Get your patient on Bijuva (Estradiol And Progesterone)
Bijuva patient education
Patient toolkit
Dosage & administration

Bijuva prescribing information
| Boxed Warning, Cardiovascular Disorders, Probable | |
| Dementia, Breast Cancer, and Endometrial Cancer | removed 2/2026 |
| Dosage and Administration (2 ) | 2/2026 |
| Contraindications (4 ) | 2/2026 |
| Warnings and Precautions, Cardiovascular Disorders (5.1 ) | 2/2026 |
| Warnings and Precautions, Malignant Neoplasms (5.2 ) | 2/2026 |
| Warnings and Precautions, Probable Dementia | removed 2/2026 |
| Warnings and Precautions, Addition of a Progestogen | |
| When a Woman Has Not Had a Hysterectomy | removed 2/2026 |
INDICATIONS AND USAGE
BIJUVA is a combination of an estrogen and progesterone indicated in a woman with a uterus for the treatment of moderate to severe vasomotor symptoms due to menopause. (1.1 )
Treatment of Moderate to Severe Vasomotor Symptoms Due to Menopause
DOSAGE AND ADMINISTRATION
The timing of BIJUVA initiation can affect the overall risk-benefit profile. Consider initiating BIJUVA in women < 60 years old or < 10 years from onset of menopause [see Warnings and Precautions (5) , Adverse Reactions (6.1) , Use in Specific Populations (8.5) and Clinical Studies (14) ] .
Take a single BIJUVA capsule orally each evening with food. Generally, start therapy with BIJUVA 0.5 mg estradiol/100 mg progesterone dosage strength. Make dosage adjustment based on the clinical response. Attempt to taper or discontinue BIJUVA at 3 to 6 month intervals.
DOSAGE FORMS AND STRENGTHS
BIJUVA capsules, 0.5 mg/100 mg, are oval shaped, opaque, light pink on one side, dark pink on the other side, and printed with "5C1" in white ink.
BIJUVA capsules, 1 mg/100 mg, are oval shaped, opaque, light pink on one side, dark pink on the other side, and printed with "1C1" in white ink.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
BIJUVA is not indicated for use in pregnancy. There are no data with the use of BIJUVA in pregnant women, however, epidemiologic studies and meta-analyses have not found an increased risk of genital or non-genital birth defects (including cardiac anomalies and limb-reduction defects) following exposure to combined hormonal contraceptives (estrogens and progestins) before conception or during early pregnancy.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Lactation
Risk Summary
Estrogens plus progestogens are present in human milk and can reduce milk production in breast-feeding females. This reduction can occur at any time but is less likely to occur once breast-feeding is well-established. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for BIJUVA and any potential adverse effects on the breastfed child from BIJUVA or from the underlying maternal condition.
Pediatric Use
BIJUVA is not indicated for use in pediatric patients. Clinical studies have not been conducted in the pediatric population.
Geriatric Use
There have not been sufficient numbers of geriatric women involved in clinical studies utilizing BIJUVA to determine whether those over 65 years of age differ from younger women in their response to BIJUVA.
The Women's Health Initiative Studies
In the WHI estrogen plus progestin trial (daily CE [0.625 mg] plus MPA [2.5 mg] versus placebo), there was a higher relative risk of nonfatal stroke and invasive breast cancer in women greater than 65 years of age [see Clinical Studies (14.4) ] .
The Women's Health Initiative Memory Study
In the WHIMS ancillary studies of postmenopausal women 65 to 79 years of age, there was an increased risk of developing probable dementia in women receiving estrogen plus progestin [see Clinical Studies (14.5) ] .
It is unknown whether these findings apply to younger postmenopausal women [see Clinical Studies (14.5) ] . The safety and efficacy of BIJUVA for the prevention of dementia has not been established.
CONTRAINDICATIONS
BIJUVA is contraindicated in women with any of the following conditions:
- Abnormal genital bleeding of unknown etiology [see Warnings and Precautions (5.2) ].
- Breast cancer or a history of breast cancer [see Warnings and Precautions (5.2) ].
- Estrogen-dependent neoplasia [see Warnings and Precautions (5.2) ].
- Active deep vein thrombosis (DVT), pulmonary embolisum (PE), or history of these conditions [see Warnings and Precautions (5.1) ].
- Active arterial thromboembolic disease (for example, stroke, myocardial infarction (MI)), or a history of these conditions [see Warnings and Precautions (5.1) ].
- Known anaphylactic reaction, angioedema, or hypersensitivity to BIJUVA.
- Hepatic impairment or disease [see Warnings and Precautions (5.8) ]
- Known thrombophilic disorders, such as protein C, protein S, or antithrombin deficiency
WARNINGS AND PRECAUTIONS
- Cardiovascular Disorders: Increased risks of PE, DVT, stroke, and MI are reported with estrogen plus progestin therapy. Manage risk factors for arterial vascular disease and/or venous thromboembolisum. Discontinue if an arterial or venous thrombotic or thromboembolic event occurs. (5.1 )
- Malignant Neoplasms: Assess risk and provide surveillance measures for breast cancer, such as breast examinations and mammography. (5.2 )
- Estrogens increase the risk of gallbladder disease. (5.3 )
- Discontinue estrogen if severe hypercalcemia, loss of vision, severe hypertriglyceridemia, or cholestatic jaundice occurs. (5.4 , 5.5 , 5.7 , 5.8 )
- Monitor thyroid function in women on thyroid replacement hormone therapy. (5.9 , 5.15 )
Cardiovascular Disorders
BIJUVA is contraindicated in females with active DVT, PE, arterial thromboembolic disease (e.g., stroke, MI) disease, or a history of these conditions [see Contraindications (4) ] . Immediately discontinue BIJUVA if a PE, DVT, stroke, or MI occurs or is suspected.
If feasible, discontinue BIJUVA at least 4 to 6 weeks before surgery of the type associated with an increased risk of thromboembolism, or during periods of prolonged immobilization.
The safety and efficacy of BIJUVA for the prevention of cardiovascular disorders has not been established [see Clinical Studies (14.4) ] .
The Women's Health Initiative (WHI) estrogen plus progestin trial reported increased risks of PE, DVT, stroke, and MI in postmenopausal women (50 to 79 years of age, average age 63.4 years) during the 5.6 years of treatment with daily oral conjugated estrogens (CE) [0.625 mg] combined with medroxyprogesterone acetate (MPA) [2.5 mg], relative to placebo. Analyses were also conducted in women aged 50-59 years, a group of women more likely to present with new onset of moderate to severe VMS compared to women in other age groups in the trial [see Clinical Studies (14.4) ] .
Only daily oral 0.625 mg CE and 2.5 mg MPA were studied in the estrogen plus progestin trial of the WHI. Therefore, the relevance of the WHI findings regarding adverse cardiovascular events to lower CE plus other MPA doses, other routes of administration, or other estrogen plus progestogen products is not known. Without such data, it is not possible to definitively exclude these risks or determine the extent of these risks for other products.
Venous Thromboembolism
In women aged 50-59 years, the WHI estrogen plus progestin trial reported a relative risk for PE of 2.05 (95% confidence interval [CI], 0.89-4.71) for CE/MPA compared to placebo, with a risk difference of 6 per 10,000 women-years (WYs; 11 versus 5). The relative risk for DVT was 3.01 (95% CI, 1.36-6.66) in those receiving CE/MPA compared to placebo, with a risk difference of 10 per 10,000 WYs (15 versus 5) [see Clinical Studies (14.4) ] .
In the overall study population of women aged 50-79 years (average 63.4 years), the trial reported a relative risk for PE of 1.98 (95% CI, 1.36-2.87) for CE/MPA compared to placebo, with a risk difference of 9 per 10,000 WYs (18 versus 9). The relative risk for DVT was 1.87 (95% CI, 1.37-2.54) for CE/MPA compared to placebo, with a risk difference of 12 per 10,000 WYs (25 versus 14) [see Clinical Studies (14.4) ] .
Stroke
In women aged 50-59 years, the WHI estrogen plus progestin trial reported a relative risk for stroke of 1.51 (95% CI, 0.81-2.82) for CE/MPA compared to placebo, with a risk difference of 5 per 10,000 WYs (15 versus 10) [see Clinical Studies (14.4) ] .
In the overall study population of women aged 50-79 years (average 63.4 years), the WHI estrogen plus progestin trial reported relative risk for stroke of 1.37 (95% CI, 1.07-1.76) for CE/MPA compared to placebo, with a risk difference of 9 per 10,000 WYs (33 versus 24) [see Clinical Studies (14.4) ] .
Coronary Heart Disease
In women 50 to 59 years of age, the WHI estrogen plus progestin trial reported a relative risk for coronary heart disease (CHD) events (defined as nonfatal MI, silent MI, or CHD death) of 1.34 (95% CI, 0.82-2.19) for CE/MPA compared placebo, with a risk difference of 5 per 10,000 WYs (23 versus 17).
In the overall study population of women aged 50-79 years (average 63.4 years), the trial reported a relative risk of CHD of 1.18 (95% CI, 0.95-1.45) for CE/MPA compared to placebo, with a risk difference of 6 per 10,000 WYs (41 versus 35) [see Clinical Studies (14.4) ] .
In the Heart and Estrogen/Progestin Replacement Study (HERS) and open label extension (HERS II), postmenopausal women with documented heart disease (n=2,763, average age 66.7 years) received daily CE (0.625 mg) plus MPA or placebo. In Year 1, there were more CHD events in the CE plus MPA-treated group than placebo; however, rates of CHD events were comparable among both groups for the remainder of the duration of the studies (average total follow-up of 6.8 years). 2, 3
Malignant Neoplasms
Breast Cancer
BIJUVA is contraindicated in women with breast cancer, a history of breast cancer, or estrogen-dependent neoplasia [see Contraindications (4) ].
Discontinue BIJUVA if a hormone-sensitive malignancy is diagnosed.The use of estrogen plus progestin therapy has been reported to result in an increase in abnormal mammograms requiring further evaluation.
Only daily oral CE 0.625 mg and MPA 2.5 mg were studied in the estrogen plus progestin trial of the WHI. Therefore, the relevance of the WHI findings regarding breast cancer to lower CE plus other MPA doses, other routes of administration, or other estrogen plus progestogen products is not known. Without such data, it is not possible to definitively exclude these risks or determine the extent of these risks for other products.
In women 50-59 years of age, the WHI estrogen plus progestin trial reported a relative risk for invasive breast cancer of 1.21 (95% CI, 0.81-1.80) for CE/MPA compared to placebo, with a risk difference of 6 per 10,000 WYs (33 versus 27). In this age group, among those who reported no prior use of hormone therapy, the relative risk was 1.06 (95% CI, 0.67-1.67) for CE/MPA compared to placebo, with a risk difference of 2 per 10,000 WYs (33 versus 31) [see Clinical Studies (14.4) ] .
In the overall study population of women aged 50-79 years (average 63.4 years), the WHI estrogen plus progestin trial reported a relative risk for invasive breast cancer of 1.24 (95% CI, 1.01-1.53) for CE/MPA compared to placebo, with a risk difference of 9 per 10,000 WYs (43 versus 35). In the overall study population, among women who reported prior use of hormone therapy, the relative risk of invasive breast cancer was 1.85 (95% CI, 1.18-2.90) for CE/MPA compared to placebo, with a risk difference of 21 per 10,000 WYs (46 versus 25). Among women who reported no prior use of hormone therapy, the relative risk of invasive breast cancer was 1.09 (95% CI, 0.86-1.39), with a risk difference of 4 per 10,000 WYs (40 versus 36). Invasive breast cancers were larger, were more likely to be node positive, and were diagnosed at a more advanced stage in the CE/MPA group compared with the placebo group. Metastatic disease was rare, with no apparent difference between the two groups. Other prognostic factors, such as histologic subtype, grade and hormone receptor status did not differ between the groups. Extension of the WHI trial also demonstrated increased breast cancer risk associated with estrogen plus progestin therapy [see Clinical Studies (14.4) ] . 1
Consistent with the WHI trial, observational studies have also reported an increased risk of breast cancer with estrogen plus progestin therapy. A large meta-analysis including 24 prospective studies of postmenopausal women comparing current use of estrogen plus progestin products with use duration of 5 to 14 years (average of 9 years) versus never use reported a relative risk for breast cancer of 2.08 (95% CI, 2.02-2.15). These studies have not generally found the risk of breast cancer to be different among the various estrogen plus progestin combinations, doses, or routes of administration. 4
Regarding breast cancer mortality, the WHI estrogen plus progestin trial did not show a statistically significant difference between CE/MPA and placebo. The trial reported a relative risk of 1.35 (95% CI, 0.94-1.95) for CE/MPA compared to placebo, with a risk difference of 1 per 10,000 WYs (5 versus 4) after a median of 19 years of cumulative follow-up [see Clinical Studies (14.4) ] .
Ovarian Cancer
Comparing CE/MPA to placebo, women 50-59 years of age had a relative risk for ovarian cancer of 0.30 (95% CI, 0.06-1.47) and the risk difference was -3 per 10,000 WYs (1 versus 4) [see Clinical Studies (14.4) ] .
In the overall WHI study population of women aged 50-79 years (average 63.4 years), the WHI estrogen plus progestin trial reported a relative risk for ovarian cancer of 1.41 (95% CI, 0.75-2.66) for CE/MPA versus placebo after an average follow-up of 5.6 years. The risk difference was 1 per 10,000 WYs (5 versus 4) [see Clinical Studies (14.4) ] .
A large meta-analysis including 17 prospective studies of postmenopausal women compared current use of estrogen plus progestin products versus never use and reported a relative risk for ovarian cancer of 1.37 (95% CI, 1.26-1.48). The duration of hormone therapy use that was associated with an increased risk of ovarian cancer is unknown. 5
Gallbladder Disease
A 2- to 4-fold increase in the risk of gallbladder disease requiring surgery in postmenopausal women receiving estrogens has been reported.
Hypercalcemia
Estrogen administration may lead to severe hypercalcemia in women with breast cancer and bone metastases. Discontinue estrogens, including BIJUVA if hypercalcemia occurs, and take appropriate measures to reduce the serum calcium level.
Visual Abnormalities
Retinal vascular thrombosis has been reported in women receiving estrogens. Discontinue BIJUVA pending examination if there is a sudden partial or complete loss of vision, or a sudden onset of proptosis, diplopia, or migraine. Permanently discontinue estrogens, including BIJUVA, if examination reveals papilledema or retinal vascular lesions.
Elevated Blood Pressure
In a small number of case reports, substantial increases in blood pressure have been attributed to idiosyncratic reactions to estrogens. In a large, randomized, placebo-controlled clinical trial, a generalized effect of estrogens on blood pressure was not seen.
Exacerbation of Hypertriglyceridemia
In women with pre-existing hypertriglyceridemia, estrogen therapy may be associated with elevations of plasma triglycerides leading to pancreatitis. Discontinue BIJUVA if pancreatitis occurs.
Hepatic Impairment and/or Past History of Cholestatic Jaundice
Estrogens may be poorly metabolized in women with hepatic impairment. Exercise caution in any woman with a history of cholestatic jaundice associated with past estrogen use or with pregnancy. In the case of recurrence of cholestatic jaundice, discontinue BIJUVA.
Exacerbation of Hypothyroidism
Estrogen administration leads to increased thyroid-binding globulin (TBG) levels. Women with normal thyroid function can compensate for the increased TBG by making more thyroid hormone, thus maintaining free T4 and T3 serum concentrations in the normal range. Women dependent on thyroid hormone replacement therapy who are also receiving estrogens may require increased doses of their thyroid replacement therapy. Monitor thyroid function in these women during treatment with BIJUVA to maintain their free thyroid hormone levels in an acceptable range.
Fluid Retention
Estrogens plus progestogens may cause some degree of fluid retention. Monitor any woman with a condition(s) that might predispose her to fluid retention, such as cardiac or renal impairment.
Discontinue estrogen plus progestogen therapy, including BIJUVA, with evidence of medically concerning fluid retention.
Hypocalcemia
Estrogen-induced hypocalcemia may occur in women with hypoparathyroidism. Consider whether the benefits of estrogen therapy, including BIJUVA, outweigh the risks in such women.
Hereditary Angioedema
Exogenous estrogens may exacerbate symptoms of angioedema in women with hereditary angioedema. Consider whether the benefits of estrogen therapy, including BIJUVA, outweigh the risks in such women.
Exacerbation of Other Conditions
Estrogen therapy, including BIJUVA, may cause an exacerbation of asthma, diabetes mellitus, epilepsy, migraine, porphyria, systemic lupus erythematosus, and hepatic hemangiomas.
Consider whether the benefits of estrogen therapy outweigh the risks in women with such conditions.
Laboratory Tests
Serum follicle stimulating hormone (FSH) and estradiol levels have not been shown to be useful in the management of postmenopausal women with moderate to severe vasomotor symptoms.
Drug Laboratory Test Interactions
- Accelerated prothrombin time, partial thromboplastin time, and platelet aggregation time; increased platelet count; increased factors II, VII antigen, VIII antigen, VIII coagulant activity, IX, X, XII, VII-X complex, II-VII-X complex, and beta-thromboglobulin; decreased levels of antifactor Xa and antithrombin III, decreased antithrombin III activity; increased levels of fibrinogen and fibrinogen activity; increased plasminogen antigen and activity.
- Increased thyroid-binding globulin (TBG) levels leading to increased circulating total thyroid hormone as measured by protein-bound iodine (PBI), T4 levels (by column or by radioimmunoassay) or T3 levels by radioimmunoassay. T3 resin uptake is decreased, reflecting the elevated TBG. Free T4 and free T3 concentrations are unaltered. Women on thyroid replacement therapy may require higher doses of thyroid hormone.
- Other binding proteins may be elevated in serum, for example, corticosteroid binding globulin (CBG), sex hormone-binding globulin (SHBG), leading to increased total circulating corticosteroids and sex steroids, respectively. Free hormone concentrations, such as testosterone and estradiol, may be decreased. Other plasma proteins may be increased (angiotensinogen/renin substrate, alpha-1-antitrypsin, ceruloplasmin).
- Increased plasma high-density lipoprotein (HDL) and HDL2 cholesterol subfraction concentrations, reduced low-density lipoprotein (LDL) cholesterol concentrations, increased triglyceride levels.
- Impaired glucose tolerance.
ADVERSE REACTIONS
The following serious adverse reactions are discussed elsewhere in the labeling:
- Cardiovascular Disorders [see Warnings and Precautions (5.1) ].
- Malignant Neoplasms [see Warnings and Precautions (5.2) ].
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of estradiol and progesterone capsules was assessed in a 1-year trial that included 1,835 postmenopausal women (1,684 were treated with estradiol and progesterone capsules once daily and 151 women received placebo). Most women (~70%) in the active treatment groups were treated for ≥ 326 days.
Treatment related adverse reactions with an incidence of ≥ 3% in either BIJUVA (estradiol and progesterone) capsules group and numerically greater than those reported in the placebo group are listed in Table 1.
| Preferred Term | BIJUVA 0.5 mg/100 mg (N=424) | BIJUVA 1 mg/100 mg (N=415) | Placebo (N=151) |
|---|---|---|---|
| Breast tenderness | 17 (4.0) | 43 (10.4) | 1 (0.7) |
| Headache | 17 (4.0) | 14 (3.4) | 1 (0.7) |
| Nausea | 15 (3.5) | 9 (2.2) | 1 (0.7) |
| Vaginal bleeding | 10 (2.4) | 14 (3.4) | 0 |
| Vaginal discharge | 8 (1.9) | 14 (3.4) | 1 (0.7) |
| Pelvic pain | 12 (2.8) | 13 (3.1) | 0 |
Postmarketing Experience
The following additional adverse reactions have been identified during post-approval use of BIJUVA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Gastrointestinal disorders
Abdominal pain and discomfort, abdominal distention, diarrhea, nausea, vomiting.
General disorders and administration site conditions
Fatigue, feeling abnormal, malaise.
Investigations
Weight increased.
Metabolism and nutrition disorders
Fluid retention.
Musculoskeletal and connective tissue disorders
Muscle spasms, pain in extremity.
Nervous system disorders
Dizziness, headache, somnolence.
Psychiatric disorders
Insomnia, sleep disorder.
Reproductive system and breast disorders
Breast pain, breast tenderness, uterine bleeding.
Skin and subcutaneous tissue disorders
Night sweats, pruritus.
Vascular disorders
Hot flush.
DRUG INTERACTIONS
In-vitro and in-vivo studies have shown that estrogens and progestins are metabolized partially by cytochrome P450 3A4 (CYP3A4). Therefore, inducers or inhibitors of CYP3A4 may affect estrogen and progestin drug metabolism. Inducers of CYP3A4 such as St. John's wort (Hypericum perforatum) preparations, phenobarbital, carbamazepine, and rifampin may reduce plasma concentrations of estrogens and progestins, possibly resulting in a decrease in therapeutic effects and/or changes in the uterine bleeding profile. Inhibitors of CYP3A4, such as erythromycin, clarithromycin, ketoconazole, itraconazole, ritonavir and grapefruit juice, may increase plasma concentrations of the estrogen or the progestin or both and may result in adverse reactions.
DESCRIPTION
BIJUVA (estradiol and progesterone) is an oval shaped opaque capsule in which the estradiol is solubilized and the progesterone is micronized and suspended in the mixture of medium chain mono and di-glycerides and lauroyl polyoxyl-32 glycerides.
Each 0.5 mg/100 mg capsule is light pink on one side, dark pink on the other side, and printed with "5C1" in white ink.
Each 1 mg/100 mg capsule is light pink on one side, dark pink on the other side, and printed with "1C1" in white ink.
Estradiol (estra-1,3,5 (10)-triene-3,17β-diol), an estrogen, has a molecular weight of 272.38, and chemical formula C 18 H 24 O 2 .
Progesterone (pregn-4-ene-3, 20-dione) has a molecular weight of 314.47, and chemical formula C 21 H 30 O 2 .
The structural formulas are as follows:
 | Estradiol |
 | Progesterone |
Each BIJUVA (estradiol and progesterone) capsule contains the following inactive ingredients: ammonium hydroxide, ethanol, ethyl acetate, FD&C Red #40, gelatin, glycerin, hydrolyzed gelatin, isopropyl alcohol, lauroyl polyoxyl-32 glycerides, lecithin, medium chain mono and di- glycerides, medium chain triglycerides, polyethylene glycol, polyvinyl acetate phthalate, propylene glycol, purified water, and titanium dioxide.
CLINICAL PHARMACOLOGY
Mechanism of Action
Endogenous estrogens are largely responsible for the development and maintenance of the female reproductive system and secondary sexual characteristics. Although circulating estrogens exist in a dynamic equilibrium of metabolic interconversions, estradiol is the principal intracellular human estrogen and is substantially more potent than its metabolites, estrone and estriol, at the receptor level.
The primary source of estrogen in normally cycling adult women is the ovarian follicle, which secretes 70 to 500 mcg of estradiol daily, depending on the phase of the menstrual cycle. After menopause, most endogenous estrogen is produced by conversion of androstenedione, secreted by the adrenal cortex, to estrone in the peripheral tissues. Thus, estrone and the sulfate conjugated form, estrone sulfate, are the most abundant circulating estrogens in postmenopausal women.
Estrogens act through binding to nuclear receptors in estrogen-responsive tissues. To date, two estrogen receptors have been identified. These vary in proportion from tissue to tissue.
Circulating estrogens modulate the pituitary secretion of the gonadotropins, luteinizing hormone (LH), and FSH, through a negative feedback mechanism. Estrogens act to reduce the elevated levels of these hormones seen in postmenopausal women.
Endogenous progesterone is secreted by the ovary, placenta, and adrenal gland. In the presence of adequate estrogen, progesterone transforms a proliferative endometrium into a secretory endometrium.
Progesterone enhances cellular differentiation and generally opposes the actions of estrogens by decreasing estrogen receptor levels, increasing local metabolism of estrogens to less active metabolites, or inducing gene products that blunt cellular responses to estrogen. Progesterone exerts its effects in target cells by binding to specific progesterone receptors that interact with progesterone response elements in target genes. Progesterone receptors have been identified in the female reproductive tract, breast, pituitary, hypothalamus, and central nervous system.
Pharmacodynamics
Generally, a serum estrogen concentration does not predict an individual woman's therapeutic response to BIJUVA nor her risk for adverse outcomes. Likewise, exposure comparisons across different estrogen products to infer efficacy or safety for the individual woman may not be valid.
Pharmacokinetics
Absorption
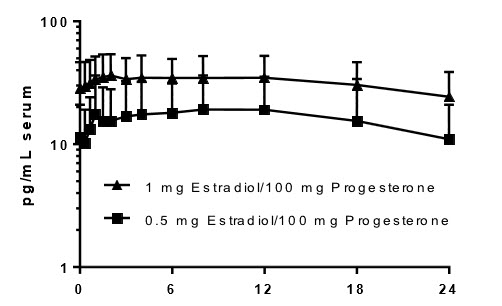
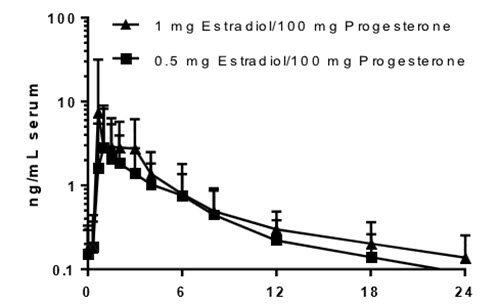
The oral absorption of both estradiol and progesterone is subject to first-pass metabolism. After multiple doses of BIJUVA (estradiol and progesterone) capsules administered with food, the t max (the time at which the maximum concentration is attained) for estradiol is approximately 3 to 6 hours and approximately 3 hours for progesterone (Figure 1, Figure 2, and Table 2, below).
Steady state for both estradiol and progesterone components of BIJUVA, as well as estradiol's main metabolite, estrone, is achieved within seven days. A dose-dependent increase in AUC 0-t and C max of estradiol and a slightly more than proportionality increase in AUC 0-t and C max of estrone were observed when the dose of estradiol was increased from 0.5 mg/day to 1 mg/day (Table 2).
Figure 1: Mean Steady-State Serum Estradiol Concentrations Following Daily Oral Administration of 0.5 mg Estradiol/100 mg Progesterone or 1 mg Estradiol/100 mg Progesterone with Food (Baseline Adjusted, at Day 7)
| Estradiol |
 |
| time after dosing (hrs) |
Figure 2: Mean Steady-State Serum Progesterone Concentrations Following Daily Oral Administration of 0.5 mg Estradiol/100 mg Progesterone or 1 mg Estradiol/100 mg Progesterone with Food (Baseline Adjusted, at Day 7)
| Progesterone |
 |
| time after dosing (hrs) |
| Dosage Strength (estradiol/progesterone) | BIJUVA 0.5 mg/100 mg Mean (SD) | BIJUVA 1 mg/100 mg Mean (SD) | ||
|---|---|---|---|---|
| Abbreviations: AUC 0-τ = area under the concentration vs time curve within the dosing interval at steady-state, C avg = average concentration at steady-state, C max = maximum concentration, SD = standard deviation, t max = time to maximum concentration, t ½ = half-life | ||||
| Estradiol | N | N | ||
| AUC 0-τ (pg∙h/mL) | 17 | 386.8 (356.6) | 20 | 772.4 (384.1) |
| C max (pg/mL) | 17 | 23.95 (16.86) | 20 | 42.27 (18.60) |
| C avg (pg/mL) | 17 | 16.64 (14.50) | 19 | 33.99 (14.53) |
| t max (h) Median and range | 17 | 6.00 (0.00 – 12.00) | 19 | 3.00 (0.67 – 18.03) |
| t ½ (h) Effective t½. Calculated as 24∙ln(2)/ ln (accumulation ratio/(accumulation ratio-1)) for subjects with accumulation ratio >1. | 11 | 28.01 (9.99) | 19 | 26.47 (14.61) |
| Estrone | ||||
| AUC 0-τ (pg∙h/mL) | 17 | 1981 (976.0) | 20 | 4594 (2138) |
| C max (pg/mL) | 17 | 108.0 (48.58) | 20 | 238.5 (100.4) |
| C avg (pg/mL) | 17 | 82.81 (40.80) | 20 | 192.1 (89.43) |
| t max (h) | 17 | 11.98 (2.00 – 18.00) | 20 | 5.00 (1.50 – 12.00) |
| t ½ (h) | 17 | 20.46 (5.61) | 19 | 22.37 (7.64) |
| Progesterone | ||||
| AUC 0-τ (ng∙h/mL) | 17 | 12.19 (11.01) | 20 | 18.05 (15.58) |
| C max (ng/mL) | 17 | 4.40 (5.72) | 20 | 11.31 (23.10) |
| C avg (ng/mL) | 17 | 0.55 (0.45) | 20 | 0.76 (0.65) |
| t max (h) | 17 | 2.00 (0.67 – 8.00) | 20 | 2.51 (0.67 – 6.00) |
| t ½ (h) | 13 | 8.77 (2.78) | 18 | 9.98 (2.57) |
Food Effect
Concomitant food ingestion increased the AUC and C max of the progesterone component of BIJUVA relative to a fasting state when administered at a dose of 100 mg. In a study where BIJUVA was administered to postmenopausal women at a dose of 1 mg estradiol/100 mg progesterone within 30 minutes of starting a high-fat meal, the C max and AUC of progesterone were 162% and 79% higher, respectively, relative to the fasting state and the median t max of progesterone was delayed from 2 hours to 3 hours. Concomitant food ingestion had no effect on the AUC of the estradiol component of BIJUVA but decreased C max by approximately 54% and delayed median t max from 1 hour to 12 hours.
Distribution
Estradiol
The distribution of exogenous estrogens is similar to that of endogenous estrogens. Estrogens are widely distributed in the body and are generally found in higher concentrations in the sex hormone target organs. Estrogens circulating in the blood largely are bound to SHBG and albumin.
Progesterone
Progesterone is approximately 96% to 99% bound to serum proteins, primarily to serum albumin (50% to 54%) and transcortin (43% to 48%).
Elimination
Following repeat dosing with BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg or 1 mg/100 mg, the half-life of estradiol was 28 ± 10 hours and 26 ± 15 hours, respectively, and the half-life of progesterone was 9 ± 3 hours and 10 ± 3 hours, respectively (Table 2).
Metabolism
Estradiol
Exogenous estrogens are metabolized in the same manner as endogenous estrogens. Circulating estrogens exist in a dynamic equilibrium of metabolic interconversions. These transformations take place mainly in the liver. Estradiol is converted reversibly to estrone, and both can be converted to estriol, the major urinary metabolite. Estrogens also undergo enterohepatic recirculation via sulfate and glucuronide conjugation in the liver, biliary secretion of conjugates into the intestine, and hydrolysis in the intestine followed by reabsorption. In postmenopausal women, a significant portion of the circulating estrogens exist as sulfate conjugates, especially estrone sulfate, which serves as a circulating reservoir for the formation of more active estrogens.
Progesterone
Progesterone is metabolized primarily by the liver largely to pregnanediols and pregnanolones. Pregnanediols and pregnanolones are conjugated in the liver to glucuronide and sulfate metabolites. Progesterone metabolites, which are excreted in the bile, may be deconjugated and may be further metabolized in the intestine via reduction, dehydroxylation, and epimerization.
Excretion
Estradiol
Estradiol, estrone, and estriol are excreted in the urine along with glucuronide and sulfate conjugates.
Progesterone
The glucuronide and sulfate conjugates of pregnanediol and pregnanolone are excreted in the bile and urine. Progesterone metabolites are eliminated mainly by the kidneys. Progesterone metabolites which are excreted in the bile may undergo enterohepatic recycling or may be excreted in the feces.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term continuous administration of natural and synthetic estrogens in certain animal species increases the frequency of carcinomas of the breast, uterus, cervix, vagina, testis, and liver.
Progesterone has not been tested for carcinogenicity in animals by the oral route of administration. When implanted into female mice, progesterone produced mammary carcinomas, ovarian granulosa cell tumors, and endometrial stromal sarcomas. In dogs, long-term intramuscular injections produced nodular hyperplasia and benign and malignant mammary tumors. Subcutaneous or intramuscular injections of progesterone decreased the latency period and increased the incidence of mammary tumors in rats previously treated with a chemical carcinogen.
Progesterone did not show evidence of genotoxicity in in vitro studies for point mutations or for chromosomal damage. In vivo studies for chromosome damage have yielded positive results in mice at oral doses of 1000 mg/kg and 2000 mg/kg. Exogenously administered progesterone has been shown to inhibit ovulation in a number of species and it is expected that high doses given for an extended duration would impair fertility until the cessation of treatment.
CLINICAL STUDIES
Effects on Vasomotor Symptoms in Postmenopausal Women
The effectiveness and safety of BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg and 1 mg/100 mg, on moderate to severe vasomotor symptoms (hot flushes) due to menopause were examined in a 12-week randomized, double-blind, placebo-controlled substudy of a single 52-week safety study. A total of 726 postmenopausal women were randomized to multiple dose combinations of estradiol and progesterone, and placebo; these women were 40 to 65 years of age (mean 54.6 years) and had at least 50 moderate to severe vasomotor symptoms per week at baseline. The mean number of years since last menstrual period was 5.9 years, with all women undergoing natural menopause. The primary efficacy population consisted of women who self- identified their race as: White (67%), Black/African American (31%), and "Other" (2.1%). In the substudy evaluating effects on moderate to severe vasomotor symptoms, a total of 149 women received BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg, 141 women received BIJUVA (estradiol and progesterone) capsules, 1 mg/100 mg, and 135 women received placebo.
The evaluated co-primary efficacy endpoints included: 1) mean weekly reduction in frequency of moderate to severe vasomotor symptoms with BIJUVA compared to placebo at Weeks 4 and 12 and 2) mean weekly reduction in severity of moderate to severe vasomotor symptoms with BIJUVA compared to placebo at Weeks 4 and 12.
Overall, BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg and 1 mg/100 mg, statistically significantly reduced both the frequency and severity of moderate to severe vasomotor symptoms from baseline compared with placebo at Weeks 4 and 12. The change from baseline in the frequency and severity of vasomotor symptoms observed and the difference from placebo are shown in Table 3 and Table 4, respectively.
| BIJUVA 0.5 mg/100 mg (N=149) | BIJUVA 1 mg/100 mg (N=141) | Placebo (N=135) | |
|---|---|---|---|
| Definitions: SD – standard deviation; SE – standard error | |||
| Week 4 | n=144 | n=134 | n=126 |
| Baseline | 72.3 (28.06) | 72.1 (27.80) | 72.3 (23.44) |
| Mean (SD) change from baseline | -35.1 (29.14) | -40.6 (30.59) | -26.4 (27.05) |
| Difference from placebo Least square mean difference (SE) from placebo | -8.07 (3.25) | -12.81 (3.30) | --- |
| P-value P-value of least square mean difference from placebo using mixed model repeated measures analyses | 0.013 | < 0.001 | --- |
| Week 12 | n=129 | n=124 | n=115 |
| Baseline | 72.8 (28.96) | 72.2 (25.04) | 72.2 (22.66) |
| Mean (SD) change from baseline | -53.7 (31.93) | -55.1 (31.36) | -40.2 (29.79) |
| Difference from placebo | -15.07 (3.39) | -16.58 (3.44) | --- |
| P-value | <0.001 | <0.001 | --- |
| BIJUVA 0.5 mg/100 mg (N=149) | BIJUVA 1 mg/100 mg (N=141) | Placebo (N=135) | |
|---|---|---|---|
| Definitions: SD – standard deviation; SE – standard error | |||
| Week 4 | n=144 | n=134 | n=126 |
| Baseline | 2.51 (0.248) | 2.54 (0.325) | 2.52 (0.249) |
| Mean (SD) change from baseline | -0.51 (0.563) | -0.48 (0.547) | -0.34 (0.386) |
| Difference from placebo Least square mean difference (SE) from placebo | -0.17 (0.060) | -0.13 (0.061) | --- |
| P-value P-value of least square mean difference from placebo using mixed model repeated measures analyses | 0.005 | 0.031 | --- |
| Week 12 | n=129 | n=124 | n=115 |
| Baseline | 2.51 (0.248) | 2.55 (0.235) | 2.52 (0.245) |
| Mean (SD) change from baseline | -0.90 (0.783) | -1.12 (0.963) | -0.56 (0.603) |
| Difference from placebo | -0.39 (0.099) | -0.57 (0.100) | --- |
| P-value | <0.001 | <0.001 | --- |
Adjusting for potential confounders such as BMI, smoking, alcohol use, and baseline estradiol level, treatment with BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg or 1 mg/100 mg, did not demonstrate statistically significant reductions in both frequency and severity of moderate to severe vasomotor symptoms by Week 12 in women who self-identified as Black/African Americans (data not shown).
Effects on Endometrium in Postmenopausal Women
Effects of BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg and 1 mg/100 mg, on endometrial hyperplasia and endometrial malignancy were assessed in the 52-week safety trial. The Endometrial Safety population included women who had taken at least one dose of BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg or 1 mg/100 mg, and had baseline and post-baseline endometrial biopsies. During the trial, endometrial biopsy assessments revealed one (1) case of endometrial hyperplasia and no cases of endometrial cancer in women who received BIJUVA (estradiol and progesterone) 0.5 mg/100 mg capsules, one (1) case of endometrial hyperplasia and no cases of endometrial cancer in women who received BIJUVA (estradiol and progesterone) 1 mg/100 mg capsules, and no cases of endometrial hyperplasia or endometrial cancer in women who received placebo (see Table 5 ).
| BIJUVA 0.5 mg/100 mg (N=303) | BIJUVA 1 mg/100 mg (N=281) | Placebo (N=92) | |
|---|---|---|---|
| Hyperplasia incidence rate % (n/N) | 1/303 (0.33) | 1/281 (0.36) | 0/92 (0.00) |
| One-sided upper 95% confidence limit | 1.83 | 1.97 | 3.93 |
Six (6) cases of disordered proliferative endometrium were reported for BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg, and four (4) cases of disordered proliferative endometrium were also reported for BIJUVA (estradiol and progesterone) capsules, 1 mg/100 mg, in the 52-week safety trial.
Effects on Uterine Bleeding or Spotting in Postmenopausal Women
Uterine bleeding or spotting was evaluated in the 52-week safety study by daily diary. At 52 weeks, cumulative amenorrhea was reported by 67.6% of women who received BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg, 56.1% of women who received BIJUVA (estradiol and progesterone) capsules, 1 mg/100 mg, and 78.9% who received placebo.
Women's Health Initiative Estrogen Plus Progestin Trial
The WHI estrogen plus progestin trial enrolled predominantly healthy postmenopausal women to assess the risks and benefits of daily oral CE (0.625 mg) in combination with MPA (2.5 mg) compared to placebo in the prevention of certain chronic diseases. The primary endpoint was the incidence of CHD (defined as nonfatal MI, silent MI and CHD death), with invasive breast cancer as the primary adverse outcome. A "global index" included the earliest occurrence of CHD, invasive breast cancer, stroke, PE, endometrial cancer, colorectal cancer, hip fracture, or death due to other causes. This trial did not evaluate the effects of CE plus MPA on menopausal symptoms.
The WHI estrogen plus progestin trial was stopped early. After an average follow-up of 5.6 years of treatment, the increased risk of invasive breast cancer crossed the predefined stopping threshold. The global index was supportive of a finding of overall harm. The absolute excess risk of events included in the global index was 19 per 10,000 women-years.
Results of the trial, which enrolled 16,608 women (average 63 years of age, range 50 to 79; 83.9% White, 6.8% Black, 5.4% Hispanic, 3.9% Other) are presented in Table 6. These results reflect centrally adjudicated data after an average follow-up of 5.6 years. 6,7
| Event | Relative Ratio (95% CI) In the WHI studies, hazard ratios were estimated using Cox proportional hazards models comparing treatment to placebo; however, they are described here as relative risks. Nominal confidence intervals unadjusted for multiple looks and multiple comparisons. | Risk Difference (CEMPA vs placebo/10,000 WYs) |
|---|---|---|
| CHD events | 1.18 (0.95-1.45) | 6 (41 vs 35) |
| Non-fatal MI | 1.24 (0.98-1.56) | 6 (35 vs 29) |
| CHD death | 1.05 (0.76-1.45) | 1 (16 vs 15) |
| All Strokes | 1.37 (1.07-1.76) | 9 (33 vs 24) |
| Deep vein thrombosis Not included in "global index." | 1.87 (1.37-2.54) | 12 (25 vs 14) |
| Pulmonary embolism | 1.98 (1.36-2.87) | 9 (18 vs 9) |
| Invasive breast cancer Includes metastatic and non-metastatic breast cancer with the exception of in situ cancer. | 1.24 (1.01-1.53) | 9 (43 vs 35) |
| Colorectal cancer | 0.62 (0.43-0.89) | -6 (10 vs 17) |
| Endometrial cancer | 0.83 (0.49-1.40) | -1 (6 vs 7) |
| Hip fracture | 0.67 (0.47-0.95) | -6 (11 vs 17) |
| Vertebral fracture | 0.68 (0.48-0.96) | -6 (12 vs 17) |
| Total factures | 0.76 (0.69-0.83) | -51 (161 vs 212) |
| Overall mortality , All deaths, except from breast or colorectal cancer, definite or probable CHD, PE or cerebrovascular disease. | 0.97 (0.81-1.16) | -1 (52 vs 53) |
| Global Index A subset of the events was combined in a "global index," defined as the earliest occurrence of CHD events, invasive breast cancer, stroke, PE, colorectal cancer, hip fracture, or death due to other causes. | 1.12 (1.02-1.24) | 20 (189 vs 168) |
Timing of the initiation of estrogen plus progestin therapy relative to the start of menopause may affect the overall risk benefit profile. The results of the WHI estrogen plus progestin trial in women 50-59 years of age (N=2,837 for CE/MPA; N=2,683 for placebo) are shown in Table 7.
| Event | Relative Ratio (95% CI) In the WHI studies, hazard ratios were estimated using Cox proportional hazards models comparing treatment to placebo; however, they are described here as relative risks. Nominal confidence intervals unadjusted for multiple looks and multiple comparisons. | Risk Difference (CEMPA vs placebo/10,000 WYs) |
|---|---|---|
| CHD events | 1.34 (0.82-2.19) | 5 (23 vs 17) |
| Non-fatal MI | 1.32 (0.77-2.25) | 4 (19 vs 15) |
| CHD death | 0.77 (0.33-1.79) | -2 (6 vs 8) |
| All Strokes | 1.51 (0.81-2.82) | 5 (15 vs 10) |
| Deep vein thrombosis Not included in "global index." | 3.01 (1.36-6.66) | 10 (15 vs 5) |
| Pulmonary embolism | 2.05 (0.89-4.71) | 6 (11 vs 5) |
| Invasive breast cancer Includes metastatic and non-metastatic breast cancer with the exception of in situ cancer. | 1.21 (0.81-1.80) | 6 (33 vs 27) |
| Colorectal cancer | 0.79 (0.29-2.18) | -1 (4 vs 5) |
| Endometrial cancer | 1.07 (0.33-3.53) | 0 (4 vs 3) |
| Hip fracture | 0.17 (0.22-1.45) | -3 (1 vs 3) |
| Vertebral fracture | 0.38 (0.15-0.97) | -6 (4 vs 10) |
| Total factures | 0.82 (0.68-1.00) | -25 (120 vs 145) |
| Overall mortality , All deaths, except from breast or colorectal cancer, definite or probable CHD, PE or cerebrovascular disease. | 0.67 (0.43-1.04) | -10 (21 vs 31) |
| Global Index A subset of the events was combined in a "global index," defined as the earliest occurrence of CHD events, invasive breast cancer, stroke, PE, colorectal cancer, hip fracture, or death due to other causes. | 1.12 (0.89-1.40) | 12 (103 vs 91) |
Women's Health Initiative Memory Study
The WHIMS estrogen plus progestin ancillary study of WHI enrolled 4,532 predominantly healthy postmenopausal women 65 years of age and older (47% were 65 to 69 years of age 35% were 70 to 74 years; 18% were 75 years of age and older) to evaluate effects of daily CE (0.625 mg) plus MPA (2.5 mg) on the incidence of probable dementia (primary outcome) compared to placebo. Probable dementia as defined in this study included Alzheimer's disease (AD), vascular dementia (VaD), and mixed types (having features of both AD and VaD). The most common classification of probable dementia in the treatment group and the placebo group was AD.
After an average follow-up of 4 years, the relative risk of probable dementia for CE/MPA versus placebo was 2.01 (95% CI, 1.19 to -3.42), with a risk difference of 23 per 10,000 WYs (46 versus 23). Since the ancillary study was conducted in women 65 to 79 years of age, it is unknown whether these findings apply to younger postmenopausal women [see Use in Specific Populations (8.5) ] . 8
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg, are oval-shaped opaque capsules, which are light pink on one side and dark pink on the other side. Each capsule is imprinted in white ink indicating the dosage strength (5C1). BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg, are provided in a blister package of 30 capsules.
BIJUVA (estradiol and progesterone) capsules, 1 mg/100 mg, are oval-shaped opaque capsules, which are light pink on one side and dark pink on the other side. Each capsule is imprinted in white ink indicating the dosage strength (1C1). BIJUVA (estradiol and progesterone) capsules, 1 mg/100 mg, are provided in a blister package of 30 capsules.
| BIJUVA (estradiol and progesterone) capsules, 0.5 mg/100 mg | NDC 50261-251-30 |
| BIJUVA (estradiol and progesterone) capsules, 1 mg/100 mg | NDC 50261-211-30 |
Keep out of reach of children. Packages are not child-resistant.
Storage and Handling
Store at 20°C to 25°C (68°F to 77°F), excursions permitted to 15°C to 30°C (59°F to 86°F). [See USP Controlled Room Temperature]
Mechanism of Action
Endogenous estrogens are largely responsible for the development and maintenance of the female reproductive system and secondary sexual characteristics. Although circulating estrogens exist in a dynamic equilibrium of metabolic interconversions, estradiol is the principal intracellular human estrogen and is substantially more potent than its metabolites, estrone and estriol, at the receptor level.
The primary source of estrogen in normally cycling adult women is the ovarian follicle, which secretes 70 to 500 mcg of estradiol daily, depending on the phase of the menstrual cycle. After menopause, most endogenous estrogen is produced by conversion of androstenedione, secreted by the adrenal cortex, to estrone in the peripheral tissues. Thus, estrone and the sulfate conjugated form, estrone sulfate, are the most abundant circulating estrogens in postmenopausal women.
Estrogens act through binding to nuclear receptors in estrogen-responsive tissues. To date, two estrogen receptors have been identified. These vary in proportion from tissue to tissue.
Circulating estrogens modulate the pituitary secretion of the gonadotropins, luteinizing hormone (LH), and FSH, through a negative feedback mechanism. Estrogens act to reduce the elevated levels of these hormones seen in postmenopausal women.
Endogenous progesterone is secreted by the ovary, placenta, and adrenal gland. In the presence of adequate estrogen, progesterone transforms a proliferative endometrium into a secretory endometrium.
Progesterone enhances cellular differentiation and generally opposes the actions of estrogens by decreasing estrogen receptor levels, increasing local metabolism of estrogens to less active metabolites, or inducing gene products that blunt cellular responses to estrogen. Progesterone exerts its effects in target cells by binding to specific progesterone receptors that interact with progesterone response elements in target genes. Progesterone receptors have been identified in the female reproductive tract, breast, pituitary, hypothalamus, and central nervous system.