Get your patient on Camila - Norethindrone tablet (Norethindrone)
Camila - Norethindrone tablet prescribing information
INDICATIONS AND USAGE
Indications
Progestin-only oral contraceptives are indicated for the prevention of pregnancy.
Efficacy
If used perfectly, the first-year failure rate for progestin-only oral contraceptives is 0.5%. However, the typical failure rate is estimated to be closer to 5%, due to late or omitted pills. The following table lists the pregnancy rates for users of all major methods of contraception.
| % of Women Experiencing an Unintended Pregnancy within the First Year of Use | % of Women Continuing Use at One Year | ||
|---|---|---|---|
| Method (1) | Typical Use Among typical couples who initiate use of a method (not necessarily for the first time), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any reason. (2) | Perfect Use Among couples who initiate use of a method (not necessarily for the first time), and who use it perfectly (both consistently and correctly), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any other reason. (3) | (4) |
| Emergency Contraceptive Pills: Treatment initiated within 72 hours after unprotected intercourse reduces the risk of pregnancy by at least 75%. The treatment schedule is one dose within 72 hours after unprotected intercourse, and a second dose 12 hours after the first dose. The Food and Drug Administration has declared the following brands of oral contraceptives to be safe and effective for emergency contraception: Ovral (1 dose is 2 white pills), Alesse (1 dose is 5 pink pills), Nordette or Levlen (1 dose is 4 yellow pills). | |||
| Lactational Amenorrhea Method: LAM is a highly effective, temporary method of contraception. However, to maintain effective protection against pregnancy, another method of contraception must be used as soon as menstruation resumes, the frequency or duration of breastfeeds is reduced, bottle feeds are introduced, or the baby reaches 6 months of age. | |||
| Source: Trussell, J, Contraceptive Efficacy. In: Hatcher RA, Trussell J, Stewart F, Cates W, Stewart GK, Kowal D, Guest F, Contraceptive Technology: Seventeenth Revised Edition. New York NY: Irvington Publishers, 1998. | |||
| 3 Among couples attempting to avoid pregnancy, the percentage who continue to use a method for one year. | |||
| Chance The percentage of women becoming pregnant noted in columns (2) and (3) are based on data from populations where contraception is not used and from women who cease using contraception in order to become pregnant. Among such populations, about 89% become pregnant within one year. This estimate was lowered slightly (to 85%) to represent the percentage that would become pregnant within one year among women now relying on reversible methods of contraception if they abandoned contraception altogether. | 85 | 85 | |
| Spermicides Foams, creams, gels, vaginal suppositories, and vaginal film. | 26 | 6 | 40 |
| Periodic Abstinence Calendar Ovulation Method Sympto-Thermal Cervical mucus (ovulation) method supplemented by calendar in the pre-ovulatory and basal body temperature in the post-ovulatory phases. Post-Ovulation | 25 | 9 3 2 1 | 63 |
| Cap With spermicidal cream or jelly. Parous Women | 40 | 26 | 42 |
| Nulliparous Women | 20 | 9 | 56 |
| Sponge | |||
| Parous Women | 40 | 20 | 42 |
| Nulliparous Women | 20 | 9 | 56 |
| Diaphragm | 20 | 6 | 56 |
| Withdrawal | 19 | 4 | |
| Condom Without spermicides. | |||
| Female (Reality) | 21 | 5 | 56 |
| Male | 14 | 3 | 61 |
| Pill | 5 | 71 | |
| Progestin-only | 0.5 | ||
| Combined | 0.1 | ||
| IUDs | |||
| Progesterone T | 2 | 1.5 | 81 |
| Copper T380A | 0.8 | 0.6 | 78 |
| LNg 20 | 0.1 | 0.1 | 81 |
| Depo-Provera | 0.3 | 0.3 | 70 |
| Levonorgestrel Implants (Norplant) | 0.05 | 0.05 | 88 |
| Female Sterilization | 0.5 | 0.5 | 100 |
| Male Sterilization | 0.15 | 0.10 | 100 |
DOSAGE AND ADMINISTRATION
To achieve maximum contraceptive effectiveness, Camila must be taken exactly as directed. One tablet is taken every day, at the same time. Administration is continuous, with no interruption between pill packs. See PATIENT LABELING for detailed instructions.
CONTRAINDICATIONS
Progestin-only oral contraceptives (POPs) should not be used by women who currently have the following conditions:
- Known or suspected pregnancy
- Known or suspected carcinoma of the breast
- Undiagnosed abnormal genital bleeding
- Hypersensitivity to any component of this product
- Benign or malignant liver tumors
- Acute liver disease
ADVERSE REACTIONS
- Menstrual irregularity is the most frequently reported side effect.
- Frequent and irregular bleeding are common, while long duration of bleeding episodes and amenorrhea are less likely.
- Headache, breast tenderness, nausea, and dizziness are increased among progestin-only oral contraceptive users in some studies.
- Androgenic side effects such as acne, hirsutism, and weight gain occur rarely.
To report SUSPECTED ADVERSE EVENTS, contact Dr. Reddy’s Laboratories Inc, at 1-888-375-3784 or FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch for voluntary reporting of adverse reactions.
Drug Interactions
Change in contraceptive effectiveness associated with coadministration of other products:
a. Anti-infective Agents and Anticonvulsants
Contraceptive effectiveness may be reduced when hormonal contraceptives are coadministered with antibiotics, anticonvulsants, and other drugs that increase the metabolism of contraceptive steroids. This could result in unintended pregnancy or breakthrough bleeding. Examples include rifampin, barbiturates, phenylbutazone, phenytoin, carbamazepine, felbamate, oxcarbazepine, topiramate, and griseofulvin.
b. Anti-HIV Protease Inhibitors
Several of the anti-HIV protease inhibitors have been studied with coadministration of oral contraceptives; significant changes (increase and decrease) in the plasma levels of the estrogen and progestin have been noted in some cases. The safety and efficacy of OC products may be affected with the coadministration of anti-HIV protease inhibitors. Health care providers should refer to the label of the individual anti-HIV protease inhibitors for further drug-drug interaction information.
c. Herbal Products
Herbal products containing St. John's Wort (hypericum perforatum) may induce hepatic enzymes (cytochrome P450) and p-glycoprotein transporter and may reduce the effectiveness of contraceptive steroids. This may also result in breakthrough bleeding.
DESCRIPTION
Each light pink Camila® tablet provides a continuous oral contraceptive regimen of 0.35 mg norethindrone, USP daily, and has the following inactive ingredients: corn starch, FD&C red no. 40 aluminum lake, lactose monohydrate, magnesium stearate, povidone and sodium starch glycolate. The chemical name for norethindrone is 17-Hydroxy-19-nor-17α-pregn-4-en-20-yn-3-one. The structural formula follows:
 |
Therapeutic class = oral contraceptive.
Meets USP Dissolution Test 2.
CLINICAL PHARMACOLOGY
Mode of Action
Camila progestin-only oral contraceptives prevent conception by suppressing ovulation in approximately half of users, thickening the cervical mucus to inhibit sperm penetration, lowering the mid-cycle LH and FSH peaks, slowing the movement of the ovum through the fallopian tubes, and altering the endometrium.
Pharmacokinetics
Absorption
Norethindrone is rapidly absorbed with maximum plasma concentrations occurring within 1 to 2 hours after Camila administration (see Table 1 ). Norethindrone appears to be completely absorbed following oral administration; however, it is subject to first pass metabolism resulting in an absolute bioavailability of approximately 65%.
Figure 1: Mean ± SD Norethindrone Plasma Concentrations Following Camila Administration.
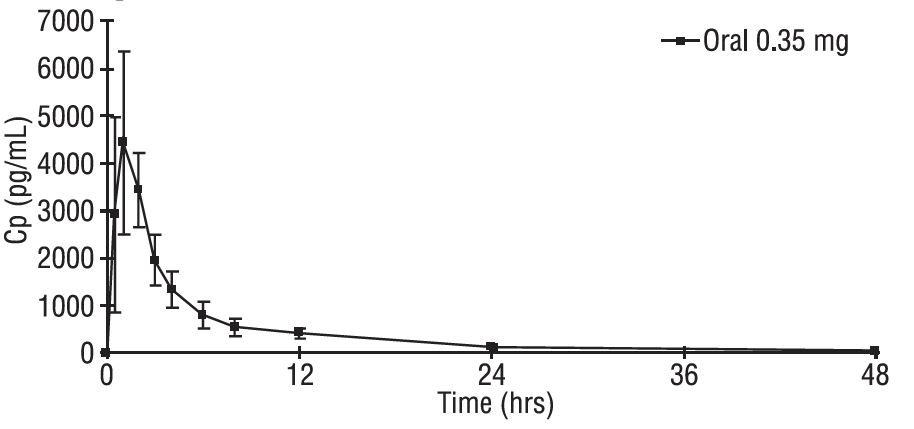
Peak plasma concentrations occur approximately 1 hour after administration (mean T max 1.2 hours). The mean (SD) C max was 4816.8 (1532.6) pg/mL and generally occurred within 1 hour (mean) of tablet administration, ranging from 0.5 to 2 hours. The mean (SD) C avg was 885 (250) pg/mL, however, the mean concentration at 24 hrs was 130 (47) pg/mL.
Table 1 provides summary statistics of the pharmacokinetic parameters associated with single dose Camila administration.
| Pharmacokinetic Parameter | Norethindrone 0.35 mg |
|---|---|
| T max (hr) | 1.2 ± 0.05 |
| C max (pg/mL) | 4817 ± 1533 |
| AUC (0-48) (pg∙h/mL) | 21233 ± 6002 |
| t 1/2 (h) | 7.7 ± 0.5 |
The food effect on the rate and extent of norethindrone absorption after Camila administration has not been evaluated.
Distribution
Following oral administration, norethindrone is 36% bound to sex hormone-binding globulin (SHBG) and 61% bound to albumin. Volume of distribution of norethindrone is approximately 4 L/kg.
Metabolism
Norethindrone undergoes extensive biotransformation, primarily via reduction, followed by sulfate and glucuronide conjugation; less than 5% of a norethindrone dose is excreted unchanged; greater than 50% and 20 to 40% of a dose is excreted in urine and feces, respectively. The majority of metabolites in the circulation are sulfate, with glucuronides accounting for most of the urinary metabolites.
Excretion
Plasma clearance rate for norethindrone has been estimated to be approximately 600 L/day. Norethindrone is excreted in both urine and feces, primarily as metabolites. The mean terminal elimination half-life of norethindrone following single dose administration of Camila is approximately 8 hours.
HOW SUPPLIED
Camila ® (norethindrone tablets USP, 0.35 mg) are packaged in cartons of 3 blister cards (NDC 75907-074-32) each containing 28 tablets. Each light pink, round, flat-faced, beveled-edge, unscored tablet is debossed with m on one side and 884 on the other side.
KEEP THIS AND ALL MEDICATIONS OUT OF THE REACH OF CHILDREN.
STORAGE
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
INSTRUCTIONS TO PATIENTS
How to Use the Camila Tablets Blister Card
1. The first time you use these pills, take your first pill on the first day of your menstrual period. Pick the Days of the Week Sticker that starts the first day of your period. When you have picked the right sticker, throw away the others and place the sticker on the blister card over the pre-printed days of the week and make sure it lines up with the pills.
2. Your blister package consists of three parts, the foil pouch, wallet, and a blister card containing 28 individually sealed pills. Note that the pills are arranged in four numbered rows of 7 pills, with the preprinted days of the week printed above them. All 28 pills are "active" birth control pills. Refer to the sample of the blister card below:
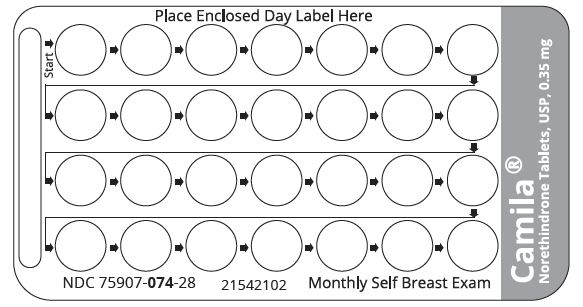
3. To remove a pill, push down on the pill with your thumb and forefinger so that the pill releases through the back of the blister card. Each day, take one pill. Always go from left to right along the row. Each new row will begin on the same day of the week.
4. Take one pill every day for 28 days, whether bleeding or not, until you have taken all the pills. It is important that you take your pill at the same time every day.
5. After you have taken all 28 pills, begin taking your pills again the next day. Be sure that the calendar day on your new package corresponds with the actual day.
All brand names listed are the registered trademarks of their respective owners and are not trademarks of Dr. Reddy’s Laboratories Inc.
Distributed by: Dr. Reddy’s Laboratories Inc. Princeton, NJ 08540
Manufactured by: Piramal Healthcare UK Limited Whalton Road Morpeth, NE61 3 YA
Rev. 11/2023 20769462
Mode of Action
Camila progestin-only oral contraceptives prevent conception by suppressing ovulation in approximately half of users, thickening the cervical mucus to inhibit sperm penetration, lowering the mid-cycle LH and FSH peaks, slowing the movement of the ovum through the fallopian tubes, and altering the endometrium.