Get your patient on Clonidine - Clonidine patch (Clonidine)
Clonidine - Clonidine patch prescribing information
INDICATIONS AND USAGE
Clonidine transdermal system is indicated in the treatment of hypertension. It may be employed alone or concomitantly with other antihypertensive agents.
DOSAGE AND ADMINISTRATION
Apply clonidine transdermal system once every 7 days to a hairless area of intact skin on the upper outer arm or chest. Each new application of clonidine transdermal system should be on a different skin site from the previous location. If the system loosens during 7-day wearing, the adhesive cover should be applied directly over the system to ensure good adhesion. There have been rare reports of the need for patch changes prior to 7 days to maintain blood pressure control.
To initiate therapy, clonidine transdermal system dosage should be titrated according to individual therapeutic requirements, starting with clonidine transdermal system 0.1 mg/day. If after one or two weeks the desired reduction in blood pressure is not achieved, increase the dosage by adding another clonidine transdermal system, 0.1 mg/day or changing to a larger system. An increase in dosage above two clonidine transdermal system 0.3 mg/day is usually not associated with additional efficacy.
When substituting clonidine transdermal system for oral clonidine or for other antihypertensive drugs, physicians should be aware that the antihypertensive effect of clonidine transdermal system may not commence until 2-3 days after initial application. Therefore, gradual reduction of prior drug dosage is advised. Some or all previous antihypertensive treatment may have to be continued, particularly in patients with more severe forms of hypertension.
Renal Impairment
Patients with renal impairment may benefit from a lower initial dose. Patients should be carefully monitored. Since only a minimal amount of clonidine is removed during routine hemodialysis, there is no need to give supplemental clonidine following dialysis.
CONTRAINDICATIONS
Clonidine transdermal system should not be used in patients with known hypersensitivity to clonidine or to any other component of the therapeutic system.
ADVERSE REACTIONS
Clinical Trial Experience with Clonidine Transdermal System
Most systemic adverse effects during clonidine transdermal system therapy have been mild and have tended to diminish with continued therapy. In a 3-month multi-clinic trial of clonidine transdermal system in 101 hypertensive patients, the systemic adverse reactions were, dry mouth (25 patients) and drowsiness (12), fatigue (6), headache (5), lethargy and sedation (3 each), insomnia, dizziness, impotence/sexual dysfunction, dry throat (2 each) and constipation, nausea, change in taste and nervousness (1 each).
In the above mentioned 3-month controlled clinical trial, as well as other uncontrolled clinical trials, the most frequent adverse reactions were dermatological and are described below.
In the 3-month trial, 51 of the 101 patients had localized skin reactions such as erythema (26 patients) and/or pruritus, particularly after using an adhesive cover throughout the 7-day dosage interval. Allergic contact sensitization to clonidine transdermal system was observed in 5 patients. Other skin reactions were localized vesiculation (7 patients), hyperpigmentation (5), edema (3), excoriation (3), burning (3), papules (1), throbbing (1), blanching (1), and a generalized macular rash (1).
In additional clinical experience, contact dermatitis resulting in treatment discontinuation was observed in 128 of 673 patients (about 19 in 100) after a mean duration of treatment of 37 weeks. The incidence of contact dermatitis was about 34 in 100 among white women, about 18 in 100 in white men, about 14 in 100 in black women, and approximately 8 in 100 in black men. Analysis of skin reaction data showed that the risk of having to discontinue clonidine transdermal system treatment because of contact dermatitis was greatest between treatment weeks 6 and 26, although sensitivity may develop either earlier or later in treatment.
In a large-scale clinical acceptability and safety study by 451 physicians in a total of 3539 patients, other allergic reactions were recorded for which a causal relationship to clonidine transdermal system was not established: maculopapular rash (10 cases); urticaria (2 cases); and angioedema of the face (2 cases), which also affected the tongue in one of the patients.
Marketing Experience with Clonidine Transdermal System
The following adverse reactions have been identified during post-approval use of clonidine transdermal system. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to estimate reliably their frequency or establish a causal relationship to drug exposure. Decisions to include these reactions in labeling are typically based on one or more of the following factors: (1) seriousness of the reaction, (2) frequency of reporting, or (3) strength of causal connection to clonidine transdermal system.
Body as a Whole: Fever; malaise; weakness; pallor; and withdrawal syndrome.
Cardiovascular: Congestive heart failure; cerebrovascular accident; electrocardiographic abnormalities (i.e., bradycardia, sick sinus syndrome disturbances and arrhythmias); chest pain; orthostatic symptoms; syncope; increases in blood pressure; sinus bradycardia and AV block with and without the use of concomitant digitalis; Raynaud’s phenomenon; tachycardia; bradycardia; and palpitations.
Central and Peripheral Nervous System/Psychiatric: Delirium; mental depression; hallucinations (including visual and auditory); localized numbness; vivid dreams or nightmares; restlessness; anxiety; agitation; irritability; other behavioral changes; and drowsiness.
Dermatological: Angioneurotic edema; localized or generalized rash; hives; urticaria; contact dermatitis; pruritus; alopecia; and localized hypo or hyper pigmentation.
Gastrointestinal: Anorexia and vomiting.
Genitourinary: Difficult micturition; loss of libido; and decreased sexual activity.
Metabolic: Gynecomastia or breast enlargement and weight gain.
Musculoskeletal: Muscle or joint pain; and leg cramps.
Ophthalmological: Blurred vision; burning of the eyes and dryness of the eyes.
Adverse Events Associated with Oral Clonidine Therapy
Most adverse effects are mild and tend to diminish with continued therapy. The most frequent (which appear to be dose-related) are dry mouth, occurring in about 40 of 100 patients; drowsiness, about 33 in 100; dizziness, about 16 in 100; constipation and sedation, each about 10 in 100. The following less frequent adverse experiences have also been reported in patients receiving clonidine hydrochloride tablets, but in many cases patients were receiving concomitant medication and a causal relationship has not been established.
Body as a Whole: Fatigue, fever, headache, pallor, weakness, and withdrawal syndrome. Also reported were a weakly positive Coombs’ test and increased sensitivity to alcohol.
Cardiovascular: Bradycardia, congestive heart failure, electrocardiographic abnormalities (i.e., sinus node arrest, junctional bradycardia, high degree AV block and arrhythmias), orthostatic symptoms, palpitations, Raynaud’s phenomenon, syncope, and tachycardia. Cases of sinus bradycardia and AV block have been reported, both with and without the use of concomitant digitalis.
Central Nervous System: Agitation, anxiety, delirium, delusional perception, hallucinations (including visual and auditory), insomnia, mental depression, nervousness, other behavioral changes, paresthesia, restlessness, sleep disorder, and vivid dreams or nightmares.
Dermatological: Alopecia, angioneurotic edema, hives, pruritus, rash, and urticaria.
Gastrointestinal: Abdominal pain, anorexia, constipation, hepatitis, malaise, mild transient abnormalities in liver function tests, nausea, parotitis, pseudo-obstruction (including colonic pseudo-obstruction), salivary gland pain, and vomiting.
Genitourinary: Decreased sexual activity, difficulty in micturition, erectile dysfunction, loss of libido, nocturia, and urinary retention.
Hematologic: Thrombocytopenia.
Metabolic: Gynecomastia, transient elevation of blood glucose or serum creatine phosphokinase, and weight gain.
Musculoskeletal: Leg cramps and muscle or joint pain.
Oro-otolaryngeal: Dryness of the nasal mucosa.
Ophthalmological: Accommodation disorder, blurred vision, burning of the eyes, decreased lacrimation, and dryness of the eyes.
DESCRIPTION
Clonidine transdermal system, USP is a transdermal system providing continuous systemic delivery of clonidine for 7 days at an approximately constant rate. Clonidine is a centrally acting alpha-agonist hypotensive agent. It is an imidazoline derivative with the chemical name 2-[(2,6-Dichlorophenyl)imino]imidazolidine and has the following chemical structure:
Meets USP Drug Release Test 3.
System Structure and Components
Clonidine transdermal system is a multi-layered film, 0.25 mm thick, containing clonidine as the active agent. The system areas are 3.33 cm 2 (0.1 mg/day), 6.67 cm 2 (0.2 mg/day), and 10.0 cm 2 (0.3 mg/day) and the amount of drug released is directly proportional to the area (see DESCRIPTION: Release Rate Concept ). The composition per unit area is the same for all three doses.
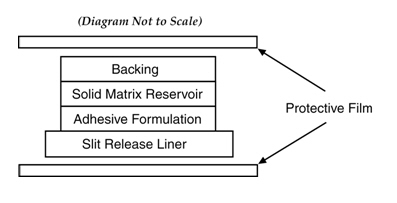
Proceeding from the visible surface towards the surface attached to the skin, there are three consecutive layers: 1) a backing layer of pigmented polyethylene and polyester film, 2) a solid matrix reservoir of clonidine, mineral oil, polyisobutylene, and colloidal silicon dioxide, 3) an adhesive formulation of clonidine, mineral oil, polyisobutylene, and colloidal silicon dioxide. Prior to use, a protective slit release liner of polyester that covers the adhesive formulation layer is removed.
Clonidine transdermal systems are packaged with additional pieces of protective film above and below the system within each pouch. These pieces of protective film are removed and discarded at the time of use.
Cross Section of the System:
Release Rate Concept
Clonidine transdermal system is programmed to release clonidine at an approximately constant rate for 7 days. The energy for drug release is derived from the concentration gradient existing between the patch and the much lower concentration prevailing in the skin. Clonidine flows in the direction of the lower concentration at a constant rate.
Following system application to intact skin, clonidine in the adhesive formulation layer saturates the skin site below the system. Clonidine from the patch then begins to flow into the systemic circulation via the capillaries beneath the skin. Therapeutic plasma clonidine levels are achieved 2 to 3 days after initial application of clonidine transdermal system.
The 3.33, 6.67, and 10.0 cm 2 systems deliver 0.1, 0.2, and 0.3 mg of clonidine per day, respectively. To ensure constant release of drug for 7 days, the total drug content of the system is higher than the total amount of drug delivered. Application of a new system to a fresh skin site at weekly intervals continuously maintains therapeutic plasma concentrations of clonidine. If the clonidine transdermal system is removed and not replaced with a new system, therapeutic plasma clonidine levels will persist for about 8 hours and then decline slowly over several days. Over this time period, blood pressure returns gradually to pretreatment levels.
CLINICAL PHARMACOLOGY
Clonidine stimulates alpha-adrenoreceptors in the brain stem. This action results in reduced sympathetic outflow from the central nervous system and in decreases in peripheral resistance, renal vascular resistance, heart rate, and blood pressure. Renal blood flow and glomerular filtration rate remain essentially unchanged. Normal postural reflexes are intact; therefore, orthostatic symptoms are mild and infrequent.
Acute studies with clonidine hydrochloride in humans have demonstrated a moderate reduction (15% to 20%) of cardiac output in the supine position with no change in the peripheral resistance; at a 45° tilt there is a smaller reduction in cardiac output and a decrease of peripheral resistance.
During long-term therapy, cardiac output tends to return to control values, while peripheral resistance remains decreased. Slowing of the pulse rate has been observed in most patients given clonidine, but the drug does not alter normal hemodynamic responses to exercise.
Tolerance to the antihypertensive effect may develop in some patients, necessitating a reevaluation of therapy.
Other studies in patients have provided evidence of a reduction in plasma renin activity and in the excretion of aldosterone and catecholamines. The exact relationship of these pharmacologic actions to the antihypertensive effect of clonidine has not been fully elucidated.
Clonidine acutely stimulates the release of growth hormone in children as well as adults but does not produce a chronic elevation of growth hormone with long-term use.
Pharmacokinetics
Clonidine transdermal system delivers clonidine at an approximately constant rate for 7 days. The absolute bioavailability of clonidine from the clonidine transdermal system dosage form is approximately 60%. Steady-state clonidine plasma levels are obtained within 3 days after transdermal application to the upper outer arm and increase linearly with increasing size of the transdermal patch. Mean steady-state plasma concentrations with the 3.33 cm 2 , 6.67 cm 2 , and 10.0 cm 2 systems are approximately 0.4 ng/mL, 0.8 ng/mL, and 1.1 ng/mL, respectively. Similar clonidine steady-state concentrations are reached after application to the chest. Steady-state clonidine plasma levels remain constant after removal of one system and application of a new system of the same size.
Following intravenous administration clonidine displays biphasic disposition with a distribution half-life of about 20 minutes and an elimination half-life ranging from 12 to 16 hours. The half-life increases up to 41 hours in patients with severe impairment of renal function. Clonidine has a total clearance of 177 mL/min and a renal clearance of 102 mL/min. The apparent volume of distribution (V z ) of clonidine is 197 L (2.9 L/kg). Clonidine crosses the placental barrier. It has been shown to cross the blood brain barrier in rats.
Following oral administration, about 40% to 60% of the absorbed dose is recovered in the urine as unchanged drug within 24 hours. About 50% of the absorbed dose is metabolized in the liver.
After removal of the clonidine transdermal system, clonidine plasma concentrations decline slowly with a half-life of approximately 20 hours.
HOW SUPPLIED
Clonidine Transdermal System, USP is available as 0.1 mg/day, 0.2 mg/day and 0.3 mg/day of clonidine, USP and are supplied as 4 pouched systems and 4 adhesive covers per carton. See chart below.
Programmed Delivery Clonidine in vivo Per Day Over 1 Week | Clonidine Content | Size | |
Clonidine Transdermal System, USP NDC 0378-0871-99 | 0.1 mg | 2.52 mg | 3.33 cm 2 |
Clonidine Transdermal System, USP NDC 0378-0872-99 | 0.2 mg | 5.04 mg | 6.67 cm 2 |
Clonidine Transdermal System, USP NDC 0378-0873-99 | 0.3 mg | 7.56 mg | 10.0 cm 2 |