Get your patient on Provocholine - Methacholine Chloride powder, For Solution (Methacholine Chloride)
Provocholine - Methacholine Chloride powder, For Solution prescribing information
WARNING: SEVERE BRONCHOCONSTRICTION
WARNING: SEVERE BRONCHOCONSTRICTION
Severe bronchoconstriction can result from Provocholine administration (including the lowest dose). The use of Provocholine is contraindicated in pediatric and adult patients with baseline FEV1 < 60% predicted or adults with FEV1 < 1.5 L. Because of the potential for severe bronchoconstriction, the use of Provocholine in patients with clinically apparent asthma or wheezing is not recommended [ see Warnings and Precautions (5.1) ].
Emergency equipment and medication should be immediately available to treat acute respiratory distress. If severe bronchoconstriction occurs, reverse immediately with a rapid-acting inhaled bronchodilator agent (β-agonist) [ see Warnings and Precautions (5.1) ].
If baseline spirometry is not performed or is measured inaccurately, the initial FEV1 may be underestimated. In this situation, decreases in FEV1 may not be detected after administration of escalating Provocholine doses, which may result in administration of unnecessary higher doses and an increased risk for excessive bronchoconstriction [ see Warnings and Precautions (5.1) ].
1 INDICATIONS AND USAGE
Provocholine, used in a methacholine challenge test, is indicated for the diagnosis of bronchial airway hyperreactivity in adults and pediatric patients five years of age and older who do not have clinically apparent asthma.
2 DOSAGE AND ADMINISTRATION
Methacholine Challenge Test Overview
- Provocholine should be administered in a methacholine challenge test in a pulmonary function laboratory or clinic, by adequately trained personnel, for safety and accuracy, and should be performed only under the responsibility of a healthcare practitioner trained in and thoroughly familiar with all aspects of the technique of the test and the management of respiratory distress. Emergency medication and equipment should be immediately available to treat acute respiratory distress.
- Only consider Provocholine use in patients on chronic asthma drugs if the accuracy of the asthma diagnosis is in doubt. In these patients, only administer Provocholine if spirometry is normal after supervised withdrawal of the asthma drugs.
- Provocholine is not recommended for use in patients with clinically apparent asthma or wheezing.
- Before starting a methacholine challenge test, baseline spirometry must be performed. For a patient to be able to undergo the test, he or she must present with baseline FEV1 (Forced Expiratory Volume in 1 second) greater than or equal to 60% of the predicted value (in adults and children) and greater than or equal to 1.5 L (in adults).
- Do not use Provocholine in pediatric and adult patients with baseline FEV1 < 60% predicted or in adults with FEV1 < 1.5 L [ see Contraindications (4) and Warnings and Precautions (5.1) ].
- At commencement of the methacholine challenge test and prior to nebulization with Provocholine dose(s), FEV1 must be measured following exposure to nebulized diluent or base solution (contains no methacholine chloride) to obtain the post-diluent FEV1 [ see Dosage and Administration (2.4, 2.5) ].
- Provocholine powder for inhalation solution requires reconstitution and dilution before use ( see Reconstitution and Dilution Prior to Administration (2.3) ).
- Provocholine inhalation solution (in a ready-to-use kit) does not require reconstitution and/or dilution.
- Administer Provocholine by oral inhalation using either the 5-Breath Dosimeter Dosing Method or the 2-Minute Tidal Breathing Dosing Method with the doubling or quadrupling stepwise protocols [ see Dosage and Administration (2.4, 2.5) ].
- Discard any unused solution from the nebulizer after each administration.
- May use Provocholine with or without meals.
- The methacholine challenge test is considered positive if there is a reduction in FEV1 of 20% or more from post-diluent FEV1. The test should be stopped at this point. The reduction value must be calculated and recorded before starting the test with Provocholine ( see Calculation and Interpretation of Methacholine Challenge Test Results (2.6) ).
- An inhaled β agonist must be administered after a methacholine challenge test with Provocholine to expedite the return of the FEV1 to baseline and to relieve any discomfort of the subject. Most patients revert to normal pulmonary function within 10 to 20 minutes following administration of a β agonist.
3 DOSAGE FORMS AND STRENGTHS
• For inhalation solution: 100 mg of white to off-white crystalline powder in amber glass vials (powder is reconstituted and then diluted prior to administration)
• Inhalation solution: o base solution (contains no methacholine chloride/3 mL) o 0.0625 mg/mL (0.1875 mg/3 mL) o 0.25 mg/mL (0.75 mg/3 mL) o 1 mg/mL (3 mg/3 mL) o 4 mg/mL (12 mg/3 mL) o 16 mg/mL (48 mg/3 mL)
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary The available data from published literature on Provocholine use in pregnant women are insufficient to evaluate for a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Animal reproduction studies evaluating effects of methacholine chloride on embryofetal development have not been conducted. Diagnosis of bronchial airway hyperreactivity with bronchoprovocation challenge is not recommended for pregnant women because of the potential for hypoxia in the fetus. If bronchial airway hyperreactivity is suspected, consider trial of empiric treatment.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the United States general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
8.2 Lactation
Risk Summary There are no available data on the presence of methacholine chloride in human milk, the effect on the breastfed infant, or the effect on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Provocholine and any potential adverse effects on the breastfed infant from Provocholine or from the underlying maternal condition.
8.4 Pediatric Use
Provocholine is used in a methacholine challenge test for the diagnosis of bronchial airway hyperreactivity in pediatric patients 5 years of age and older who do not have clinically apparent asthma. The safety and effectiveness of Provocholine have not been established in pediatric patients below the age of 5 years.
8.5 Geriatric Use
The diagnosis of bronchial airway hyperreactivity is largely performed in pediatric and younger adult patients. Clinical studies of Provocholine did not include patients 65 years of age or older.
4 CONTRAINDICATIONS
Provocholine is contraindicated in the following:
- Hypersensitivity to methacholine or other parasympathomimetic agents. Reactions have included rash, itching/swelling (especially of the face/tongue/throat), severe dizziness, trouble breathing.
- Baseline FEV 1 < 60% predicted (adults or pediatric patients) or <1.5 L (adults)
5 WARNINGS AND PRECAUTIONS
5.1 Risk of Severe Bronchoconstriction
Severe bronchoconstriction can result from Provocholine administration (including the lowest dose). The use of Provocholine is contraindicated in pediatric and adult patients with baseline FEV 1 < 60% predicted or adults with FEV 1 < 1.5 L. Emergency equipment and medication should be immediately available to treat acute respiratory distress. Because of the potential for severe bronchoconstriction, the use of Provocholine in patients with clinically apparent asthma or wheezing is not recommended. If severe bronchoconstriction occurs, reverse immediately by the administration of a rapid-acting inhaled β-agonist.
If baseline spirometry is not performed or is measured inaccurately, the initial FEV 1 may be underestimated. In this situation, decreases in FEV 1 may not be detected after escalating Provocholine doses, which may result in administration of unnecessary higher doses and an increase in the risk for excessive bronchoconstriction.
5.2 Risks to Healthcare Providers Administering Provocholine
The supplied Provocholine powder or the Provocholine nebulized aerosol may cause bronchoconstriction in healthcare providers administering Provocholine in a methacholine challenge test. Healthcare providers and any other personnel involved in the administration of Provocholine should take the following precautionary steps:
- Do not inhale the supplied Provocholine powder
- Do not handle the Provocholine powder if you have asthma or hay fever.
- Apply a low resistance filter to expiratory ports of dosing apparatus, as necessary, to prevent Provocholine release in the room air
5.3 Coexisting Diseases and Conditions
Provocholine is not recommended for patients with uncontrolled hypertension, aortic aneurysm, or history of myocardial infarction or stroke diseases. Patients with epilepsy, vagotonia, peptic ulcer disease, thyroid disease, urinary tract obstruction or other condition that could be adversely affected by a cholinergic agent should undergo methacholine challenge only if the healthcare practitioner considers the benefit to the individual outweighs the potential risks.
6 ADVERSE REACTIONS
The following adverse reactions associated with the use of Provocholine were identified in clinical studies or post marketing reports. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Bronchospasm (includes symptoms such as chest tightness, cough or wheezing).
Adverse reactions less commonly associated with Provocholine include headache, throat irritation, light-headedness and itching.
7 DRUG INTERACTIONS
Beta-Adrenergic Blockers
The use of beta-adrenergic blockers may impair reversal of Provocholine-caused bronchoconstriction.
Beta-Agonists, Anticholinergics, and Theophylline Beta-agonists, anticholinergics, and theophylline inhibit the response of airways to Provocholine; therefore, hold these drugs before Provocholine use for the following duration:
• Short-acting β-agonists (e.g., albuterol): 6 hours • Long-acting β-agonists (e.g., salmeterol): 36 hours • Short-acting anti-cholinergics (e.g., ipratropium): 12 hours • Long-acting anti-cholinergics (e.g., tiotropium): ≥168 hours • Oral theophylline: 12-48 hours
Oral or Inhaled Corticosteroids, and Inhaled Cromoglycate
Regular use of oral or inhaled corticosteroids and inhaled cromoglycate may acutely decrease bronchial responsiveness to Provocholine. However, these drugs may be continued with Provocholine use.
11 DESCRIPTION
Methacholine chloride, the active ingredient of Provocholine, is a parasympathomimetic (cholinergic) bronchoconstrictor agent. Provocholine (methacholine chloride) powder for solution is administered by oral inhalation.
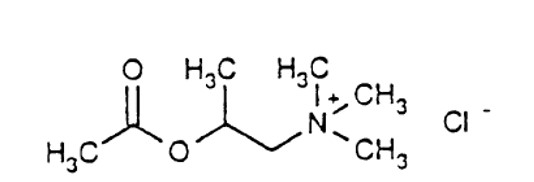
Chemically, methacholine chloride (the active ingredient) is 1-propanaminium, 2-(acetyloxy)-N,N,N,-trimethyl-, chloride. It is a white to practically white deliquescent compound, soluble in water, alcohol and chloroform and insoluble in ether. Aqueous solutions are neutral to litmus.
Methacholine chloride has an empirical formula of C 8 H 18 ClNO 2 , a molecular weight of 195.69, and the following structural formula:
Provocholine Powder for Solution: Each vial of Provocholine contains 100 mg of methacholine chloride powder.
Provocholine Solution for Inhalation Kit (Sterile): Each kit is packaged in a carton with six plastic vials with twist-off cap each containing 3 mL of the following concentrations of methacholine chloride solution. Each solution also contains: Sodium Acetate Trihydrate, Sodium Chloride, glacial acetic acid as pH adjuster.
a) base solution (contains no methacholine chloride) b) 0.0625 mg/mL (0.1875 mg/3 mL) c) 0.25 mg/mL (0.75 mg/3 mL) d) 1 mg/mL (3 mg/3 mL) e) 4 mg/mL (12 mg/3 mL) f) 16 mg/mL (48 mg/3 mL)
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Methacholine chloride is a cholinergic agonist. Bronchial smooth muscle contains significant parasympathetic (cholinergic) innervation. Methacholine chloride agonizes the muscarinic receptors which eventually induce bronchoconstriction.
12.2 Pharmacodynamics
After oral inhalation of Provocholine, patients with asthma are more sensitive to Provocholine-induced bronchoconstriction than are healthy subjects. This difference in response is the pharmacological basis for Provocholine in the methacholine challenge test.
12.3 Pharmacokinetics
There are no metabolic and pharmacokinetic data available on methacholine chloride.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
There have been no studies with methacholine chloride that would permit an evaluation of its carcinogenic or mutagenic potential or of its effect on fertility.
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
- Provocholine (methacholine chloride) Powder for Inhalation Solution: in amber glass vials that contain 100 mg of methacholine chloride powder, white to off-white in color. Cartons have 6 vials (NDC 64281-100-06).
- Provocholine (methacholine chloride) Inhalation Solution Kit (Sterile):
Each kit (NDC: 64281-110-05) contains six (6) plastic vials with twist-off cap each containing 3 mL of different concentrations of methacholine chloride as shown below. Cartons have six (6) kits (NDC 64281-110-06).
a) base solution (contains no methacholine chloride) (NDC: 64281-111-00) b) 0.0625 mg/mL (0.1875 mg/3 mL) (NDC:64281-112-00) c) 0.25 mg/mL (0.75 mg/3 mL) (NDC:64281-113-00) d) 1 mg/mL (3 mg/3 mL) (NDC:64281-114-00) e) 4 mg/mL (12 mg/3 mL) (NDC:64281-115-00) f) 16 mg/mL (48 mg/3 mL) (NDC:64281-116-00)
• Provocholine (methacholine chloride) Inhalation Solution 16 mg/mL (Sterile): in 3 mL plastic vial with twist-off cap. The solutions are packaged in inner cartons containing six (6) vials (NDC 64281-116-06). Two inner cartons are packaged in an outer carton (2x 6s cartons) (NDC 64281-110-12)
Storage and Handling
- Powder for inhalation solution: Store the supplied powder at 59 o F to 86 o F (15 o C to 30 o C). Refrigerate the reconstituted and diluted solutions at 36 o F to 46 o F (2 o C to 8 o C) for up to 2 weeks [see Dosage and Administration (2.3)].
- Provocholine inhalation solution kit: Store between 59 o F to 86 o F (15°C to 30°C). Use immediately upon opening the vial.
12.1 Mechanism of Action
Methacholine chloride is a cholinergic agonist. Bronchial smooth muscle contains significant parasympathetic (cholinergic) innervation. Methacholine chloride agonizes the muscarinic receptors which eventually induce bronchoconstriction.