to the eye, eyelids, or any other surface as this may contaminate the solution.
ADVERSE REACTIONS
The following serious adverse reactions are described below and elsewhere in the labeling:
- Photophobia and Blurred Vision [see Warnings and Precautions (5.1) ]
- Elevation in Blood Pressure [see Warnings and Precautions (5.2) ]
The following adverse reactions were identified in clinical studies or post-marketing reports following use of atropine sulfate ophthalmic solution. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Ocular Adverse Reactions
Eye pain and stinging occurs upon instillation. Other commonly occurring adverse reactions include, blurred vision, photophobia, superficial keratitis and decreased lacrimation. Allergic reactions such as papillary conjunctivitis, contact dermatitis and lid edema may also occur less commonly.
Systemic Adverse Reactions
Systemic effects of atropine are related to its anti-muscarinic activity. Systemic adverse events reported include dryness of skin, mouth and throat from decreased secretions from mucus membranes; restlessness, irritability or delirium from stimulation of the central nervous system; tachycardia; flushed skin of the face and neck.
DRUG INTERACTIONS
Monoamine Oxidase Inhibitors (MAOI)
The use of atropine and monoamine oxidase inhibitors (MAOI) is generally not recommended because of the potential to precipitate hypertensive crisis.
DESCRIPTION
Atropine Sulfate Ophthalmic Solution USP, 1% contains atropine, an anticholinergic, in a sterile colorless, clear solution for topical ophthalmic use. The active ingredient is represented by the chemical structure:
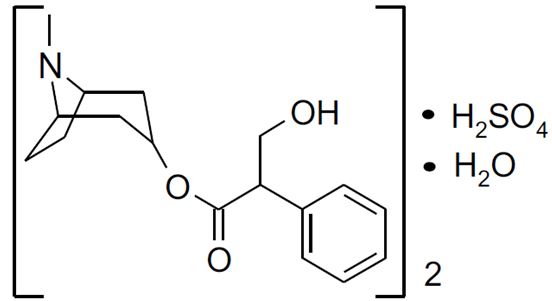
Chemical Name: Benzeneacetic acid, α-(hydroxymethyl)-, 8-methyl-8-azabicyclo-[3.2.1]oct-3-yl ester, endo –(±), sulfate (2:1) (salt), monohydrate.
Molecular Formula: (C 17 H 23 NO 3 ) 2 • H 2 SO 4 • H 2 O
Molecular Weight: 694.83 g/mol
Each mL of atropine sulfate ophthalmic solution USP, 1% contains:
Active: atropine sulfate, USP 10 mg equivalent to 8.3 mg of atropine.
Inactives: benzalkonium chloride 0.1 mg (0.01%), dibasic sodium phosphate, edetate disodium, hypromellose (2910), monobasic sodium phosphate, hydrochloric acid and/or sodium hydroxide may be added to adjust pH (3.5 to 6.0) and water for injection USP.
CLINICAL PHARMACOLOGY
Mechanism of Action
Atropine is a reversible antagonist of muscarine-like actions of acetyl-choline and is therefore classified as an antimuscarinic agent. Atropine is relatively selective for muscarinic receptors. Its potency at nicotinic receptors is much lower, and actions at non-muscarinic receptors are generally undetectable clinically. Atropine does not distinguish among the M1, M2 and M3 subgroups of muscarinic receptors.
The pupillary constrictor muscle depends on muscarinic cholinoceptor activation. This activation is blocked by topical atropine resulting in unopposed sympathetic dilator activity and mydriasis. Atropine also weakens the contraction of the ciliary muscle, or cycloplegia. Cycloplegia results in loss of the ability to accommodate such that the eye cannot focus for near vision.
Pharmacodynamics
The onset of action after administration of atropine sulfate ophthalmic solution, 1%, is usually within 40 minutes with maximal effect being reached in about 2 hours. The effect can last for up to 2 weeks in a normal eye.
Pharmacokinetics
The bioavailability of atropine sulfate ophthalmic solution, 1% was assessed in six healthy subjects, 24 to 29 years of age. Subjects received either 0.3 mg atropine sulfate administered as bolus intravenous injection or 0.3 mg administered as 30 μL instilled unilaterally in the cul-de-sac of the eye. Plasma l-hyoscyamine concentrations were determined over selected intervals up to eight hours after dose administration.
The mean bioavailability of topically applied atropine was 63.5 ± 29% (range 19% to 95%) with large inter-individual differences. Mean maximum observed plasma concentration for the ophthalmic solution was 288 ± 73 pg/mL. Maximum concentration was reached in 28 ± 27 min after administration. Terminal half-life of l-hyoscamine was not affected by route of administration and was calculated to be 3 ± 1.2 hours (intravenous) and 2.5 ± 0.8 hours (topical ophthalmic).
In another placebo-controlled study, the systemic exposure to l-hyoscyamine, and the anti-cholinergic effects of atropine were investigated in eight ocular surgery patients 56 to 66 years of age, following single topical ocular 0.4 mg atropine dose (given as 40 microliters of atropine sulfate ophthalmic solution, 1%). The mean (± standard deviation (SD)) C max of l-hyoscyamine in these patients was 860 ± 402 pg/mL, achieved within 8 minutes of eyedrop instillation.
Following intravenous administration, the mean (± SD) elimination half-life (t 1/2 ) of atropine was reported to be longer in pediatric subjects under 2 years (6.9 ± 3.3 hours) and in geriatric patients 65 to 75 years (10.0 ± 7.3 hours), compared to in children over 2 years (2.5 ± 1.2 hours) and in adults 16 to 58 years (3.0 ± 0.9 hours) [see Use in Specific Populations (8.4) ] .
Atropine is destroyed by enzymatic hydrolysis, particularly in the liver; from 13% to 50% is excreted unchanged in the urine. Traces are found in various secretions, including milk. The major metabolites of atropine are noratropine, atropin-n-oxide, tropine and tropic acid. Atropine readily crosses the placental barrier and enters the fetal circulation, but is not found in amniotic fluid.
Atropine binds poorly (about 44%) to plasma protein, mainly to alpha-1 acid glycoprotein; age has no effect on the serum protein binding of atropine. Atropine binding to α-1 acid glycoprotein was concentration dependent (2 mcg/mL to 20 mcg/mL) and nonlinear in vitro and in vivo . There is no gender effect on the pharmacokinetics of atropine administered by injection.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Long term studies in animals have not been performed to evaluate the carcinogenic potential of atropine sulfate.
Mutagenesis
Atropine sulfate was negative in the salmonella/microsome mutagenicity test.
Impairment of Fertility
Studies to evaluate impairment of fertility have not been conducted.
CLINICAL STUDIES
Topical administration of atropine sulfate ophthalmic solution, 1% results in cycloplegia and mydriasis which has been demonstrated in several controlled clinical studies in adults and pediatric patients. Maximal mydriasis usually occurs in about 40 minutes and maximal cycloplegia is usually achieved in about 60 to 90 minutes after single administration. Full recovery usually occurs in approximately one week, but may last a couple of weeks.
HOW SUPPLIED/STORAGE AND HANDLING
Atropine Sulfate Ophthalmic Solution USP, 1% is supplied sterile in white opaque low density polyethylene plastic bottles and natural low density polyethylene tips with red high density polyethylene caps in the following sizes:
2 mL in 5 mL Container: NDC 60219-1748-2
5 mL in 5 mL Container: NDC 60219-1749-3
15 mL in 15 mL Container: NDC 60219-1750-8
Storage: Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature]. Keep tightly closed. After opening, Atropine Sulfate Ophthalmic Solution can be used until the expiration date on the bottle.
Mechanism of Action
Atropine is a reversible antagonist of muscarine-like actions of acetyl-choline and is therefore classified as an antimuscarinic agent. Atropine is relatively selective for muscarinic receptors. Its potency at nicotinic receptors is much lower, and actions at non-muscarinic receptors are generally undetectable clinically. Atropine does not distinguish among the M1, M2 and M3 subgroups of muscarinic receptors.
The pupillary constrictor muscle depends on muscarinic cholinoceptor activation. This activation is blocked by topical atropine resulting in unopposed sympathetic dilator activity and mydriasis. Atropine also weakens the contraction of the ciliary muscle, or cycloplegia. Cycloplegia results in loss of the ability to accommodate such that the eye cannot focus for near vision.