Get your patient on Imipramine Pamoate - Imipramine Pamoate capsule (Imipramine Pamoate)
Imipramine Pamoate - Imipramine Pamoate capsule prescribing information
Suicidality and Antidepressant Drugs
Antidepressants increased the risk compared to placebo of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults in short-term studies of major depressive disorder (MDD) and other psychiatric disorders. Anyone considering the use of imipramine pamoate or any other antidepressant in a child, adolescent, or young adult must balance this risk with the clinical need. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction in risk with antidepressants compared to placebo in adults aged 65 and older. Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Patients of all ages who are started on antidepressant therapy should be monitored appropriately and observed closely for clinical worsening, suicidality, or unusual changes in behavior. Families and caregivers should be advised of the need for close observation and communication with the prescriber. Imipramine pamoate is not approved for use in pediatric patients (see WARNINGS: Clinical Worsening and Suicide Risk , PRECAUTIONS: Information for Patients , and PRECAUTIONS: Pediatric Use ).
INDICATIONS AND USAGE
For the relief of symptoms of depression. Endogenous depression is more likely to be alleviated than other depressive states. One to three weeks of treatment may be needed before optimal therapeutic effects are evident.
DOSAGE AND ADMINISTRATION
The following recommended dosages for imipramine pamoate capsules should be modified as necessary by the clinical response and any evidence of intolerance.
Initial Adult Dosage
Outpatients
Therapy should be initiated at 75 mg/day. Dosage may be increased to 150 mg/day which is the dose level at which optimum response is usually obtained. If necessary, dosage may be increased to 200 mg/day.
Dosage higher than 75 mg/day may also be administered on a once-a-day basis after the optimum dosage and tolerance have been determined. The daily dosage may be given at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
As with all tricyclics, the antidepressant effect of imipramine may not be evident for one to three weeks in some patients.
Hospitalized Patients
Therapy should be initiated at 100 to 150 mg/day and may be increased to 200 mg/day. If there is no response after two weeks, dosage should be increased to 250 to 300 mg/day.
Dosage higher than 150 mg/day may also be administered on a once-a-day basis after the optimum dosage and tolerance have been determined. The daily dosage may be given at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
As with all tricyclics, the antidepressant effect of imipramine may not be evident for one to three weeks in some patients.
Adult Maintenance Dosage
Following remission, maintenance medication may be required for a longer period of time at the lowest dose that will maintain remission after which the dosage should gradually be decreased.
The usual maintenance dosage is 75 to 150 mg/day. The total daily dosage can be administered on a once-a-day basis, preferably at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
In cases of relapse due to premature withdrawal of the drug, the effective dosage of imipramine should be reinstituted.
Adolescent and Geriatric Patients
Therapy in these age groups should be initiated with Tofranil™, brand of imipramine hydrochloride tablets, at a total daily dosage of 25 to 50 mg, since imipramine pamoate capsules are not available in these strengths. Dosage may be increased according to response and tolerance, but it is generally unnecessary to exceed 100 mg/day in these patients. Imipramine pamoate capsules may be used when total daily dosage is established at 75 mg or higher.
The total daily dosage can be administered on a once-a-day basis, preferably at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
As with all tricyclics, the antidepressant effect of imipramine may not be evident for one to three weeks in some patients.
Adolescent and geriatric patients can usually be maintained at lower dosage. Following remission, maintenance medication may be required for a longer period of time at the lowest dose that will maintain remission after which the dosage should gradually be decreased.
The total daily maintenance dosage can be administered on a once-a-day basis, preferably at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
In cases of relapse due to premature withdrawal of the drug, the effective dosage of imipramine should be reinstituted.
Switching a Patient to or from a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
At least 14 days should elapse between discontinuation of an MAOI intended to treat psychiatric disorders and initiation of therapy with imipramine pamoate. Conversely, at least 14 days should be allowed after stopping imipramine pamoate before starting an MAOI intended to treat psychiatric disorders (see CONTRAINDICATIONS ).
Use of Imipramine Pamoate with Other MAOIs, such as Linezolid or Methylene Blue
Do not start imipramine pamoate in a patient who is being treated with linezolid or intravenous methylene blue because there is increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, other interventions, including hospitalization, should be considered (see CONTRAINDICATIONS ).
In some cases, a patient already receiving imipramine pamoate therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, imipramine pamoate should be stopped promptly, and linezolid or intravenous methylene blue can be administered. The patient should be monitored for symptoms of serotonin syndrome for two weeks or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with imipramine pamoate may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue (see WARNINGS ).
The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with imipramine pamoate is unclear. The clinician should, nevertheless, be aware of the possibility of emergent symptoms of serotonin syndrome with such use (see WARNINGS ).
CONTRAINDICATIONS
Monoamine Oxidase Inhibitors (MAOIs)
The use of MAOIs intended to treat psychiatric disorders with imipramine pamoate or within 14 days of stopping treatment with imipramine pamoate is contraindicated because of an increased risk of serotonin syndrome. The use of imipramine pamoate within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated (see WARNINGS and DOSAGE AND ADMINISTRATION ).
Starting imipramine pamoate in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome (see WARNINGS and DOSAGE AND ADMINISTRATION ).
Myocardial Infarction
The drug is contraindicated during the acute recovery period after a myocardial infarction.
Hypersensitivity to Tricyclic Antidepressants
Patients with a known hypersensitivity to this compound should not be given the drug. The possibility of cross-sensitivity to other dibenzazepine compounds should be kept in mind.
ADVERSE REACTIONS
Note: Although the listing which follows includes a few adverse reactions which have not been reported with this specific drug, the pharmacological similarities among the tricyclic antidepressant drugs require that each of the reactions be considered when imipramine is administered.
Cardiovascular: Orthostatic hypotension, hypertension, tachycardia, palpitation, myocardial infarction, arrhythmias, heart block, ECG changes, precipitation of congestive heart failure, stroke.
Psychiatric
Confusional states (especially in the elderly) with hallucinations, disorientation, delusions; anxiety, restlessness, agitation; insomnia and nightmares; hypomania; exacerbation of psychosis.
Neurological
Numbness, tingling, paresthesias of extremities; incoordination, ataxia, tremors; peripheral neuropathy; extrapyramidal symptoms; seizures, alterations in EEG patterns; tinnitus.
Anticholinergic
Dry mouth, and, rarely, associated sublingual adenitis; blurred vision, disturbances of accommodation, mydriasis; constipation, paralytic ileus; urinary retention, delayed micturition, dilation of the urinary tract.
Allergic
Skin rash, petechiae, urticaria, itching, photosensitization; edema (general or of face and tongue); drug fever; cross-sensitivity with desipramine.
Hematologic
Bone marrow depression including agranulocytosis; eosinophilia; purpura; thrombocytopenia.
Gastrointestinal
Nausea and vomiting, anorexia, epigastric distress, diarrhea; peculiar taste, stomatitis, abdominal cramps, black tongue.
Endocrine
Gynecomastia in the male; breast enlargement and galactorrhea in the female; increased or decreased libido, impotence; testicular swelling; elevation or depression of blood sugar levels; inappropriate antidiuretic hormone (ADH) secretion syndrome.
Other
Jaundice (simulating obstructive); altered liver function; weight gain or loss; perspiration; flushing; urinary frequency; drowsiness, dizziness, weakness and fatigue; headache; parotid swelling; alopecia; proneness to falling; hyponatremia.
Withdrawal Symptoms
Though not indicative of addiction, abrupt cessation of treatment after prolonged therapy may produce nausea, headache and malaise.
Postmarketing Experience
The following adverse drug reaction has been reported during post-approval use of imipramine pamoate. Because this reaction is reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate frequency.
Eye disorders
Angle-closure glaucoma
Drug Interactions
Drugs Metabolized by P450 2D6 - The biochemical activity of the drug metabolizing isozyme cytochrome P450 2D6 (debrisoquin hydroxylase) is reduced in a subset of the Caucasian population (about 7% to 10% of Caucasians are so-called "poor metabolizers"); reliable estimates of the prevalence of reduced P450 2D6 isozyme activity among Asian, African, and other populations are not yet available. Poor metabolizers have higher than expected plasma concentrations of tricyclic antidepressants (TCAs) when given usual doses. Depending on the fraction of drug metabolized by P450 2D6, the increase in plasma concentration may be small, or quite large (8-fold increase in plasma AUC of the TCA).
In addition, certain drugs inhibit the activity of this isozyme and make normal metabolizers resemble poor metabolizers. An individual who is stable on a given dose of TCA may become abruptly toxic when given one of these inhibiting drugs as concomitant therapy. The drugs that inhibit cytochrome P450 2D6 include some that are not metabolized by the enzyme (quinidine; cimetidine) and many that are substrates for P450 2D6 (many other antidepressants, phenothiazines, and the Type 1C antiarrhythmics propafenone and flecainide). While all the selective serotonin reuptake inhibitors (SSRIs), e.g., fluoxetine, sertraline, and paroxetine, inhibit P450 2D6, they may vary in the extent of inhibition. The extent to which SSRI-TCA interactions may pose clinical problems will depend on the degree of inhibition and the pharmacokinetics of the SSRI involved. Nevertheless, caution is indicated in the co-administration of TCAs with any of the SSRIs and also in switching from one class to the other. Of particular importance, sufficient time must elapse before initiating TCA treatment in a patient being withdrawn from fluoxetine, given the long half-life of the parent and active metabolite (at least 5 weeks may be necessary).
Concomitant use of tricyclic antidepressants with drugs that can inhibit cytochrome P450 2D6 may require lower doses than usually prescribed for either the tricyclic antidepressant or the other drug. Furthermore, whenever one of these other drugs is withdrawn from co-therapy, an increased dose of tricyclic antidepressant may be required. It is desirable to monitor TCA plasma levels whenever a TCA is going to be co-administered with another drug known to be an inhibitor of P450 2D6.
The plasma concentration of imipramine may increase when the drug is given concomitantly with hepatic enzyme inhibitors (e.g., cimetidine, fluoxetine) and decrease by concomitant administration with hepatic enzyme inducers (e.g., barbiturates, phenytoin), and adjustment of the dosage of imipramine may therefore be necessary.
In occasional susceptible patients or in those receiving anticholinergic drugs (including antiparkinsonism agents) in addition, the atropine-like effects may become more pronounced (e.g., paralytic ileus). Close supervision and careful adjustment of dosage is required when imipramine pamoate is administered concomitantly with anticholinergic drugs.
Avoid the use of preparations, such as decongestants and local anesthetics, that contain any sympathomimetic amine (e.g., epinephrine, norepinephrine), since it has been reported that tricyclic antidepressants can potentiate the effects of catecholamines.
Caution should be exercised when imipramine pamoate is used with agents that lower blood pressure. Imipramine pamoate may potentiate the effects of CNS depressant drugs.
Patients should be warned that imipramine pamoate may enhance the CNS depressant effects of alcohol (see WARNINGS ) .
DESCRIPTION
Imipramine pamoate capsules USP are a tricyclic antidepressant, available as capsules for oral administration. The 75-, 100-, 125-, and 150-mg capsules contain imipramine pamoate equivalent to 75, 100, 125, and 150 mg of imipramine hydrochloride. Imipramine pamoate is 5-[3-(dimethylamino)propyl]-10,11-dihydro- 5H -dibenz[b,f]azepine 4, 4'-methylenebis-(3-hydroxy-2-naphthoate) (2:1), and its structural formula is
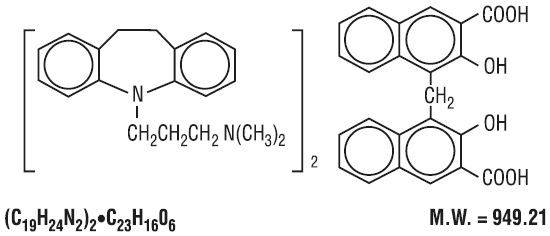
Imipramine pamoate is a fine, yellow, tasteless, odorless powder. It is soluble in ethanol, in acetone, in ether, in chloroform, and in carbon tetrachloride, and is insoluble in water.
Inactive Ingredients. corn starch, FD and C blue 1, FD and C red 40, FD and C yellow 6, D and C yellow 10 (in 100 mg and 125 mg capsules), gelatin, magnesium stearate, sodium lauryl sulphate, talc and titanium dioxide.
FDA approved dissolution specification differs from the USP dissolution specification.
CLINICAL PHARMACOLOGY
The mechanism of action of imipramine is not definitely known. However, it does not act primarily by stimulation of the central nervous system. The clinical effect is hypothesized as being due to potentiation of adrenergic synapses by blocking uptake of norepinephrine at nerve endings.
HOW SUPPLIED
Imipramine Pamoate Capsules USP 75 mg are size "2" capsule with brown cap and brown body, imprinted with "LU" in black ink on cap and "U01" in black ink on body, containing pale yellow to yellow granular powder.
They are supplied as follows:
NDC 68180-314-06 Bottles of 30's
Imipramine Pamoate Capsules USP 100 mg are size "1" capsule with brown cap and dark yellow body, imprinted with "LU" in black ink on cap and "U02" in black ink on body, containing pale yellow to yellow granular powder.
They are supplied as follows:
NDC 68180-315-06 Bottles of 30's
Imipramine Pamoate Capsules USP 125 mg are size "1" capsule with brown cap and light yellow body, imprinted with "LU" in black ink on cap and "U03" in black ink on body, containing pale yellow to yellow granular powder.
They are supplied as follows:
NDC 68180-316-06 Bottles of 30's
Imipramine Pamoate Capsules USP 150 mg are size "0" capsule with brown cap and brown body, imprinted with "LU" in black ink on cap and "U04" in black ink on body, containing pale yellow to yellow granular powder.
They are supplied as follows:
NDC 68180-317-06 Bottles of 30's
Store at 20°C to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Dispense in tight container (USP) with a child-resistant closure.