Get your patient on Flutamide - Flutamide capsule (Flutamide)
Flutamide - Flutamide capsule prescribing information
BOXED WARNING
WARNINGS
Hepatic Injury
There have been postmarketing reports of hospitalization and rarely death due to liver failure in patients taking flutamide. Evidence of hepatic injury included elevated serum transaminase levels, jaundice, hepatic encephalopathy and death related to acute hepatic failure. The hepatic injury was reversible after discontinuation of therapy in some patients. Approximately half of the reported cases occurred within the initial 3 months of treatment with flutamide.
Serum transaminase levels should be measured prior to starting treatment with flutamide. Flutamide is not recommended in patients whose ALT values exceed twice the upper limit of normal. Serum transaminase levels should then be measured monthly for the first 4 months of therapy, and periodically thereafter. Liver function tests also should be obtained at the first signs and symptoms suggestive of liver dysfunction, e.g., nausea, vomiting, abdominal pain, fatigue, anorexia, "flu-like" symptoms, hyperbilirubinuria, jaundice or right upper quadrant tenderness. If at any time, a patient has jaundice, or their ALT rises above 2 times the upper limit of normal, flutamide should be immediately discontinued with close follow-up of liver function tests until resolution.
INDICATIONS AND USAGE
Flutamide capsules are indicated for use in combination with LHRH agonists for the management of locally confined Stage B 2 -C and Stage D 2 metastatic carcinoma of the prostate.
Stage B2-C Prostatic Carcinoma
Treatment with flutamide capsules and the goserelin acetate implant should start 8 weeks prior to initiating radiation therapy and continue during radiation therapy.
Stage D2 Metastatic Carcinoma
To achieve benefit from treatment, flutamide capsules should be initiated with the LHRH agonist and continued until progression.
DOSAGE AND ADMINISTRATION
The recommended dosage is 2 capsules 3 times a day at 8 hour intervals for a total daily dose of 750 mg.
CONTRAINDICATIONS
Flutamide capsules are contraindicated in patients who are hypersensitive to flutamide or any component of this preparation.
Flutamide capsules are contraindicated in patients with severe hepatic impairment (baseline hepatic enzymes should be evaluated prior to treatment).
ADVERSE REACTIONS
Stage B2-C Prostatic Carcinoma
Treatment with flutamide capsules and the goserelin acetate implant did not add substantially to the toxicity of radiation treatment alone. The following adverse experiences were reported during a multicenter clinical trial comparing flutamide capsules + goserelin acetate implant + radiation versus radiation alone. The most frequently reported (greater than 5%) adverse experiences are listed below.
| Adverse Events During Acute Radiation Therapy | ( within first 90 days of radiation therapy ) | Adverse Events During Late Radiation Phase | ( after 90 days of radiation therapy ) | ||
| ( n = 231 ) Goserelin Acetate Implant + Flutamide Capsules + Radiation % All | ( n = 235 ) Radiation Only % All | ( n = 231 ) Goserelin Acetate Implant + Flutamide Capsules + Radiation % All | ( n = 235 ) Radiation Only % All | ||
| Rectum/large bowel | 80 | 76 | Diarrhea | 36 | 40 |
| Bladder | 58 | 60 | Cystitis | 16 | 16 |
| Skin | 37 | 37 | Rectal bleeding | 14 | 20 |
| Proctitis | 8 | 8 | |||
| Hematuria | 7 | 12 |
Stage D2 Metastatic Carcinoma
The following adverse experiences were reported during a multicenter clinical trial comparing flutamide capsules + LHRH agonist versus placebo + LHRH agonist.
The most frequently reported (greater than 5%) adverse experiences during treatment with flutamide capsules in combination with an LHRH agonist are listed in the table below. For comparison, adverse experiences seen with an LHRH agonist and placebo are also listed in the following table.
| ( n = 294 ) Flutamide + LHRH agonist % All | ( n = 285 ) Placebo + LHRH agonist % All | |
| Hot flashes | 61 | 57 |
| Loss of libido | 36 | 31 |
| Impotence | 33 | 29 |
| Diarrhea | 12 | 4 |
| Nausea/vomiting | 11 | 10 |
| Gynecomastia | 9 | 11 |
| Other | 7 | 9 |
| Other GI | 6 | 4 |
Cardiovascular System
Hypertension in 1% of patients
Central Nervous System
CNS (drowsiness/confusion/depression/anxiety/nervousness) reactions occurred in 1% of patients
Gastrointestinal System
Anorexia 4%, and other GI disorders occurred in 6% of patients
Hematopoietic System
Anemia occurred in 6%, leukopenia in 3%, and thrombocytopenia in 1% of patients
Liver and Biliary System
Hepatitis and jaundice in less than 1% of patients
Skin
Irritation at the injection site and rash occurred in 3% of patients
Other
Edema occurred in 4%, genitourinary and neuromuscular symptoms in 2%, and pulmonary symptoms in less than 1% of patients.
In addition, the following spontaneous adverse experiences have been reported during the marketing of flutamide: hemolytic anemia, macrocytic anemia, methemoglobinemia, sulfhemoglobinemia, photosensitivity reactions (including erythema, ulceration, bullous eruptions, and epidermal necrolysis), and urine discoloration. The urine was noted to change to an amber or yellow-green appearance which can be attributed to the flutamide and/or its metabolites. Also reported were cholestatic jaundice, hepatic encephalopathy, and hepatic necrosis. The hepatic conditions were often reversible after discontinuing therapy; however, there have been reports of death following severe hepatic injury associated with use of flutamide.
Malignant breast neoplasms have occurred rarely in male patients being treated with flutamide.
Abnormal Laboratory Test Values
Laboratory abnormalities including elevated SGOT, SGPT, bilirubin values, SGGT, BUN, and serum creatinine have been reported.
Drug Interactions
Increases in prothrombin time have been noted in patients receiving long-term warfarin therapy after flutamide was initiated. Therefore close monitoring of prothrombin time is recommended and adjustment of the anticoagulant dose may be necessary when flutamide capsules are administered concomitantly with warfarin.
DESCRIPTION
Flutamide capsules, USP contain flutamide, an acetanilid, nonsteroidal, orally active antiandrogen having the chemical name, α,α,α-Trifluoro-2-methyl-4'-nitro- m -propionotoluidide and has the following structural formula:
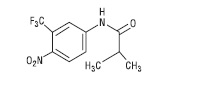
C 11 H 11 F 3 N 2 O 3 M.W. 276.21
Flutamide is a buff to yellow powder. Each capsule, for oral administration, contains 125 mg flutamide and has the following inactive ingredients: black iron oxide, corn starch, D&C yellow #10 aluminum lake, FD&C blue #1 aluminum lake, FD&C blue #2 aluminum lake, FD&C red #40 aluminum lake, gelatin, lactose monohydrate, magnesium stearate, red iron oxide, sodium lauryl sulfate, titanium dioxide and yellow iron oxide.
CLINICAL PHARMACOLOGY
General
In animal studies, flutamide demonstrates potent antiandrogenic effects. It exerts its antiandrogenic action by inhibiting androgen uptake and/or by inhibiting nuclear binding of androgen in target tissues or both. Prostatic carcinoma is known to be androgen-sensitive and responds to treatment that counteracts the effect of androgen and/or removes the source of androgen, e.g., castration. Elevations of plasma testosterone and estradiol levels have been noted following flutamide administration.
Pharmacokinetics
Absorption
Analysis of plasma, urine, and feces following a single oral 200 mg dose of tritium-labeled flutamide to human volunteers showed that the drug is rapidly and completely absorbed. Following a single 250 mg oral dose to normal adult volunteers, the biologically active alpha-hydroxylated metabolite reaches maximum plasma concentrations in about 2 hours, indicating that it is rapidly formed from flutamide. Food has no effect on bioavailability of flutamide.
Distribution
In male rats neither flutamide nor any of its metabolites is preferentially accumulated in any tissue except the prostate after an oral 5 mg/kg dose of 14 C-flutamide. Total drug levels were highest 6 hours after drug administration in all tissues. Levels declined at roughly similar rates to low levels at 18 hours. The major metabolite was present at higher concentrations than flutamide in all tissues studied. Following a single 250 mg oral dose to normal adult volunteers, low plasma levels of flutamide were detected. The plasma half-life for the alpha-hydroxylated metabolite of flutamide is about 6 hours. Flutamide, in vivo, at steady-state plasma concentrations of 24 to 78 ng/mL, is 94% to 96% bound to plasma proteins. The active metabolite of flutamide, in vivo, at steady-state plasma concentrations of 1556 to 2284 ng/mL, is 92% to 94% bound to plasma proteins.
Metabolism
The composition of plasma radioactivity, following a single 200 mg oral dose of tritium-labeled flutamide to normal adult volunteers, showed that flutamide is rapidly and extensively metabolized, with flutamide comprising only 2.5% of plasma radioactivity 1 hour after administration. At least 6 metabolites have been identified in plasma. The major plasma metabolite is a biologically active alpha-hydroxylated derivative which accounts for 23% of the plasma tritium 1 hour after drug administration. The major urinary metabolite is 2-amino-5-nitro-4-(trifluoromethyl)phenol.
Excretion
Flutamide and its metabolites are excreted mainly in the urine with only 4.2% of the dose excreted in the feces over 72 hours.
| Single Dose | Steady State | |||
| Flutamide | Hydroxyflutamide | Flutamide | Hydroxyflutamide | |
| C m a x (ng/mL) | 25.2 ± 34.2 | 894 ± 406 | 113 ± 213 | 1629 ± 586 |
| Elimination half-life (hr) | - | 8.1 ± 1.3 | 7.8 | 9.6 ± 2.5 |
| T m a x (hr) | 1.9 ± 0.7 | 2.7 ± 1 | 1.3 ± 0.7 | 1.9 ± 0.6 |
| C m i n (ng/mL) | - | - | - | 673 ± 316 |
Special Populations
Geriatric
Following multiple oral dosing of 250 mg t.i.d. in normal geriatric volunteers, flutamide and its active metabolite approached steady-state plasma levels (based on pharmacokinetic simulations) after the fourth flutamide dose. The half-life of the active metabolite in geriatric volunteers after a single flutamide dose is about 8.1 hours and at steady state in 9.6 hours.
Race
There are no known alterations in flutamide absorption, distribution, metabolism, or excretion due to race.
Renal Impairment
Following a single 250 mg dose of flutamide administered to subjects with chronic renal insufficiency, there appeared to be no correlation between creatinine clearance and either C max or AUC of flutamide. Renal impairment did not have an effect on the C max or AUC of the biologically active alpha-hydroxylated metabolite of flutamide. In subjects with creatinine clearance of < 29 mL/min, the half-life of the active metabolite was slightly prolonged. Flutamide and its active metabolite were not well dialyzed. Dose adjustment in patients with chronic renal insufficiency is not warranted.
Hepatic Impairment
No information on the pharmacokinetics of flutamide in hepatic impairment is available (see BOXED WARNINGS, Hepatic Injury ).
Women, Pediatrics
Flutamide has not been studied in women or pediatric patients.
Drug-Drug Interactions
Interactions between flutamide capsules and LHRH agonists have not occurred. Increases in prothrombin have been noted in patients receiving warfarin therapy (see PRECAUTIONS ).
Clinical Studies
Flutamide has been demonstrated to interfere with testosterone at the cellular level. This can complement medical castration achieved with LHRH agonists which suppresses testicular androgen production by inhibiting luteinizing hormone secretion.
The effects of combination therapy have been evaluated in two studies. One study evaluated the effects of flutamide and an LHRH agonist as neoadjuvant therapy to radiation in stage B 2 -C prostatic carcinoma and the other study evaluated flutamide and an LHRH agonist as the sole therapy in stage D 2 metastatic carcinoma.
Stage B2-C Prostatic Carcinoma
The effects of hormonal treatment combined with radiation were studied in 466 patients (231 flutamide capsules + goserelin acetate implant + radiation, 235 radiation alone) with bulky primary tumors confined to the prostate (stage B 2 ) or extending beyond the capsule (stage C), with or without pelvic node involvement.
In this multicentered, controlled trial, administration of flutamide capsules (250 mg t.i.d.) and goserelin acetate (3.6 mg depot) prior to and during radiation was associated with a significantly lower rate of local failure compared to radiation alone (16% vs. 33% at 4 years, P < 0.001). The combination therapy also resulted in a trend toward reduction in the incidence of distant metastases (27% vs. 36% at 4 years, P = 0.058). Median disease-free survival was significantly increased in patients who received complete hormonal therapy combined with radiation as compared to those patients who received radiation alone (4.4 vs. 2.6 years, P < 0.001). Inclusion of normal PSA level as a criterion for disease-free survival also resulted in significantly increased median disease-free survival in patients receiving the combination therapy (2.7 vs. 1.5 years, P < 0.001).
Stage D2 Prostatic Carcinoma
To study the effects of combination therapy in metastatic disease, 617 patients (311 leuprolide + flutamide, 306 leuprolide + placebo) with previously untreated advanced prostatic carcinoma were enrolled in a large multicentered, controlled clinical trial.
Three and one-half years after the study was initiated, median survival had been reached. The median actuarial survival time was 34.9 months for patients treated with leuprolide and flutamide versus 27.9 months for patients treated with leuprolide alone. This 7 month increment represents a 25% improvement in overall survival time with the flutamide therapy. Analysis of progression-free survival showed a 2.6 month improvement in patients who received leuprolide plus flutamide, a 19% increment over leuprolide and placebo.
Clinical Studies
Flutamide has been demonstrated to interfere with testosterone at the cellular level. This can complement medical castration achieved with LHRH agonists which suppresses testicular androgen production by inhibiting luteinizing hormone secretion.
The effects of combination therapy have been evaluated in two studies. One study evaluated the effects of flutamide and an LHRH agonist as neoadjuvant therapy to radiation in stage B 2 -C prostatic carcinoma and the other study evaluated flutamide and an LHRH agonist as the sole therapy in stage D 2 metastatic carcinoma.
Stage B2-C Prostatic Carcinoma
The effects of hormonal treatment combined with radiation were studied in 466 patients (231 flutamide capsules + goserelin acetate implant + radiation, 235 radiation alone) with bulky primary tumors confined to the prostate (stage B 2 ) or extending beyond the capsule (stage C), with or without pelvic node involvement.
In this multicentered, controlled trial, administration of flutamide capsules (250 mg t.i.d.) and goserelin acetate (3.6 mg depot) prior to and during radiation was associated with a significantly lower rate of local failure compared to radiation alone (16% vs. 33% at 4 years, P < 0.001). The combination therapy also resulted in a trend toward reduction in the incidence of distant metastases (27% vs. 36% at 4 years, P = 0.058). Median disease-free survival was significantly increased in patients who received complete hormonal therapy combined with radiation as compared to those patients who received radiation alone (4.4 vs. 2.6 years, P < 0.001). Inclusion of normal PSA level as a criterion for disease-free survival also resulted in significantly increased median disease-free survival in patients receiving the combination therapy (2.7 vs. 1.5 years, P < 0.001).
Stage D2 Prostatic Carcinoma
To study the effects of combination therapy in metastatic disease, 617 patients (311 leuprolide + flutamide, 306 leuprolide + placebo) with previously untreated advanced prostatic carcinoma were enrolled in a large multicentered, controlled clinical trial.
Three and one-half years after the study was initiated, median survival had been reached. The median actuarial survival time was 34.9 months for patients treated with leuprolide and flutamide versus 27.9 months for patients treated with leuprolide alone. This 7 month increment represents a 25% improvement in overall survival time with the flutamide therapy. Analysis of progression-free survival showed a 2.6 month improvement in patients who received leuprolide plus flutamide, a 19% increment over leuprolide and placebo.
HOW SUPPLIED
Flutamide capsules, USP, 125 mg are available as light brown opaque body and light brown opaque cap linear printed with 'Cipla' logo in black ink on cap and '915' along with '125 mg' in black ink on body. They are supplied as follows:
Bottle of 180 NDC 69097-915-91
Bottle of 500 NDC 69097-915-12
Dispense in a tight, light-resistant container as defined in the USP, with a child-resistant closure (as required).
KEEP THIS AND ALL MEDICATIONS OUT OF THE REACH OF CHILDREN.
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].
Manufactured by :
CIPLA Verna.
Goa, India
Manufactured for:
Cipla USA, Inc.
1560 Sawgrass Corporate Parkway.
Suite 130 Miami, FL 33323
Issued: 05/2017