Get your patient on Moexipril Hydrochloride - Moexipril Hydrochloride tablet, Film Coated (Moexipril Hydrochloride)
Moexipril Hydrochloride - Moexipril Hydrochloride tablet, Film Coated prescribing information
WARNING: FETAL TOXICITY
- When pregnancy is detected, discontinue moexipril hydrochloride as soon as possible.
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. See WARNINGS: Fetal Toxicity .
INDICATIONS AND USAGE
Moexipril hydrochloride tablets are indicated for treatment of patients with hypertension. They may be used alone or in combination with thiazide diuretics.
In using moexipril hydrochloride tablets, consideration should be given to the fact that another ACE inhibitor, captopril, has caused agranulocytosis, particularly in patients with renal impairment or collagen-vascular disease. Available data are insufficient to show that moexipril hydrochloride tablets do not have a similar risk (see WARNINGS ).
In considering use of moexipril hydrochloride tablets, it should be noted that in controlled trials ACE inhibitors have an effect on blood pressure that is less in black patients than in non-blacks. In addition, ACE inhibitors (for which adequate data are available) cause a higher rate of angioedema in black than in non-black patients (see WARNINGS, Angioedema ).
DOSAGE AND ADMINISTRATION
Hypertension
The recommended initial dose of moexipril hydrochloride tablets in patients not receiving diuretics is 7.5 mg, one hour prior to meals, once daily. Dosage should be adjusted according to blood pressure response. The antihypertensive effect of moexipril hydrochloride tablets may diminish towards the end of the dosing interval. Blood pressure should, therefore, be measured just prior to dosing to determine whether satisfactory blood pressure control is obtained. If control is not adequate, increased dose or divided dosing can be tried. The recommended dose range is 7.5 to 30 mg daily, administered in one or two divided doses one hour before meals. Total daily doses above 60 mg a day have not been studied in hypertensive patients.
In patients who are currently being treated with a diuretic, symptomatic hypotension may occasionally occur following the initial dose of moexipril hydrochloride tablets. The diuretic should, if possible, be discontinued for 2 to 3 days before therapy with moexipril hydrochloride tablets is begun, to reduce the likelihood of hypotension (see WARNINGS ). If the patient’s blood pressure is not controlled with moexipril hydrochloride tablets alone, diuretic therapy may then be reinstituted. If diuretic therapy cannot be discontinued, an initial dose of 3.75 mg of moexipril hydrochloride tablets should be used with medical supervision until blood pressure has stabilized (see WARNINGS and PRECAUTIONS, Drug Interactions ).
Dosage Adjustment in Renal Impairment
For patients with a creatinine clearance ≤40 mL/min/1.73 m 2 , an initial dose of 3.75 mg once daily should be given cautiously. Doses may be titrated upward to a maximum daily dose of 15 mg.
CONTRAINDICATIONS
Moexipril hydrochloride is contraindicated in patients who are hypersensitive to this product and in patients with a history of angioedema related to previous treatment with an ACE inhibitor.
Do not co-administer aliskiren with moexipril hydrochloride in patients with diabetes (see PRECAUTIONS, Drug Interactions ).
ADVERSE REACTIONS
Moexipril hydrochloride has been evaluated for safety in more than 2500 patients with hypertension; more than 250 of these patients were treated for approximately one year. The overall incidence of reported adverse events was only slightly greater in patients treated with moexipril hydrochloride than patients treated with placebo.
Reported adverse experiences were usually mild and transient, and there were no differences in adverse reaction rates related to gender, race, age, duration of therapy, or total daily dosage within the range of 3.75 mg to 60 mg. Discontinuation of therapy because of adverse experiences was required in 3.4% of patients treated with moexipril hydrochloride and in 1.8% of patients treated with placebo. The most common reasons for discontinuation in patients treated with moexipril hydrochloride were cough (0.7%) and dizziness (0.4%).
All adverse experiences considered at least possibly related to treatment that occurred at any dose in placebo-controlled trials of once-daily dosing in more than 1% of patients treated with moexipril hydrochloride alone and that were at least as frequent in the moexipril hydrochloride group as in the placebo group are shown in the following table:
ADVERSE EVENT | MOEXIPRIL HYDROCHLORIDE (N=674) | PLACEBO (N=226) |
N (%) | N (%) | |
Cough Increased | 41 (6.1) | 5 (2.2) |
Dizziness | 29 (4.3) | 5 (2.2) |
Diarrhea | 21 (3.1) | 5 (2.2) |
Flu Syndrome | 21 (3.1) | 0 (0) |
Fatigue | 16 (2.4) | 4 (1.8) |
Pharyngitis | 12 (1.8) | 2 (0.9) |
Flushing | 11 (1.6) | 0 (0) |
Rash | 11 (1.6) | 2 (0.9) |
Myalgia | 9 (1.3) | 0 (0) |
Other adverse events occurring in more than 1% of patients on moexipril that were at least as frequent on placebo include: headache, upper respiratory infection, pain, rhinitis, dyspepsia, nausea, peripheral edema, sinusitis, chest pain, and urinary frequency. See WARNINGS and PRECAUTIONS for discussion of anaphylactoid reactions, angioedema, hypotension, neutropenia/agranulocytosis, second and third trimester fetal/neonatal morbidity and mortality, hyperkalemia, and cough.
Other potentially important adverse experiences reported in controlled or uncontrolled clinical trials in less than 1% of moexipril patients or that have been attributed to other ACE inhibitors include the following:
Cardiovascular:
Symptomatic hypotension, postural hypotension, or syncope were seen in 9/1750 (0.51%) patients; these reactions led to discontinuation of therapy in controlled trials in 3/1254 (0.24%) patients who had received moexipril hydrochloride monotherapy and in 1/344 (0.3%) patients who had received moexipril hydrochloride with hydrochlorothiazide (see PRECAUTIONS and WARNINGS ). Other adverse events included angina/myocardial infarction, palpitations, rhythm disturbances, and cerebrovascular accident.
Renal:
Of hypertensive patients with no apparent preexisting renal disease, 1% of patients receiving moexipril hydrochloride alone and 2% of patients receiving moexipril hydrochloride with hydrochlorothiazide experienced increases in serum creatinine to at least 140% of their baseline values (see PRECAUTIONS and DOSAGE AND ADMINISTRATION ).
Gastrointestinal:
Abdominal pain, constipation, vomiting, appetite/weight change, dry mouth, pancreatitis, hepatitis.
Respiratory:
Bronchospasm, dyspnea, eosinophilic pneumonitis.
Urogenital:
Renal insufficiency, oliguria.
Dermatologic:
Apparent hypersensitivity reactions manifested by urticaria, rash, pemphigus, pruritus, photosensitivity, alopecia.
Neurological and Psychiatric:
Drowsiness, sleep disturbances, nervousness, mood changes, anxiety.
Other:
Angioedema (see WARNINGS ), taste disturbances, tinnitus, sweating, malaise, arthralgia, hemolytic anemia.
Clinical Laboratory Test Findings
Serum Electrolytes:
Hyperkalemia (see PRECAUTIONS ), hyponatremia.
Creatinine and Blood Urea Nitrogen:
As with other ACE inhibitors, minor increases in blood urea nitrogen or serum creatinine, reversible upon discontinuation of therapy, were observed in approximately 1% of patients with essential hypertension who were treated with moexipril hydrochloride. Increases are more likely to occur in patients receiving concomitant diuretics and in patients with compromised renal function (see PRECAUTIONS, General ).
Other (causal relationship unknown):
Clinically important changes in standard laboratory tests were rarely associated with moexipril hydrochloride administration.
Elevations of liver enzymes and uric acid have been reported. In trials, less than 1% of moexipril-treated patients discontinued moexipril hydrochloride treatment because of laboratory abnormalities. The incidence of abnormal laboratory values with moexipril was similar to that in the placebo-treated group.
Drug Interactions
Diuretics:
Excessive reductions in blood pressure may occur in patients on diuretic therapy when ACE inhibitors are started. The possibility of hypotensive effects with moexipril hydrochloride can be minimized by discontinuing diuretic therapy for several days or cautiously increasing salt intake before initiation of treatment with moexipril hydrochloride. If this is not possible, the starting dose of moexipril should be reduced. (See WARNINGS and DOSAGE AND ADMINISTRATION ).
Potassium Supplements and Potassium-Sparing Diuretics:
Moexipril hydrochloride can increase serum potassium because it decreases aldosterone secretion. Use of potassium-sparing diuretics (spironolactone, triamterene, amiloride) or potassium supplements concomitantly with ACE inhibitors can increase the risk of hyperkalemia. Therefore, if concomitant use of such agents is indicated, they should be given with caution and the patient’s serum potassium should be monitored.
Oral Anticoagulants:
Interaction studies with warfarin failed to identify any clinically important effect on the serum concentrations of the anticoagulant or on its anticoagulant effect.
Lithium:
Increased serum lithium levels and symptoms of lithium toxicity have been reported in patients receiving ACE inhibitors during therapy with lithium. These drugs should be coadministered with caution, and frequent monitoring of serum lithium levels is recommended. If a diuretic is also used, the risk of lithium toxicity may be increased.
Gold :
Nitritoid reactions (symptoms include facial flushing, nausea, vomiting and hypotension) have been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and concomitant ACE inhibitor therapy including moexipril hydrochloride.
Non-Steroidal Anti-Inflammatory Agents including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors):
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, co-administration of NSAIDS, including selective COX-2 inhibitors, with ACE inhibitors, including moexipril, may result in deterioration of renal function, including possible acute renal failure. These effects are usually reversible. Monitor renal function periodically in patients receiving moexipril and NSAID therapy.
The antihypertensive effect of ACE inhibitors, including moexipril, may be attenuated by NSAIDS.
Dual Blockade of the Renin-Angiotensin System (RAS):
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Closely monitor blood pressure, renal function and electrolytes in patients on moexipril hydrochloride and other agents that affect the RAS.
Do not co-administer aliskiren with moexipril hydrochloride in patients with diabetes. Avoid use of aliskiren with moexipril hydrochloride in patients with renal impairment (GFR <60 mL/min).
Other Agents:
No clinically important pharmacokinetic interactions occurred when moexipril hydrochloride was administered concomitantly with hydrochlorothiazide, digoxin, or cimetidine.
Moexipril hydrochloride has been used in clinical trials concomitantly with calcium-channel-blocking agents, diuretics, H 2 blockers, digoxin, oral hypoglycemic agents, and cholesterol-lowering agents. There was no evidence of clinically important adverse interactions.
DESCRIPTION
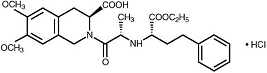
Moexipril hydrochloride USP, the hydrochloride salt of moexipril, has the empirical formula C 27 H 34 N 2 O 7 •HCl and a molecular weight of 535.04. It is chemically described as [3S-[2[R•(R•)],3R•]]-2-[2-[[1-(ethoxycarbonyl)-3-phenylpropyl]amino]-1-oxopropyl]- 1,2,3,4-tetrahydro-6,7-dimethoxy-3-iso-quinolinecarboxylic acid, monohydrochloride. It is a non-sulfhydryl containing precursor of the active angiotensin-converting enzyme (ACE) inhibitor moexiprilat and its structural formula is:
Moexipril hydrochloride USP is a fine white to off-white powder. It is soluble (about 10% weight-to-volume) in distilled water at room temperature.
Moexipril hydrochloride tablets USP are supplied as scored, coated tablets containing 7.5 mg and 15 mg of moexipril hydrochloride USP for oral administration. In addition to the active ingredient, moexipril hydrochloride USP, the tablet core contains the following inactive ingredients: crospovidone, lactose monohydrate, magnesium oxide, magnesium stearate and povidone. The film coating contains: hypromellose, hydroxypropyl cellulose, titanium dioxide, polyethylene glycol 6000, magnesium stearate, ferric oxide red, ferric oxide black and ferric oxide yellow (15 mg tablet only).
CLINICAL PHARMACOLOGY
Mechanism of Action
Moexipril hydrochloride is a prodrug for moexiprilat, which inhibits ACE in humans and animals. The mechanism through which moexiprilat lowers blood pressure is believed to be primarily inhibition of ACE activity. ACE is a peptidyl dipeptidase that catalyzes the conversion of the inactive decapeptide angiotensin I to the vasoconstrictor substance angiotensin II. Angiotensin II is a potent peripheral vasoconstrictor that also stimulates aldosterone secretion by the adrenal cortex and provides negative feedback on renin secretion. ACE is identical to kininase II, an enzyme that degrades bradykinin, an endothelium-dependent vasodilator. Moexiprilat is about 1000 times as potent as moexipril in inhibiting ACE and kininase II. Inhibition of ACE results in decreased angiotensin II formation, leading to decreased vasoconstriction, increased plasma renin activity, and decreased aldosterone secretion. The latter results in diuresis and natriuresis and a small increase in serum potassium concentration (mean increases of about 0.25 mEq/L were seen when moexipril was used alone, see PRECAUTIONS ).
Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of moexipril remains to be elucidated. Although the principal mechanism of moexipril in blood pressure reduction is believed to be through the renin-angiotensin-aldosterone system, ACE inhibitors have some effect on blood pressure even in apparent low-renin hypertension. As is the case with other ACE inhibitors, however, the antihypertensive effect of moexipril is considerably smaller in black patients, a predominantly low-renin population, than in non-black hypertensive patients.
Pharmacokinetics and Metabolism
Pharmacokinetics:
Moexipril’s antihypertensive activity is almost entirely due to its deesterified metabolite, moexiprilat. Bioavailability of oral moexipril is about 13% compared to intravenous (I.V.) moexipril (both measuring the metabolite moexiprilat), and is markedly affected by food, which reduces the peak plasma level (C max ) and AUC (see Absorption). Moexipril should therefore be taken in a fasting state. The time of peak plasma concentration (T max ) of moexiprilat is about 1 1/2 hours and elimination half-life (t 1/2 ) is estimated at 2 to 9 hours in various studies, the variability reflecting a complex elimination pattern that is not simply exponential. Like all ACE inhibitors, moexiprilat has a prolonged terminal elimination phase, presumably reflecting slow release of drug bound to the ACE. Accumulation of moexiprilat with repeated dosing is minimal, about 30%, compatible with a functional elimination t 1/2 of about 12 hours. Over the dose range of 7.5 to 30 mg, pharmacokinetics are approximately dose proportional.
Absorption:
Moexipril is incompletely absorbed, with bioavailability as moexiprilat of about 13%. Bioavailability varies with formulation and food intake which reduces C max and AUC by about 70% and 40% respectively after the ingestion of a low-fat breakfast or by 80% and 50% respectively after the ingestion of a high-fat breakfast.
Distribution:
The clearance (CL) for moexipril is 441 mL/min and for moexiprilat 232 mL/min with a t ½ of 1.3 and 9.8 hours, respectively. Moexiprilat is about 50% protein bound. The volume of distribution of moexiprilat is about 183 liters.
Metabolism and Excretion:
Moexipril is relatively rapidly converted to its active metabolite moexiprilat, but persists longer than some other ACE inhibitor prodrugs, such that its t ½ is over one hour and it has a significant AUC. Both moexipril and moexiprilat are converted to diketopiperazine derivatives and unidentified metabolites. After I.V. administration of moexipril, about 40% of the dose appears in urine as moexiprilat, about 26% as moexipril, with small amounts of the metabolites; about 20% of the I.V. dose appears in feces, principally as moexiprilat. After oral administration, only about 7% of the dose appears in urine as moexiprilat, about 1% as moexipril, with about 5% as other metabolites. Fifty-two percent of the dose is recovered in feces as moexiprilat and 1% as moexipril.
Special Populations:
Decreased Renal Function: The effective elimination t ½ and AUC of both moexipril and moexiprilat are increased with decreasing renal function. There is insufficient information available to characterize this relationship fully, but at creatinine clearances in the range of 10 to 40 mL/min, the t ½ of moexiprilat is increased by a factor of 3 to 4.
Decreased Hepatic Function: In patients with mild to moderate cirrhosis given single 15 mg doses of moexipril, the C max of moexipril was increased by about 50% and the AUC increased by about 120%, while the C max for moexiprilat was decreased by about 50% and the AUC increased by almost 300%.
Elderly Patients: In elderly male subjects (65 to 80 years old) with clinically normal renal and hepatic function, the AUC and C max of moexiprilat is about 30% greater than those of younger subjects (19 to 42 years old).
Pharmacokinetic Interactions With Other Drugs:
No clinically important pharmacokinetic interactions occurred when moexipril hydrochloride was administered concomitantly with hydrochlorothiazide, digoxin, or cimetidine.
Pharmacodynamics and Clinical Effect
Single and multiple doses of 15 mg or more of moexipril hydrochloride gives sustained inhibition of plasma ACE activity of 80 to 90%, beginning within 2 hours and lasting 24 hours (80%).
In controlled trials, the peak effects of orally administered moexipril increased with the dose administered over a dose range of 7.5 to 60 mg, given once a day. Antihypertensive effects were first detectable about 1 hour after dosing, with a peak effect between 3 and 6 hours after dosing. Just before dosing (i.e., at trough), the antihypertensive effects were less prominently related to dose and the antihypertensive effect tended to diminish during the 24-hour dosing interval when the drug was administered once a day.
In multiple dose studies in the dose range of 7.5 to 30 mg once daily, moexipril hydrochloride lowered sitting diastolic and systolic blood pressure effects at trough by 3 to 6 mmHg and 4 to 11 mmHg more than placebo, respectively. There was a tendency toward increased response with higher doses over this range. These effects are typical of ACE inhibitors but, to date, there are no trials of adequate size comparing moexipril with other antihypertensive agents.
The trough diastolic blood pressure effects of moexipril were approximately 3 to 6 mmHg in various studies. Generally, higher doses of moexipril leave a greater fraction of the peak blood pressure effect still present at trough. During dose titration, any decision as to the adequacy of a dosing regimen should be based on trough blood pressure measurements. If diastolic blood pressure control is not adequate at the end of the dosing interval, the dose can be increased or given as a divided (BID) regimen.
During chronic therapy, the antihypertensive effect of any dose of moexipril hydrochloride is generally evident within 2 weeks of treatment, with maximal reduction after 4 weeks. The antihypertensive effects of moexipril hydrochloride have been proven to continue during therapy for up to 24 months.
Moexipril hydrochloride, like other ACE inhibitors, is less effective in decreasing trough blood pressures in blacks than in non-blacks. Placebo-corrected trough group mean diastolic blood pressure effects in blacks in the proposed dose range varied between +1 to -3 mmHg compared with responses in non-blacks of -4 to -6 mmHg.
The effectiveness of moexipril hydrochloride was not significantly influenced by patient age, gender, or weight. Moexipril hydrochloride has been shown to have antihypertensive activity in both pre- and postmenopausal women who have participated in placebo-controlled clinical trials.
Formal interaction studies with moexipril have not been carried out with antihypertensive agents other than thiazide diuretics. In these studies, the added effect of moexipril was similar to its effect as monotherapy. In general, ACE inhibitors have less than additive effects with beta-adrenergic blockers, presumably because both work by inhibiting the renin-angiotensin system.
HOW SUPPLIED
Moexipril hydrochloride tablets USP 7.5 mg are peach, round, biconvex, film coated tablets with ‘G' and breakline engraved on one side and ‘209’ on the other side.
Bottles of 90 NDC 68462-209-90 Bottles of 100 NDC 68462-209-01 Bottles of 1,000 NDC 68462-209-10
Moexipril hydrochloride tablets USP 15 mg are brown, round, biconvex, film coated tablets with ‘G' and breakline engraved on one side and ‘208’ on the other side.
Bottles of 90 NDC 68462-208-90 Bottles of 100 NDC 68462-208-01 Bottles of 1,000 NDC 68462-208-10
Mechanism of Action
Moexipril hydrochloride is a prodrug for moexiprilat, which inhibits ACE in humans and animals. The mechanism through which moexiprilat lowers blood pressure is believed to be primarily inhibition of ACE activity. ACE is a peptidyl dipeptidase that catalyzes the conversion of the inactive decapeptide angiotensin I to the vasoconstrictor substance angiotensin II. Angiotensin II is a potent peripheral vasoconstrictor that also stimulates aldosterone secretion by the adrenal cortex and provides negative feedback on renin secretion. ACE is identical to kininase II, an enzyme that degrades bradykinin, an endothelium-dependent vasodilator. Moexiprilat is about 1000 times as potent as moexipril in inhibiting ACE and kininase II. Inhibition of ACE results in decreased angiotensin II formation, leading to decreased vasoconstriction, increased plasma renin activity, and decreased aldosterone secretion. The latter results in diuresis and natriuresis and a small increase in serum potassium concentration (mean increases of about 0.25 mEq/L were seen when moexipril was used alone, see PRECAUTIONS ).
Whether increased levels of bradykinin, a potent vasodepressor peptide, play a role in the therapeutic effects of moexipril remains to be elucidated. Although the principal mechanism of moexipril in blood pressure reduction is believed to be through the renin-angiotensin-aldosterone system, ACE inhibitors have some effect on blood pressure even in apparent low-renin hypertension. As is the case with other ACE inhibitors, however, the antihypertensive effect of moexipril is considerably smaller in black patients, a predominantly low-renin population, than in non-black hypertensive patients.