Get your patient on Vancomycin Hydrochloride - Vancomycin Hydrochloride injection, Powder, Lyophilized, For Solution (Vancomycin Hydrochloride)
Vancomycin Hydrochloride - Vancomycin Hydrochloride injection, Powder, Lyophilized, For Solution prescribing information
INDICATIONS AND USAGE:
To reduce the development of drug-resistant bacteria and maintain the effectiveness of Vancomycin Hydrochloride for Injection, USP and other antibacterial drugs, vancomycin should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
Vancomycin Hydrochloride for Injection, USP is indicated for the treatment of serious or severe infections caused by susceptible strains of methicillin-resistant (β-lactam-resistant) staphylococci. It is indicated for penicillin-allergic patients, for patients who cannot receive or who have failed to respond to other drugs, including the penicillins or cephalosporins, and for infections caused by vancomycin-susceptible organisms that are resistant to other antimicrobial drugs. Vancomycin is indicated for initial therapy when methicillin-resistant staphylococci are suspected, but after susceptibility data are available, therapy should be adjusted accordingly.
Vancomycin is effective in the treatment of staphylococcal endocarditis. Its effectiveness has been documented in other infections due to staphylococci, including septicemia, bone infections, lower respiratory tract infections, and skin and skin-structure infections. When staphylococcal infections are localized and purulent, antibiotics are used as adjuncts to appropriate surgical measures.
Vancomycin has been reported to be effective alone or in combination with an aminoglycoside for endocarditis caused by S. viridans or S. bovis. For endocarditis caused by enterococci (e.g., E. faecalis ) , vancomycin has been reported to be effective only in combination with an aminoglycoside.
Vancomycin has been reported to be effective for the treatment of diphtheroid endocarditis. Vancomycin has been used successfully in combination with either rifampin, an aminoglycoside, or both in early-onset prosthetic valve endocarditis caused by S. epidermidis or diphtheroids.
Specimens for bacteriologic cultures should be obtained in order to isolate and identify causative organisms and to determine their susceptibilities to vancomycin.
The parenteral form of vancomycin may be administered orally for treatment of antibiotic-associated pseudomembranous colitis produced by C. difficile and for staphylococcal enterocolitis. Parenteral administration of vancomycin hydrochloride alone is of unproven benefit for these indications. Vancomycin is not effective by the oral route for other types of infection.
DOSAGE AND ADMINISTRATION:
Infusion-related events are related to both the concentration and the rate of administration of vancomycin. Concentrations of no more than 5 mg/mL and rates of no more than 10 mg/min are recommended in adults (see also age-specific recommendations). In selected patients in need of fluid restriction, a concentration up to 10 mg/mL may be used; use of such higher concentrations may increase the risk of infusion-related events. Infusion-related events may occur, however, at any rate or concentration.
Patients with Normal Renal Function
Adults
The usual daily dose is 2 g divided either as 500 mg every six hours or 1 g every 12 hours. Each dose should be administered at no more than 10 mg/min, or over a period of at least 60 minutes, whichever is longer. Other patients factors, such as age or obesity, may call for modification of the usual intravenous daily dose.
Children
The usual intravenous dosage of vancomycin is 10 mg/kg per dose given every 6 hours. Each dose should be administered over a period of at least 60 minutes.
Infants and Neonates
In neonates and young infants, the total daily IV dosage may be lower. In both neonates and infants, an initial dose of 15 mg/kg is suggested, followed by 10 mg/kg every 12 hours for neonates in the first week of life and every eight hours thereafter up to the age of one month. Each dose should be administered over 60 minutes. Close monitoring of serum concentrations of vancomycin may be warranted in these patients.
Patients with Impaired Renal Function and Elderly Patients
Dosage adjustment must be made in patients with impaired renal function. In premature infants and the elderly, greater dosage reductions than expected may be necessary because of decreased renal function. Measurement of vancomycin serum concentrations can be helpful in optimizing therapy, especially in seriously ill patients with changing renal function. Vancomycin serum concentrations can be determined by use of microbiologic assay, radioimmunoassay, fluorescence polarization immunoassay, fluorescence immunoassay or high-pressure liquid chromatography.
If creatinine clearance can be measured or estimated accurately, the dosage for most patients with renal impairment can be calculated using the following table. The dosage of vancomycin per day in mg is about 15 times the glomerular filtration rate in mL/min (see following table).
DOSAGE TABLE FOR VANCOMYCIN IN PATIENTS WITH IMPAIRED RENAL FUNCTION
(Adapted from Moellering et al. 3 )
Creatinine Clearance Vancomycin Dose
_______mL/min mg/24 hr_____
100 1,545
90 1,390
80 1,235
70 1,080
60 925
50 770
40 620
30 465
20 310
10 155
The initial dose should be no less than 15 mg/kg, even in patients with mild to moderate renal insufficiency.
The table is not valid for functionally anephric patients. For such patients, an initial dose of 15 mg/kg of body weight should be given to achieve prompt therapeutic serum concentrations. The dose required to maintain stable concentrations is 1.9 mg/kg/24 hr. In patients with marked renal impairment, it may be more convenient to give maintenance doses of 250 to 1,000 mg once every several days rather than administering the drug on a daily basis. In anuria, a dose of 1,000 mg every 7 to 10 days has been recommended.
When only serum creatinine is known, the following formula (based on sex, weight and age of the patient) may be used to calculate creatinine clearance. Calculated creatinine clearances (mL/min) are only estimates. The creatinine clearance should be measured promptly.
Men: Weight (kg) x (140 – age in years)
72 x serum creatinine concentration (mg/dL)
Women: 0.85 x above value
The serum creatinine must represent a steady state of renal function or the estimated value for creatinine clearance will not be valid. Such a calculated clearance is an overestimate of actual clearance in patients with conditions: (1) characterized by decreasing renal function, such as shock, severe heart failure or oliguria; (2) in which a normal relationship between muscle mass and total body weight is not present, such as in obese patients or those with liver disease, edema, or ascites; and (3) accompanied by debilitation, malnutrition or inactivity.
The safety and efficacy of vancomycin administration by the intrathecal (intralumbar or intraventricular) route have not been assessed.
Intermittent infusion is the recommended method of administration.
Preparation and Stability
At the time of use, reconstitute vials of vancomycin with Sterile Water for Injection, USP to a concentration of 50 mg of vancomycin/mL. (See following table for volume of diluent.)
| Concentration/Vial | Volume of Diluent |
| 1 g | 20 mL |
After reconstitution, the vials may be stored in a refrigerator for 96 hours without significant loss of potency.
Reconstituted solutions of vancomycin (1 g/20 mL) must be further diluted in at least 200 mL of a suitable infusion solution. The desired dose diluted in this manner should be administered by intermittent IV infusion over a period of at least 60 minutes.
Compatibility with Other Drugs and IV Fluids
The following diluents are physically and chemically compatible (with 4 g/L vancomycin hydrochloride):
5% Dextrose Injection, USP
5% Dextrose Injection and 0.9% Sodium Chloride Injection, USP
Lactated Ringer’s Injection, USP
5% Dextrose and Lactated Ringer’s Injection
Normosol ® -M and 5% Dextrose
0.9% Sodium Chloride Injection, USP
Isolyte ® E
Good professional practice suggests that compounded admixtures should be administered as soon after preparation as is feasible.
Vancomycin solution has a low pH and may cause physical instability of other compounds.
Parenteral drug products should be visually inspected for particulate matter and discoloration prior to administration, whenever solution and container permit.
For Oral Administration
Oral vancomycin is used in treating antibiotic-associated pseudomembranous colitis caused by C. difficile and for staphylococcal enterocolitis. Vancomycin is not effective by the oral route for other types of infections. The usual adult total daily dosage is 500 mg to 2 g given in 3 or 4 divided doses for 7 to 10 days. The total daily dose in children is 40 mg/kg of body weight in 3 or 4 divided doses for 7 to 10 days. The total daily dosage should not exceed 2 g. The appropriate dose may be diluted in 1 oz of water and given to the patient to drink. Common flavoring syrups may be added to the solution to improve the taste for oral administration. The diluted solution may be administered via a nasogastric tube.
CONTRAINDICATIONS:
Vancomycin is contraindicated in patients with known hypersensitivity to this antibiotic.
ADVERSE REACTIONS:
Infusion-Related Events
During or soon after rapid infusion of vancomycin, patients may develop anaphylactoid reactions, including hypotension (see ANIMAL PHARMACOLOGY ), wheezing, dyspnea, urticaria, or pruritus. Rapid infusion may also cause flushing of the upper body (“red neck”) or pain and muscle spasm of the chest and back. These reactions usually resolve within 20 minutes but may persist for several hours. Such events are infrequent if vancomycin is given by a slow infusion over 60 minutes. In studies of normal volunteers, infusion-related events did not occur when vancomycin was administered at a rate of 10 mg/min or less.
Nephrotoxicity
Renal failure, principally manifested by increased serum creatinine or BUN concentrations, especially in patients administered large doses of vancomycin, has been reported rarely. Cases of interstitial nephritis have also been reported rarely. Most of these have occurred in patients who were given aminoglycosides concomitantly or who had pre-existing kidney dysfunction. When vancomycin was discontinued, azotemia resolved in most patients.
Gastrointestinal
Onset of pseudomembranous colitis symptoms may occur during or after antibiotic treatment (see WARNINGS ).
Ototoxicity
A few dozen cases of hearing loss associated with vancomycin have been reported. Most of these patients had kidney dysfunction or a pre-existing hearing loss or were receiving concomitant treatment with an ototoxic drug. Vertigo, dizziness, and tinnitus have been reported rarely.
Hematopoietic
Reversible neutropenia, usually starting 1 week or more after onset of therapy with vancomycin or after a total dosage of more than 25 g, has been reported for several dozen patients. Neutropenia appears to be promptly reversible when vancomycin is discontinued. Thrombocytopenia has rarely been reported. Although a causal relationship has not been established, reversible agranulocytosis (granulocytes <500/mm 3 ) has been reported rarely.
Phlebitis
Inflammation at the injection site has been reported.
Miscellaneous
Infrequently, patients have been reported to have had anaphylaxis, drug fever, nausea, chills, eosinophilia, rashes including exfoliative dermatitis, Stevens-Johnson syndrome, toxic epidermal necrolysis and vasculitis in association with administration of vancomycin.
Chemical peritonitis has been reported following intraperitoneal administration of vancomycin (see PRECAUTIONS ).
Post Marketing Reports
The following adverse reactions have been identified during post-approval use of vancomycin. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Skin and Subcutaneous Tissue Disorders
Drug Rash with Eosinophilia and Systemic Symptoms (DRESS)
DESCRIPTION:
Vancomycin Hydrochloride for Injection, USP is a lyophilized powder, for preparing intravenous (IV) infusions, in vials each containing the equivalent of 1 g vancomycin base. 500 mg of the base are equivalent to 0.34 mmol. When reconstituted with Sterile Water for Injection to a concentration of 50 mg/mL, the pH of the solution is between 2.5 and 4.5. Vancomycin Hydrochloride for Injection, USP should be administered intravenously in diluted solution (see DOSAGE AND ADMINISTRATION ). FURTHER DILUTION IS REQUIRED BEFORE USE.
Vancomycin is a tricyclic glycopeptide antibiotic derived from Amycolatopasis orientalis (formerly Nocardia orientalis ). Vancomycin hydrochloride has the following structural formula:
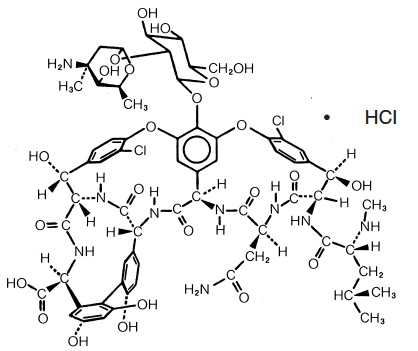
C 66 H 75 Cl 2 N 9 O 24 • HCl M.W. 1485.73
CLINICAL PHARMACOLOGY:
Vancomycin is poorly absorbed after oral administration.
In subjects with normal kidney function, multiple IV dosing of 1 g of vancomycin (15 mg/kg) infused over 60 minutes produces mean plasma concentrations of approximately 63 mcg/mL immediately at the completion of infusion, mean plasma concentrations of approximately 23 mcg/mL two hours after infusion, and mean plasma concentrations of approximately 8 mcg/mL 11 hours after the end of the infusion. Multiple dosing of 500 mg infused over 30 minutes produces mean plasma concentrations of about 49 mcg/mL at the completion of infusion, mean plasma concentrations of about 19 mcg/mL two hours after infusion, and mean plasma concentrations of about 10 mcg/mL six hours after infusion. The plasma concentrations during multiple dosing are similar to those after a single dose.
The mean elimination half-life of vancomycin from plasma is four to six hours in subjects with normal renal function. In the first 24 hours, about 75% of an administered dose of vancomycin is excreted in urine by glomerular filtration. Mean plasma clearance is about 0.058 L/kg/hr, and mean renal clearance is about 0.048 L/kg/hr. Renal dysfunction slows excretion of vancomycin. In anephric patients, the average half-life of elimination is 7.5 days. The distribution coefficient is from 0.3 to 0.43 L/kg. There is no apparent metabolism of the drug. About 60% of an intraperitoneal dose of vancomycin administered during peritoneal dialysis is absorbed systemically in six hours. Serum concentrations of about 10 mcg/mL are achieved by intraperitoneal injection of 30 mg/kg of vancomycin. Vancomycin is not effectively removed by either hemodialysis or peritoneal dialysis; there have been no reports of vancomycin clearance with hemoperfusion.
Total systemic and renal clearance of vancomycin may be reduced in the elderly.
Vancomycin is approximately 55% serum protein bound as measured by ultrafiltration at vancomycin serum concentrations of 10 to 100 mcg/mL. After IV administration of vancomycin inhibitory concentrations are present in pleural, pericardial, ascitic and synovial fluids; in urine; in peritoneal dialysis fluid; and in atrial appendage tissue. Vancomycin does not readily diffuse across normal meninges into the spinal fluid; but, when the meninges are inflamed, penetration into the spinal fluid occurs.
Microbiology
The bactericidal action of vancomycin results primarily from inhibition of cell-wall biosynthesis. In addition, vancomycin alters bacterial-cell-membrane permeability and RNA synthesis. There is no cross-resistance between vancomycin and other antibiotics. Vancomycin is not active in vitro against gram-negative bacilli, mycobacteria, or fungi.
Synergy
The combination of vancomycin and an aminoglycoside acts synergistically in vitro against many strains of Staphylococcus aureus, Streptococcus bovis, enterococci, and the viridans group streptococci.
Vancomycin has been shown to be active against most strains of the following microorganisms, both in vitro and in clinical infections as described in INDICATIONS AND USAGE .
Aerobic gram-positive microorganisms
Diphtheroids
Enterococci (e.g., Enterococcus faecalis )
Staphylococci, including Staphylococcus aureus and Staphylococcus epidermidis (including heterogeneous methicillin-resistant strains)
Streptococcus bovis
Viridans group streptococci
The following in vitro data are available, but their clinical significance is unknown.
Vancomycin exhibits in vitro MICs of 1 mcg/mL or less against most (≥90%) strains of streptococci listed below and MICs of 4 mcg/mL or less against most (≥90%) strains of other listed microorganisms; however, the safety and effectiveness of vancomycin in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled clinical trials.
Aerobic gram-positive microorganisms
Listeria monocytogenes
Streptococcus pyogenes
Streptococcus pneumoniae (including penicillin-resistant strains)
Streptococcus agalactiae
Anaerobic gram-positive microorganisms
Actinomyces species
Lactobacillus species
Susceptibility Tests
Dilution Techniques
Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized procedure. Standardized procedures are based on a dilution method 1 (broth or agar) or equivalent with standardized inoculum concentrations and standardized concentrations of vancomycin powder. The MIC values should be interpreted according to the following criteria:
For testing aerobic microorganisms a other than streptococci:
| MIC (mcg/mL) | Interpretation |
| ≤4 | Susceptible (S) |
| 8 to 16 | Intermediate (I) |
| ≥32 | Resistant (R) |
| a A ß-lactamase test using an inoculum ≥ 10 7 CFU/mL (or direct colony growth) and a nitrocefin-based substrate should be performed to detect either ampicillin or penicillin resistance among enterococci due to ß-lactamase production. | |
For testing streptococci a other than Streptococcus pneumoniae :
| MIC (mcg/mL) | Interpretation |
| ≤1 | Susceptible (S) |
| a Interpretative criteria applicable only to tests performed by broth microdilution method using cation-adjusted Mueller-Hinton broth with 2 to 5% lysed horse blood 1 . | |
The current absence of data on resistant strains precludes defining any categories other than “Susceptible”.
Strains yielding MIC results suggestive of a “nonsusceptible” category should be submitted to a reference laboratory for further testing.
A report of “Susceptible” indicates that the pathogen is likely to be inhibited if the antimicrobial compound in the blood reaches the concentrations usually achievable. A report of “Intermediate” indicates that the result should be considered equivocal, and, if the microorganism is not fully susceptible to alternative, clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where high dosage of drug can be used. This category also provides a buffer zone which prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of “Resistant” indicates that the pathogen is not likely to be inhibited if the antimicrobial compound in the blood reaches the concentrations usually achievable; other therapy should be selected. Standardized susceptibility test procedures require the use of laboratory control microorganisms to control the technical aspects of the laboratory procedures. Standard vancomycin powder should provide the following MIC values:
| Microorganism | MIC (mcg/mL) | |
| Enterococcus faecalis | ATCC 29212 | 1 to 4 |
| Staphylococcus aureus | ATCC 29213 | 0.5 to 2 |
| Streptococcus pneumoniae a | ATCC 49619 | 0.12 to 0.5 |
| a Interpretative criteria applicable only to tests performed by broth microdilution method using cation-adjusted Mueller-Hinton broth with 2 to 5% lysed horse blood 1 . | ||
Diffusion Techniques
Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. One such standardized procedure 2 requires the use of standardized inoculum concentrations. This procedure uses paper disks impregnated with 30-mcg vancomycin to test the susceptibility of microorganisms to vancomycin.
Reports from the laboratory providing results of the standard single-disk susceptibility test with a 30-mcg vancomycin disk should be interpreted according to the following criteria:
For testing aerobic microorganisms other than enterococci and streptococci:
| Zone Diameter (mm) | Interpretation |
| ≥15 | Susceptible (S) |
| - | Intermediate (I) |
| - | Resistant (R) |
For testing enterococci a,b :
| Zone Diameter (mm) | Interpretation |
| ≥17 | Susceptible (S) |
| 15 to 16 | Intermediate (I) |
| ≤14 | Resistant (R) |
| a A direct nitrocefin-based ß-lactamase test using direct colony growth should be performed to detect either ampicillin or penicillin resistance among enterococci due to ß-lactamase production. | |
| b When testing for enterococci resistance to vancomycin, plates should be held for a full 24 hours and examined using transmitted light. The presence of a haze or any growth within the zone of inhibition indicates resistance. Those enterococci with intermediate zones of inhibition should be tested by a standardized procedure based on a dilution method 1 (broth or agar) or equivalent. | |
For testing streptococci a other than Streptococcus pneumoniae :
| Zone Diameter (mm) | Interpretation |
| ≥17 | Susceptible (S) |
| a Interpretative criteria applicable only to tests performed by disk diffusion method using Mueller-Hinton agar with 5% defibrinated sheep blood and incubated in 5% CO 2 2 . | |
The current absence of data on resistant strains precludes defining any categories other than “Susceptible”. Strains yielding zone diameter results suggestive of a “nonsusceptible” category should be submitted to a reference laboratory for further testing.
Interpretation should be as stated above for results using dilution techniques. Interpretation involves correlation of the diameter obtained in the disk test with the MIC for vancomycin.
As with standardized dilution techniques, diffusion methods require the use of laboratory control microorganisms that are used to control the technical aspects of the laboratory procedures. For the diffusion technique, the 30-mcg vancomycin disk should provide the following zone diameters in these laboratory test quality control strains:
| Microorganism | Zone Diameter (mm) | |
| Staphylococcus aureus | ATCC 25923 | 17 to 21 |
| Streptococcus pneumoniae a | ATCC 49619 | 20 to 27 |
| a Interpretative criteria applicable only to tests performed by disk diffusion method using Mueller-Hinton agar with 5% defibrinated sheep blood and incubated in 5% CO 2 2 . | ||
HOW SUPPLIED:
| Product No. | NDC No. | |
| 28421 | 63323-284-21 | Vancomycin Hydrochloride for Injection, USP equivalent to 1 g vancomycin in a 20 mL flip-top vial, in packages of 10. |
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature].
The container closure is not made with natural rubber latex.