Get your patient on Lofena - Diclofenac Potassium tablet, Film Coated (Diclofenac Potassium)
Lofena - Diclofenac Potassium tablet, Film Coated prescribing information
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
Cardiovascular Thrombotic Events
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use (see WARNINGS ).
- LOFENA™ are contraindicated in the setting of coronary artery bypass graft (CABG) surgery (see CONTRAINDICATIONS , WARNINGS ).
Gastrointestinal Bleeding, Ulceration, and Perforation
- NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events (see WARNINGS ).
INDICATIONS AND USAGE
Carefully consider the potential benefits and risks of LOFENA ™ (diclofenac potassium tablets, USP) and other treatment options before deciding to use LOFENA. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals (see WARNINGS: Gastrointestinal Bleeding, Ulceration, and Perforation ).
LOFENA is indicated:
- For treatment of primary dysmenorrhea
- For relief of mild to moderate pain
- For relief of the signs and symptoms of osteoarthritis
- For relief of the signs and symptoms of rheumatoid arthritis
DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of LOFENA and other treatment options before deciding to use LOFENA . Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals (see WARNINGS: Gastrointestinal Bleeding, Ulceration, and Perforation ).
After observing the response to initial therapy with diclofenac potassium tablets, the dose and frequency should be adjusted to suit an individual patient's needs.
For treatment of pain or primary dysmenorrhea the recommended dosage is 50 mg three times a day. With experience, physicians may find that in some patients an initial dose of 100 mg of LOFENA , followed by 50 mg doses, will provide better relief.
For the relief of osteoarthritis, the recommended dosage is 100-150 mg/day in divided doses, 50 mg twice a day or three times a day.
For the relief of rheumatoid arthritis, the recommended dosage is 150-200 mg/day in divided doses, 50 mg three times a day or four times a day.
Different formulations of diclofenac (diclofenac sodium enteric-coated tablets; diclofenac sodium extended-release tablets; diclofenac potassium immediate-release tablets) are not necessarily bioequivalent even if the milligram strength is the same.
CONTRAINDICATIONS
LOFENA ™ is contraindicated in the following patients:
- Known hypersensitivity (e.g., anaphylactic reactions and serious skin reactions) to diclofenac or any components of the drug product (see WARNINGS: Anaphylactic Reactions , Serious Skin Reactions ).
- History of asthma, urticaria, or allergic type reactions after taking aspirin or other NSAIDs. Severe, sometimes fatal, anaphylactic reactions to NSAIDs have been reported in such patients (see WARNINGS: Anaphylactic Reactions , Exacerbation of Asthma Related to Aspirin Sensitivity ).
- In the setting of coronary artery bypass graft (CABG) surgery (see WARNINGS: Cardiovascular Thrombotic Events ) .
ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling:
- Cardiovascular Thrombotic Events (see WARNINGS )
- GI Bleeding, Ulceration and Perforation (see WARNINGS )
- Hepatotoxicity (see WARNINGS )
- Hypertension (see WARNINGS )
- Heart Failure and Edema (see WARNINGS )
- Renal Toxicity and Hyperkalemia (see WARNINGS )
- Anaphylactic Reactions (see WARNINGS )
- Serious Skin Reactions (see WARNINGS )
- Hematologic Toxicity (see WARNINGS )
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In 718 patients treated for shorter periods, i.e., 2 weeks or less, with LOFENA ™, adverse reactions were reported one-half to one-tenth as frequently as by patients treated for longer periods. In a 6-month, double-blind trial comparing LOFENA (N = 196) versus diclofenac sodium delayed-release tablets (N = 197) versus ibuprofen (N = 197), adverse reactions were similar in nature and frequency.
In patients taking LOFENA or other NSAIDs, the most frequently reported adverse experiences occurring in approximately 1%-10% of patients are:
Gastrointestinal experiences including abdominal pain, constipation, diarrhea, dyspepsia, flatulence, gross bleeding/perforation, heartburn, nausea, GI ulcers (gastric/duodenal) and vomiting.
Abnormal renal function, anemia, dizziness, edema, elevated liver enzymes, headaches, increased bleeding time, pruritus, rashes and tinnitus.
Additional adverse experiences reported occasionally include:
Body as a Whole:fever, infection, sepsis
Cardiovascular System:congestive heart failure, hypertension, tachycardia, syncope
Digestive System:dry mouth, esophagitis, gastric/peptic ulcers, gastritis, gastrointestinal bleeding, glossitis, hematemesis, hepatitis, jaundice
Hemic and Lymphatic System:ecchymosis, eosinophilia, leukopenia, melena, purpura, rectal bleeding, stomatitis, thrombocytopenia
Metabolic and Nutritional:weight changes
Nervous System:anxiety, asthenia, confusion, depression, dream abnormalities, drowsiness, insomnia, malaise, nervousness, paresthesia, somnolence, tremors, vertigo
Respiratory System:asthma, dyspnea
Skin and Appendages:alopecia, photosensitivity, sweating increased
Special Senses:blurred vision
Urogenital System:cystitis, dysuria, hematuria, interstitial nephritis, oliguria/polyuria, proteinuria, renal failure
Other adverse reactions, which occur rarely are:
Body as a Whole:anaphylactic reactions, appetite changes, death
Cardiovascular System:arrhythmia, hypotension, myocardial infarction, palpitations, vasculitis
Digestive System:colitis eructation, fulminant hepatitis with and without jaundice, liver failure, liver necrosis, pancreatitis
Hemic and Lymphatic System:agranulocytosis, hemolytic anemia, aplastic anemia, lymphadenopathy, pancytopenia
Metabolic and Nutritional:hyperglycemia
Nervous System:convulsions, coma, hallucinations, meningitis
Respiratory System:respiratory depression, pneumonia
Skin and Appendages:angioedema, toxic epidermal necrolysis, erythema multiforme, exfoliative dermatitis, Stevens Johnson Syndrome, urticaria
Special Senses:conjunctivitis, hearing impairment
To report SUSPECTED ADVERSE EVENTS , contact FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch for voluntary reporting of adverse reactions.
Drug Interactions
See Table 2 for clinically significant drug interactions with diclofenac.
| Drugs That Interfere with Hemostasis | |
| Clinical Impact: |
|
| Intervention: | Monitor patients with concomitant use of LOFENA with anticoagulants (e.g., warfarin), antiplatelet agents (e.g., aspirin), selective serotonin reuptake inhibitors (SSRIs), and serotonin norepinephrine reuptake inhibitors (SNRIs) for signs of bleeding (see WARNINGS: Hematological Toxicity ). |
| Aspirin | |
| Clinical Impact: | Controlled clinical studies showed that the concomitant use of NSAIDs and analgesic doses of aspirin does not produce any greater therapeutic effect than the use of NSAIDs alone. In a clinical study, the concomitant use of an NSAID and aspirin was associated with a significantly increased incidence of GI adverse reactions as compared to use of the NSAID alone (see WARNINGS: Gastrointestinal Bleeding, Ulceration, and Perforation ). |
| Intervention: | Concomitant use of LOFENA and analgesic doses of aspirin is not generally recommended because of the increased risk of bleeding (see WARNINGS: Hematological Toxicity ). LOFENA is not a substitute for low dose aspirin for cardiovascular protection. |
| ACE Inhibitors, Angiotensin Receptor Blockers, and Beta-Blockers | |
| Clinical Impact: |
|
| Intervention: |
|
| Diuretics | |
| Clinical Impact: | Clinical studies, as well as postmarketing observations, showed that NSAIDs reduced the natriuretic effect of loop diuretics (e.g., furosemide) and thiazide diuretics in some patients. This effect has been attributed to the NSAID inhibition of renal prostaglandin synthesis. |
| Intervention: | During concomitant use of LOFENA with diuretics, observe patients for signs of worsening renal function, in addition to assuring diuretic efficacy including antihypertensive effects (see WARNINGS: Renal Toxicity and Hyperkalemia ). |
| Digoxin | |
| Clinical Impact: | The concomitant use of diclofenac with digoxin has been reported to increase the serum concentration and prolong the half-life of digoxin. |
| Intervention: | During concomitant use of LOFENA and digoxin, monitor serum digoxin levels. |
| Lithium | |
| Clinical Impact: | NSAIDs have produced elevations in plasma lithium levels and reductions in renal lithium clearance . The mean minimum lithium concentration increased 15%, and the renal clearance decreased by approximately 20%. This effect has been attributed to NSAID inhibition of renal prostaglandin synthesis. |
| Intervention: | During concomitant use of LOFENA and lithium, monitor patients for signs of lithium toxicity. |
| Methotrexate | |
| Clinical Impact: | Concomitant use of NSAIDs and methotrexate may increase the risk for methotrexate toxicity (e.g., neutropenia, thrombocytopenia, renal dysfunction). |
| Intervention: | During concomitant use of LOFENA and methotrexate, monitor patients for methotrexate toxicity. |
| Cyclosporine | |
| Clinical Impact: | Concomitant use of diclofenac potassium tablets and cyclosporine may increase cyclosporine's nephrotoxicity. |
| Intervention: | During concomitant use of diclofenac potassium tablets and cyclosporine, monitor patients for signs of worsening renal function. |
| NSAIDs and Salicylates | |
| Clinical Impact: | Concomitant use of diclofenac with other NSAIDs or salicylates (e.g., diflunisal, salsalate) increases the risk of GI toxicity, with little or no increase in efficacy (see WARNINGS: Gastrointestinal Bleeding, Ulceration, and Perforation ). |
| Intervention: | The concomitant use of diclofenac with other NSAIDs or salicylates is not recommended. |
| Pemetrexed | |
| Clinical Impact: | Concomitant use of LOFENA and pemetrexed may increase the risk of pemetrexed associated myelosuppression, renal, and GI toxicity (see the pemetrexed prescribing information). |
| Intervention: | During concomitant use of LOFENA and pemetrexed, in patients with renal impairment whose creatinine clearance ranges from 45 mL/min to 79 mL/min, monitor for myelosuppression, renal and GI toxicity. NSAIDs with short elimination half-lives (e.g., diclofenac, indomethacin) should be avoided for a period of two days before, the day of, and two days following administration of pemetrexed. In the absence of data regarding potential interaction between pemetrexed and NSAIDs with longer half-lives (e.g., meloxicam, nabumetone), patients taking these NSAIDs should interrupt dosing for at least five days before, the day of, and two days following pemetrexed administration. |
| CYP2C9 Inhibitors or Inducers | |
| Clinical Impact: | Diclofenac is metabolized by cytochrome P450 enzymes, predominantly by CYP2C9. Co-administration of diclofenac with CYP2C9 inhibitors (e.g., voriconazole) may enhance the exposure and toxicity of diclofenac whereas co-administration with CYP2C9 inducers (e.g., rifampin) may lead to compromised efficacy of diclofenac. |
| Intervention: | A dosage adjustment may be warranted when diclofenac is administered with CYP2C9 inhibitors or inducers (see CLINICAL PHARMACOLOGY: Pharmacokinetics ). |
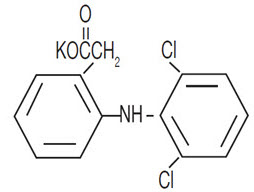
DESCRIPTION
LOFENA ™ (diclofenac potassium tablets, USP) are a benzeneacetic acid derivative. LOFENA , are available as tablets of 25 mg (white to off-white) for oral administration. The chemical name is 2-[(2,6-dichlorophenyl)amino] benzeneacetic acid, monopotassium salt. The molecular weight is 334.25. Its molecular formula is C 14 H 10 C l2 NKO 2 , and it has the following structural formula:
Each 25mg LOFENA intended for oral administration, contains 25 mg diclofenac potassium for oral administration. In addition, each tablet contains the following inactive ingredients: colloidal silicon dioxide, hydroxyethyl cellulose, iron oxide red, magnesium stearate, methanol, polyethylene glycol, povidone, sodium bicarbonate, titanium dioxide and yellow iron oxide.
CLINICAL PHARMACOLOGY
Mechanism of Action
Diclofenac has analgesic, anti-inflammatory, and antipyretic properties.
The mechanism of action of LOFENA, like that of other NSAIDs, is not completely understood but involves inhibition of cyclooxygenase (COX-1 and COX-2).
Diclofenac is a potent inhibitor of prostaglandin synthesis in vitro . Diclofenac concentrations reached during therapy have produced in vivo effects. Prostaglandins sensitize afferent nerves and potentiate the action of bradykinin in inducing pain in animal models. Prostaglandins are mediators of inflammation. Because diclofenac is an inhibitor of prostaglandin synthesis, its mode of action may be due to a decrease of prostaglandins in peripheral tissues.
Pharmacokinetics
Absorption
Diclofenac is 100% absorbed after oral administration compared to IV administration as measured by urine recovery. However, due to first pass metabolism, only about 50% of the absorbed dose is systemically available (see Table 1 ). In some fasting volunteers, measurable plasma levels are observed within 10 minutes of dosing with LOFENA . Peak plasma levels are achieved approximately 1 hour in fasting normal volunteers, with a range of .33 to 2 hours. Food has no significant effect on the extent of diclofenac absorption. However, there is usually a delay in the onset of absorption and a reduction in peak plasma levels of approximately 30%.
| PK Parameter | Normal Healthy Adults (20-52 years) | |
|---|---|---|
| Mean | Coefficient of Variation (%) | |
| Absolute Bioavailability (%) [N = 7] | 55 | 40 |
| T max (hr)[N = 65] | 1.0 | 76 |
| Oral Clearance (CL/F; mL/min) [N = 61] | 622 | 21 |
| Renal Clearance (% unchanged drug in urine) [N = 7] | < 1 | - |
| Apparent Volume of Distribution (V/F; L/kg) [N = 61] | 1.3 | 33 |
| Terminal Half-life (hr) [N = 48] | 1.9 | 29 |
Distribution
The apparent volume of distribution (V/F) of diclofenac potassium is 1.3 L/kg.
Diclofenac is more than 99% bound to human serum proteins, primarily to albumin. Serum protein binding is constant over the concentration range (0.15-105 mcg/mL) achieved with recommended doses.
Diclofenac diffuses into and out of the synovial fluid. Diffusion into the joint occurs when plasma levels are higher than those in the synovial fluid, after which the process reverses, and synovial fluid levels are higher than plasma levels. It is not known whether diffusion into the joint plays a role in the effectiveness of diclofenac.
Elimination
Metabolism
Five diclofenac metabolites have been identified in human plasma and urine. The metabolites include 4'-hydroxy, 5- hydroxy, 3'-hydroxy, 4', 5-dihydroxy and 3'-hydroxy 4'-methoxy-diclofenac. The major diclofenac metabolite, 4'-hydroxy-diclofenac, has very weak pharmacologic activity. The formation of 4'-hydroxy-diclofenac is primarily mediated by CYP2C9. Both diclofenac and its oxidative metabolites undergo glucuronidation or sulfation followed by biliary excretion. Acylglucuronidation mediated by UGT2B7 and oxidation mediated by CYP2C8 may also play a role in diclofenac metabolism. CYP3A4 is responsible for the formation of minor metabolites, 5- hydroxy-and 3'-hydroxy-diclofenac. In patients with renal dysfunction, peak concentrations of metabolites 4'- hydroxy- and 5-hydroxy-diclofenac were approximately 50% and 4% of the parent compound after single oral dosing compared to 27% and 1% in normal healthy subjects.
Excretion
Diclofenac is eliminated through metabolism and subsequent urinary and biliary excretion of the glucuronide and the sulfate conjugates of the metabolites. Little or no free unchanged diclofenac is excreted in the urine. Approximately 65% of the dose is excreted in the urine and approximately 35% in the bile as conjugates of unchanged diclofenac plus metabolites. Because renal elimination is not a significant pathway of elimination for unchanged diclofenac, dosing adjustment in patients with mild to moderate renal dysfunction is not necessary. The terminal half-life of unchanged diclofenac is approximately 2 hours.
Special Populations
Pediatric
The pharmacokinetics of LOFENA have not been investigated in pediatric patients.
Race
Pharmacokinetic differences due to race have not been identified.
Hepatic Impairment
Hepatic metabolism accounts for almost 100% of LOFENA elimination, so patients with hepatic disease may require reduced doses of LOFENA compared to patients with normal hepatic function.
Renal Impairment
Diclofenac pharmacokinetics has been investigated in subjects with renal insufficiency. No differences in the pharmacokinetics of diclofenac have been detected in studies of patients with renal impairment. In patients with renal impairment (inulin clearance 60-90, 30-60, and < 30 mL/min; N = 6 in each group), AUC values and elimination rate were comparable to those in healthy subjects.
Drug Interactions Studies
Voriconazole
When co administered with voriconazole (inhibitor of CYP2C9, 2C19 and 3A4 enzyme), the C max and AUC of diclofenac increased by 114% and 78%, respectively (see PRECAUTIONS: Drug Interactions ).
Aspirin
When NSAIDs were administered with aspirin, the protein binding of NSAIDs were reduced, although the clearance of free NSAID was not altered. The clinical significance of this interaction is not known. See Table 2 for clinically significant drug interactions of NSAIDs with aspirin (see PRECAUTIONS: Drug Interactions ).
HOW SUPPLIED
LOFENA ™ (diclofenac potassium tablets, USP) 25 mg are available for oral administration as white to off-white, round shaped, unscored, film coated tablets, imprinted "A" on one side and "25" on the other side. They are supplied as follows:
| NDC 15370-180-60 | Bottles of 60 |
| NDC 15370-180-10 | Bottles of 1000 |
Dispense in a tight, light-resistant container as defined in the USP using a child resistant closure.
Keep container tightly closed.
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
Protect from moisture.
Mechanism of Action
Diclofenac has analgesic, anti-inflammatory, and antipyretic properties.
The mechanism of action of LOFENA, like that of other NSAIDs, is not completely understood but involves inhibition of cyclooxygenase (COX-1 and COX-2).
Diclofenac is a potent inhibitor of prostaglandin synthesis in vitro . Diclofenac concentrations reached during therapy have produced in vivo effects. Prostaglandins sensitize afferent nerves and potentiate the action of bradykinin in inducing pain in animal models. Prostaglandins are mediators of inflammation. Because diclofenac is an inhibitor of prostaglandin synthesis, its mode of action may be due to a decrease of prostaglandins in peripheral tissues.