Get your patient on Sulindac - Sulindac tablet (Sulindac)
Sulindac - Sulindac tablet prescribing information
Cardiovascular Thrombotic Events
- Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use [see Warnings and Precautions ].
- Sulindac tablets are contraindicated in the setting of coronary artery bypass graft (CABG) surgery [see Contraindications and Warnings].
Gastrointestinal Risk
- NSAIDs cause an increased risk of serious gastrointestinal adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients are at greater risk for serious gastrointestinal events. (see WARNINGS .)
INDICATIONS AND USAGE
Carefully consider the potential benefits and risks of sulindac tablets and other treatment options before deciding to use sulindac tablets. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals (see WARNINGS ).
Sulindac tablets are indicated for acute or long-term use in the relief of signs and symptoms of the following:
- Osteoarthritis
- Rheumatoid arthritis•
- Ankylosing spondylitis
- Acute painful shoulder (Acute subacromial bursitis/supraspinatus tendinitis)
- Acute gouty arthritis
DOSAGE AND ADMINISTRATION
Carefully consider the potential benefits and risks of sulindac tablets and other treatment options before deciding to use sulindac tablets. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals (see WARNINGS ).
After observing the response to initial therapy with sulindac tablets, the dose and frequency should be adjusted to suit an individual patient's needs.
Sulindac tablets should be administered orally twice a day with food. The maximum dosage is 400 mg per day. Dosages above 400 mg per day are not recommended.
In osteoarthritis, rheumatoid arthritis, and ankylosing spondylitis, the recommended starting dosage is 150 mg twice a day. The dosage may be lowered or raised depending on the response.
A prompt response (within one week) can be expected in about one-half of patients with osteoarthritis, ankylosing spondylitis, and rheumatoid arthritis. Others may require longer to respond.
In acute painful shoulder (acute subacromial bursitis/supraspinatus tendinitis) and acute gouty arthritis, the recommended dosage is 200 mg twice a day. After a satisfactory response has been achieved, the dosage may be reduced according to the response. In acute painful shoulder, therapy for 7–14 days is usually adequate. In acute gouty arthritis, therapy for 7 days is usually adequate.
••Incidence between 3% and 9%. Those reactions occurring in 1% to 3% of patients are not marked with an asterisk.
CONTRAINDICATIONS
Sulindac tablets are contraindicated in patients with known hypersensitivity to sulindac or the excipients (see DESCRIPTION ).
Sulindac tablets should not be given to patients who have experienced asthma, urticaria, or allergic-type reactions after taking aspirin or other NSAIDs. Severe, rarely fatal, anaphylactic/anaphylactoid reactions to NSAIDs have been reported in such patients (see WARNINGS – Anaphylactic/Anaphylactoid Reactions , and PRECAUTIONS – Preexisting Asthma ).
- In the setting of coronary artery bypass graft (CABG) surgery [see WARNINGS ].
ADVERSE REACTIONS
The following adverse reactions were reported in clinical trials or have been reported since the drug was marketed. The probability exists of a causal relationship between sulindac tablets and these adverse reactions. The adverse reactions which have been observed in clinical trials encompass observations in 1,865 patients, including 232 observed for at least 48 weeks.
Incidence Greater Than 1%
Gastrointestinal
The most frequent types of adverse reactions occurring with sulindac tablets are gastrointestinal; these include gastrointestinal pain (10%), dyspepsia••, nausea•• with or without vomiting, diarrhea••, constipation••, flatulence, anorexia and gastrointestinal cramps.
Dermatologic
Rash••, pruritus.
Central Nervous System
Dizziness••, headache••, nervousness.
Special Senses
Tinnitus.
Miscellaneous
Edema (see WARNINGS ).
Incidence Less Than 1 in 100
Gastrointestinal
Gastritis, gastroenteritis or colitis. Peptic ulcer and gastrointestinal bleeding have been reported. GI perforation and intestinal strictures (diaphragms) have been reported rarely.
Liver function abnormalities; jaundice, sometimes with fever; cholestasis; hepatitis; hepatic failure.
There have been rare reports of sulindac metabolites in common bile duct "sludge" and in biliary calculi in patients with symptoms of cholecystitis who underwent a cholecystectomy.
Pancreatitis (see PRECAUTIONS ).
Ageusia; glossitis.
Dermatologic
Stomatitis, sore or dry mucous membranes, alopecia, photosensitivity.
Erythema multiforme, toxic epidermal necrolysis, Stevens-Johnson syndrome, fixed drug eruption (FDE), and exfoliative dermatitis have been reported.
Cardiovascular
Congestive heart failure, especially in patients with marginal cardiac function; palpitation; hypertension.
Hematologic
Thrombocytopenia; ecchymosis; purpura; leukopenia; agranulocytosis; neutropenia; bone marrow depression, including aplastic anemia; hemolytic anemia; increased prothrombin time in patients on oral anticoagulants (see PRECAUTIONS ).
Genitourinary
Urine discoloration; dysuria; vaginal bleeding; hematuria; proteinuria; crystalluria; renal impairment, including renal failure; interstitial nephritis; nephrotic syndrome.
Renal calculi containing sulindac metabolites have been observed rarely.
Metabolic
Hyperkalemia.
Musculoskeletal
Muscle weakness.
Psychiatric
Depression; psychic disturbances including acute psychosis.
Nervous System
Vertigo; insomnia; somnolence; paresthesia; convulsions; syncope; aseptic meningitis (especially in patients with systemic lupus erythematosus (SLE) and mixed connective tissue disease, see PRECAUTIONS ).
Special Senses
Blurred vision; visual disturbances; decreased hearing; metallic or bitter taste.
Respiratory
Epistaxis.
Hypersensitivity Reactions
Anaphylaxis; angioneurotic edema; urticaria; bronchial spasm; dyspnea.
Hypersensitivity vasculitis.
A potentially fatal apparent hypersensitivity syndrome has been reported. This syndrome may include constitutional symptoms (fever, chills, diaphoresis, flushing), cutaneous findings (rash or other dermatologic reactions — see above), conjunctivitis, involvement of major organs (changes in liver function including hepatic failure, jaundice, pancreatitis, pneumonitis with or without pleural effusion, leukopenia, leukocytosis, eosinophilia, disseminated intravascular coagulation, anemia, renal impairment, including renal failure), and other less specific findings (adenitis, arthralgia, arthritis, myalgia, fatigue, malaise, hypotension, chest pain, tachycardia).
Causal Relationship Unknown
A rare occurrence of fulminant necrotizing fasciitis, particularly in association with Group A β-hemolytic streptococcus, has been described in persons treated with non-steroidal anti-inflammatory agents, sometimes with fatal outcome (see also PRECAUTIONS, General ).
Other reactions have been reported in clinical trials or since the drug was marketed, but occurred under circumstances where a causal relationship could not be established. However, in these rarely reported events, that possibility cannot be excluded. Therefore, these observations are listed to serve as alerting information to physicians.
Cardiovascular
Arrhythmia.
Metabolic
Hyperglycemia.
Nervous System
Neuritis.
Special Senses
Disturbances of the retina and its vasculature.
Miscellaneous
Gynecomastia.
Drug Interactions
ACE-Inhibitors and Angiotensin II Antagonists
Reports suggest that NSAIDs may diminish the antihypertensive effect of ACE-inhibitors and angiotensin II antagonists. These interactions should be given consideration in patients taking NSAIDs concomitantly with ACE-inhibitors or angiotensin II antagonists. In some patients with compromised renal function (e.g., elderly patients or patients who are volume-depleted, including those on diuretic therapy) who are being treated with non-steroidal anti-inflammatory drugs, the co-administration of an NSAID and an ACE-inhibitor or an angiotensin II antagonist may result in further deterioration of renal function, including possible acute renal failure, which is usually reversible. Therefore, monitor renal function periodically in patients receiving ACEIs or AIIAs and NSAIDs in combination therapy.
Acetaminophen
Acetaminophen had no effect on the plasma levels of sulindac or its sulfide metabolite.
Aspirin
The concomitant administration of aspirin with sulindac significantly depressed the plasma levels of the active sulfide metabolite. A double-blind study compared the safety and efficacy of sulindac tablets 300 or 400 mg daily given alone or with aspirin 2.4 g/day for the treatment of osteoarthritis. The addition of aspirin did not alter the types of clinical or laboratory adverse experiences for sulindac tablets; however, the combination showed an increase in the incidence of gastrointestinal adverse experiences. Since the addition of aspirin did not have a favorable effect on the therapeutic response to sulindac tablets, the combination is not recommended.
Cyclosporine
Administration of non-steroidal anti-inflammatory drugs concomitantly with cyclosporine has been associated with an increase in cyclosporine-induced toxicity, possibly due to decreased synthesis of renal prostacyclin. NSAIDs should be used with caution in patients taking cyclosporine, and renal function should be carefully monitored.
Diflunisal
The concomitant administration of sulindac tablets and diflunisal in normal volunteers resulted in lowering of the plasma levels of the active sulindac sulfide metabolite by approximately one-third.
Diuretics
Clinical studies, as well as post marketing observations, have shown that sulindac tablets can reduce the natriuretic effect of furosemide and thiazides in some patients. This response has been attributed to inhibition of renal prostaglandin synthesis. During concomitant therapy with NSAIDs, the patient should be observed closely for signs of renal failure (see WARNINGS, Renal Effects ) , as well as to assure diuretic efficacy.
DMSO
DMSO should not be used with sulindac. Concomitant administration has been reported to reduce the plasma levels of the active sulfide metabolite and potentially reduce efficacy. In addition, this combination has been reported to cause peripheral neuropathy.
Lithium
NSAIDs have produced an elevation of plasma lithium levels and a reduction in renal lithium clearance. The mean minimum lithium concentration increased 15% and the renal clearance was decreased by approximately 20%. These effects have been attributed to inhibition of renal prostaglandin synthesis by the NSAID. Thus, when NSAIDs and lithium are administered concurrently, subjects should be observed carefully for signs of lithium toxicity.
Methotrexate
NSAIDs have been reported to competitively inhibit methotrexate accumulation in rabbit kidney slices. This may indicate that they could enhance the toxicity of methotrexate. Caution should be used when NSAIDs are administered concomitantly with methotrexate.
NSAIDs
The concomitant use of sulindac tablets with other NSAIDs is not recommended due to the increased possibility of gastrointestinal toxicity, with little or no increase in efficacy.
Oral anticoagulants
Although sulindac and its sulfide metabolite are highly bound to protein, studies in which sulindac tablets were given at a dose of 400 mg daily have shown no clinically significant interaction with oral anticoagulants. However, patients should be monitored carefully until it is certain that no change in their anticoagulant dosage is required. Special attention should be paid to patients taking higher doses than those recommended and to patients with renal impairment or other metabolic defects that might increase sulindac blood levels. The effects of warfarin and NSAIDs on GI bleeding are synergistic, such that users of both drugs together have a risk of serious GI bleeding higher than users of either drug alone.
Oral hypoglycemic agents
Although sulindac and its sulfide metabolite are highly bound to protein, studies in which sulindac tablets were given at a dose of 400 mg daily, have shown no clinically significant interaction with oral hypoglycemic agents. However, patients should be monitored carefully until it is certain that no change in their hypoglycemic dosage is required. Special attention should be paid to patients taking higher doses than those recommended and to patients with renal impairment or other metabolic defects that might increase sulindac blood levels.
Probenecid
Probenecid given concomitantly with sulindac had only a slight effect on plasma sulfide levels, while plasma levels of sulindac and sulfone were increased. Sulindac was shown to produce a modest reduction in the uricosuric action of probenecid, which probably is not significant under most circumstances.
Propoxyphene hydrochloride
Propoxyphene hydrochloride had no effect on the plasma levels of sulindac or its sulfide metabolite.
DESCRIPTION
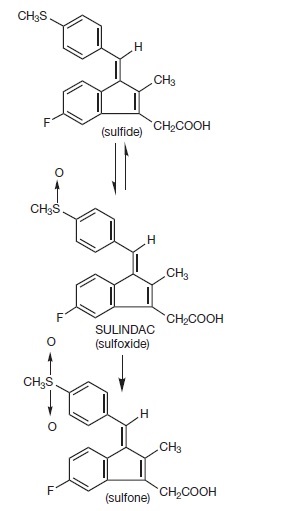
Sulindac is a non-steroidal, anti-inflammatory indene derivative designated chemically as (Z)-5-fluoro-2-methyl-1-[[ p -(methylsulfinyl)phenyl]methylene]-1 H -indene-3-acetic acid. It is not a salicylate, pyrazolone or propionic acid derivative. Its empirical formula is C 20 H 17 FO 3 S, with a molecular weight of 356.42. Sulindac, a yellow crystalline compound, is a weak organic acid practically insoluble in water below pH 4.5, but very soluble as the sodium salt or in buffers of pH 6 or higher.
Sulindac tablets are available in 150 and 200 mg tablets for oral administration. Each tablet contains the following inactive ingredients: magnesium stearate, microcrystalline cellulose, and pregelatinized starch.
Following absorption, sulindac undergoes two major biotransformations — reversible reduction to the sulfide metabolite, and irreversible oxidation to the sulfone metabolite. Available evidence indicates that the biological activity resides with the sulfide metabolite.
The structural formulas of sulindac and its metabolites are:
CLINICAL PHARMACOLOGY
Pharmacodynamics
Sulindac tablets are a non-steroidal anti-inflammatory drug (NSAID) that exhibits anti-inflammatory, analgesic and antipyretic activities in animal models. The mechanism of action, like that of other NSAIDs, is not completely understood but may be related to prostaglandin synthetase inhibition.
Pharmacokinetics
Absorption
The extent of sulindac absorption from sulindac tablets is similar as compared to sulindac solution.
There is no information regarding food effect on sulindac absorption. Antacids containing magnesium hydroxide 200 mg and aluminum hydroxide 225 mg per 5 mL have been shown not to significantly decrease the extent of sulindac absorption.
| PHARMACOKINETIC PARAMETERS | NORMAL | ELDERLY |
|---|---|---|
T max | Age 19–41 (n=24) | Age 65–87 (n=12) 400 mg qd |
(200 mg tablet) | 2.54 ± 1.52 S | |
5.75 ± 2.81 SF | ||
3.38 ± 2.30 S | 6.83 ± 4.19 SP | |
4.88 ± 2.57 SP | ||
4.96 ± 2.36 SF | ||
(150 mg tablet) | ||
3.90 ± 2.30 S | ||
5.85 ± 4.49 SP | ||
6.15 ± 3.07 SF | ||
Renal Clearance | (200 mg tablet) | |
68.12 ± 27.56 mL/min S | ||
36.58 ± 12.61 mL/min SP | ||
(150 mg tablet) | ||
74.39 ± 34.15 mL/min S | ||
41.75 ± 13.72 mL/min SP | ||
Mean effective Half life (h) | 7.8 S 16.4 SF | |
S = Sulindac SF = Sulindac Sulfide SP = Sulindac Sulfone |
Distribution
Sulindac, and its sulfone and sulfide metabolites, are 93.1, 95.4, and 97.9% bound to plasma proteins, predominantly to albumin. Plasma protein binding measured over a concentration range (0.5–2.0 µg/mL) was constant. Following an oral, radiolabeled dose of sulindac in rats, concentrations of radiolabel in red blood cells were about 10% of those in plasma. Sulindac penetrates the blood-brain and placental barriers. Concentrations in brain did not exceed 4% of those in plasma. Plasma concentrations in the placenta and in the fetus were less than 25% and 5% respectively, of systemic plasma concentrations. Sulindac is excreted in rat milk; concentrations in milk were 10 to 20% of those levels in plasma. It is not known if sulindac is excreted in human milk.
Metabolism
Sulindac undergoes two major biotransformations of its sulfoxide moiety: oxidation to the inactive sulfone and reduction to the pharmacologically active sulfide. The latter is readily reversible in animals and in man. These metabolites are present as unchanged compounds in plasma and principally as glucuronide conjugates in human urine and bile. A dihydroxydihydro analog has also been identified as a minor metabolite in human urine.
With the twice-a-day dosage regimen, plasma concentrations of sulindac and its two metabolites accumulate: mean concentration over a dosage interval at steady state relative to the first dose averages 1.5 and 2.5 times higher, respectively, for sulindac and its active sulfide metabolite.
Sulindac and its sulfone metabolite undergo extensive enterohepatic circulation relative to the sulfide metabolite in animals. Studies in man have also demonstrated that recirculation of the parent drug sulindac and its sulfone metabolite is more extensive than that of the active sulfide metabolite. The active sulfide metabolite accounts for less than six percent of the total intestinal exposure to sulindac and its metabolites.
Biochemical as well as pharmacological evidence indicates that the activity of sulindac resides in its sulfide metabolite. An in-vitro assay for inhibition of cyclooxygenase activity exhibited an EC 50 of 0.02 µM for sulindac sulfide. In-vivo models of inflammation indicate that activity is more highly correlated with concentrations of the metabolite than with parent drug concentrations.
Elimination
Approximately 50% of the administered dose of sulindac is excreted in the urine with the conjugated sulfone metabolite accounting for the major portion. Less than 1% of the administered dose of sulindac appears in the urine as the sulfide metabolite. Approximately 25% is found in the feces, primarily as the sulfone and sulfide metabolites.
The mean effective half-life (T 1/2 ) is 7.8 and 16.4 hours, respectively, for sulindac and its active sulfide metabolite.
Because sulindac tablets are excreted in the urine primarily as biologically inactive forms, it may possibly affect renal function to a lesser extent than other non-steroidal anti-inflammatory drugs; however, renal adverse experiences have been reported with sulindac tablets (see ADVERSE REACTIONS ).
In a study of patients with chronic glomerular disease treated with therapeutic doses of sulindac tablets, no effect was demonstrated on renal blood flow, glomerular filtration rate, or urinary excretion of prostaglandin E 2 and the primary metabolite of prostacyclin, 6-keto-PGF 1α . However, in other studies in healthy volunteers and patients with liver disease, sulindac tablets were found to blunt the renal responses to intravenous furosemide, i.e., the diuresis, natriuresis, increments in plasma renin activity and urinary excretion of prostaglandins. These observations may represent a differentiation of the effects of sulindac tablets on renal functions based on differences in pathogenesis of the renal prostaglandin dependence associated with differing dose-response relationships of different NSAIDs to the various renal functions influenced by prostaglandins (see PRECAUTIONS ).
In healthy men, the average fecal blood loss, measured over a two-week period during administration of 400 mg per day of sulindac tablets, was similar to that for placebo, and was statistically significantly less than that resulting from 4800 mg per day of aspirin.
Special Populations
Pediatric
The pharmacokinetics of sulindac have not been investigated in pediatric patients.
Race
Pharmacokinetic differences due to race have not been identified.
Hepatic Insufficiency
Patients with acute and chronic hepatic disease may require reduced doses of sulindac tablets compared to patients with normal hepatic function since hepatic metabolism is an important elimination pathway.
Following a single dose, plasma concentrations of the active sulfide metabolite have been reported to be higher in patients with alcoholic liver disease compared to healthy normal subjects.
Renal Insufficiency
Sulindac pharmacokinetics have been investigated in patients with renal insufficiency. The disposition of sulindac was studied in end-stage renal disease patients requiring hemodialysis. Plasma concentrations of sulindac and its sulfone metabolite were comparable to those of normal healthy volunteers whereas concentrations of the active sulfide metabolite were significantly reduced. Plasma protein binding was reduced and the AUC of the unbound sulfide metabolite was about half that in healthy subjects.
Sulindac and its metabolites are not significantly removed from the blood in patients undergoing hemodialysis.
Since sulindac tablets are eliminated primarily by the kidneys, patients with significantly impaired renal function should be closely monitored.
A lower daily dosage should be anticipated to avoid excessive drug accumulation.
In controlled clinical studies sulindac tablets were evaluated in the following five conditions:
1.000000000000000e+00 Osteoarthritis
In patients with osteoarthritis of the hip and knee, the anti-inflammatory and analgesic activity of sulindac tablets was demonstrated by clinical measurements that included: assessments by both patient and investigator of overall response; decrease in disease activity as assessed by both patient and investigator; improvement in ARA Functional Class; relief of night pain; improvement in overall evaluation of pain, including pain on weight bearing and pain on active and passive motion; improvement in joint mobility, range of motion, and functional activities; decreased swelling and tenderness; and decreased duration of stiffness following prolonged inactivity.
In clinical studies in which dosages were adjusted according to patient needs, sulindac tablets 200 to 400 mg daily were shown to be comparable in effectiveness to aspirin 2400 to 4800 mg daily. Sulindac tablets were generally well tolerated, and patients on it had a lower overall incidence of total adverse effects, of milder gastrointestinal reactions, and of tinnitus than did patients on aspirin. (See ADVERSE REACTIONS . )
2.000000000000000e+00 Rheumatoid arthritis
In patients with rheumatoid arthritis, the anti-inflammatory and analgesic activity of sulindac tablets was demonstrated by clinical measurements that included: assessments by both patient and investigator of overall response; decrease in disease activity as assessed by both patient and investigator; reduction in overall joint pain; reduction in duration and severity of morning stiffness; reduction in day and night pain; decrease in time required to walk 50 feet; decrease in general pain as measured on a visual analog scale; improvement in the Ritchie articular index; decrease in proximal interphalangeal joint size; improvement in ARA Functional Class; increase in grip strength; reduction in painful joint count and score; reduction in swollen joint count and score; and increased flexion and extension of the wrist.
In clinical studies in which dosages were adjusted according to patient needs, sulindac tablets 300 to 400 mg daily were shown to be comparable in effectiveness to aspirin 3600 to 4800 mg daily. Sulindac tablets were generally well tolerated, and patients on it had a lower overall incidence of total adverse effects, of milder gastrointestinal reactions, and of tinnitus than did patients on aspirin. (See ADVERSE REACTIONS . )
In patients with rheumatoid arthritis, sulindac tablets may be used in combination with gold salts at usual dosage levels. In clinical studies, sulindac tablets added to the regimen of gold salts usually resulted in additional symptomatic relief but did not alter the course of the underlying disease.
3.000000000000000e+00 Ankylosing spondylitis
In patients with ankylosing spondylitis, the anti-inflammatory and analgesic activity of sulindac tablets was demonstrated by clinical measurements that included: assessments by both patient and investigator of overall response; decrease in disease activity as assessed by both patient and investigator; improvement in ARA Functional Class; improvement in patient and investigator evaluation of spinal pain, tenderness and/or spasm; reduction in the duration of morning stiffness; increase in the time to onset of fatigue; relief of night pain; increase in chest expansion; and increase in spinal mobility evaluated by fingers-to-floor distance, occiput to wall distance, the Schober Test, and the Wright Modification of the Schober Test. In a clinical study in which dosages were adjusted according to patient need, sulindac tablets 200 to 400 mg daily were as effective as indomethacin 75 to 150 mg daily. In a second study, sulindac tablets 300 to 400 mg daily were comparable in effectiveness to phenylbutazone 400 to 600 mg daily. Sulindac tablets were better tolerated than phenylbutazone. (See ADVERSE REACTIONS . )
4.000000000000000e+00 Acute painful shoulder (Acute subacromial bursitis/supraspinatus tendinitis)
In patients with acute painful shoulder (acute subacromial bursitis/supraspinatus tendinitis), the anti-inflammatory and analgesic activity of sulindac tablets was demonstrated by clinical measurements that included: assessments by both patient and investigator of overall response; relief of night pain, spontaneous pain, and pain on active motion; decrease in local tenderness; and improvement in range of motion measured by abduction, and internal and external rotation. In clinical studies in acute painful shoulder, sulindac tablets 300 to 400 mg daily and oxyphenbutazone 400 to 600 mg daily were shown to be equally effective and well tolerated.
5 . Acute gouty arthritis
In patients with acute gouty arthritis, the anti-inflammatory and analgesic activity of sulindac tablets was demonstrated by clinical measurements that included: assessments by both the patient and investigator of overall response; relief of weight-bearing pain; relief of pain at rest and on active and passive motion; decrease in tenderness; reduction in warmth and swelling; increase in range of motion; and improvement in ability to function. In clinical studies, sulindac tablets at 400 mg daily and phenylbutazone at 600 mg daily were shown to be equally effective. In these short-term studies in which reduction of dosage was permitted according to response, both drugs were equally well tolerated.
HOW SUPPLIED
Sulindac tablets USP are supplied as follows:
Sulindac tablets, 150 mg, yellow, round, unscored, debossed MP 112
Bottles of 50 | NDC 53489-478-02 |
Bottles of 60 | NDC 53489-478-06 |
Bottles of 100 | NDC 53489-478-01 |
Bottles of 250 | NDC 53489-478-03 |
Bottles of 500 | NDC 53489-478-05 |
Bottles of 1000 | NDC 53489-478-10 |
Sulindac tablets, 200 mg, yellow, round, scored, debossed MP 116
Bottles of 50 | NDC 53489-479-02 |
Bottles of 60 | NDC 53489-479-06 |
Bottles of 100 | NDC 53489-479-01 |
Bottles of 250 | NDC 53489-479-03 |
Bottles of 500 | NDC 53489-479-05 |
Bottles of 1000 | NDC 53489-479-10 |
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature]
DISPENSE IN TIGHT, LIGHT-RESISTANT CONTAINER.